



Microcornea is defined as an adult cornea that is less than 10mm in diameter. It is most commonly noted as being sporadic and occurs in conjunction with microphthalmia, congenital cataracts, iris colobomas, optic atrophy, and microcephaly.
Patients present with high hyperopic prescriptions secondary to a flat anterior corneal curvature. In cases of concurrent anterior segment pathologies, surgical intervention such as cataract extraction can improve visual prognosis by preventing deprivation amblyopia.
Intervention and correction of microcornea
Cataract surgery is an early intervention that can help reduce amblyopia secondary to visual deprivation. Visual rehabilitation in children with cataract surgery requires optical correction through glasses, contact lens (CL) management, or intraocular lens (IOL) implantation to improve the likelihood of binocularity.1
Of note, 50% of patients with unilateral cataracts develop vision better than 20/200 with early intervention.1 However, IOL implantation still remains controversial in infants. While IOLs do provide the advantage of vision correction, infants require smaller diameter IOLs, which increases the risk of lens subluxation, endothelial cell loss, and posterior capsular opacification in the growing eye.2-4
Microcornea treatment outcomes for CLs, spectacles, and IOL implantation
The Infant Aphakia Treatment Study also noted that the mean visual acuity was similar across patients treated with contact lenses versus IOL.4,5 However, at 4.5 years of age, twice as many eyes in the contact lens cohort had better than 20/40 acuity. One of the reasons in such cases that patients are left aphakic is to reduce post-operative complications.4,5
Spectacle correction is possible in some situations, however, in patients with unilateral aphakia, spectacles are no longer an option secondary to concerns with aniseikonia. In addition, there is an induced prismatic imbalance that results from marked anisometropia.6,7
Specialty contact lenses can play a crucial role in visual rehabilitation and improving visual prognosis for children with aphakia. Traditionally, soft contact lenses (hydrogel and silicone hydrogel) are most commonly used in pediatric aphakia.
Rigid gas permeable (RGP) lenses, such as corneal RGPs, can provide an added advantage for correcting irregular astigmatism. In addition, with the advances in technology, lens materials such as Boston XO (Dk of 100 Barrer) or Fluoroperm 151 (Dk of 151 Barrer) are able to satisfy the Holden-Mertz criteria for oxygen transmissibility for daily and overnight lens wear even with high plus powers.6
Glaucoma as a key risk factor for microcornea
Glaucoma is one of the risk factors for microcornea and aphakia. It has been reported that the prevalence of microcornea in aphakic glaucoma patients has been as high as 88.5 to 94%.8-10 Mills et al. demonstrated a bimodal pattern of onset of glaucoma following cataract surgery.11
Early onset glaucoma a few months after cataract surgery is a result of angle closure, whereas delayed onset glaucoma is commonly from open-angle glaucoma.11 Additionally, early onset glaucoma after cataract surgery is most commonly a result of a pupillary block with secondary angle closure.
Residual lens material in the anterior chamber triggers the formation of Elsching’s pearls that physically block the pupils and induce inflammatory adhesions in the angle and pupil edge.12-15
Glaucoma post-cataract surgery
Late-onset glaucoma after cataract surgery is a result of open-angle glaucoma as there is an altered development of the filtration angle. Evidence indicates there is an anterior insertion of the iris and a lack of development of angle recess.2,12,13,16 Routine monitoring is required for early diagnosis and intervention of glaucoma.
However, post-cataract surgery, aphakia can result in significant anisometropia. Glasses usually do not address concerns with aniseikonia, and contact lenses may provide a feasible option to correct for high hyperopia prescriptions while combating concerns of aniseikonia.
Specialty contact lenses, such as custom soft contact lenses and corneal gas permeable (GP) lenses are a great resource and can help with improving visual quality and visual potential.
Microcornea case study
A 5-year-old female presented to the eye clinic in 2009 for a corneal rigid gas permeable contact lens refitting for the right eye (OD). The patient had a longstanding history of microphthalmia with microcornea, congenital cataract, constant esotropia, and dissociated vertical deviation OD.
The patient underwent iridectomy and cataract surgery, resulting in aphakia, corectopia, as well as strabismus surgery in the right eye (Figure 1). Specifically right lateral rectus and right medial rectus transposition to correct the esotropia.
A treatment of atropine 1% every morning OD and patching OS for 4 to 5 hours was initiated to prevent amblyopia by the ophthalmologist. The patient had been wearing a corneal GP contact lens on the right since her cataract surgery.
Figure 1 illustrates microcornea with corectopia, dyscoria, and aphakia in the patient’s right eye.

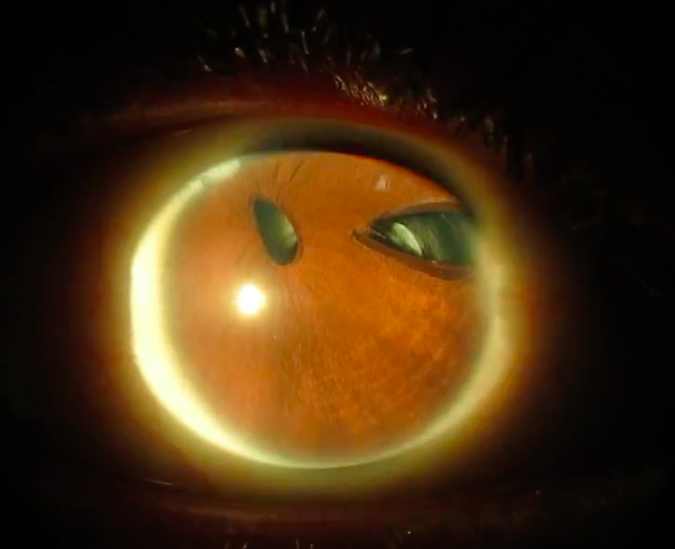
Figure 1: Courtesy of Manveen Bedi, OD, FAAO, FSLS.
Microcornea patient workup
The patient presented for refitting of corneal GP contact lenses at the eye clinic. In 2009, her presenting visual acuity at distance was 20/40- with corneal GP contact lens OD and 20/20 in the left eye (OS) with no correction. No pertinent family ocular and medical history were reported.
The right eye pupil had corectopia, and the left eye pupil was round. No relative afferent pupillary defect was noted. Visual fields were full with finger counting in each eye. Extraocular motility was full in both eyes, and a cover test revealed dissociated vertical deviation OD and a slight left hypertropia.
Manifest refraction was performed over the habitual GP lens with unknown parameters, and an over-refraction of +6.75-0.50x180 was documented with a visual acuity of 20/40 OD. There was suspicion that the patient was not prescribed full plus, and the vision in the amblyopic eye had plateaued. The left eye had a manifest refraction of +2.75DS with a visual acuity of 20/25.
Retinoscopy was performed over the right eye without the GP lens, and a power of +16.00-0.50x045 was noted. The goal of the fitting was to prescribe a full hyperopic prescription to maximize visual outcomes in the amblyopic eye and continue with patching.
Pertinent findings from the workup
Slit lamp examination revealed clear lids, lashes, and tear film as well as white and quiet bulbar and palpebral conjunctiva in both eyes. Corectopia and iridectomy were noted in the right eye. Anterior segment findings in the left eye were unremarkable.
Fluorescein sodium was instilled in both eyes, and no corneal staining was noted in either eye. Intraocular pressures were measured at 18mmHg OD and 16mmHg OS. A dilated exam was performed using tropicamide 1%.
Posterior pole findings were unremarkable, with a cup-to-disc ratio of 0.2/0.2 in each eye. Optic nerve margins were distinct, with a healthy neuroretinal rim tissue OU. The macula was flat and avascular, with the presence of a normal foveal reflex in both eyes. No pertinent findings were noted on peripheral retinal examination.
An initial corneal GP lens was ordered with best-corrected vision at 20/40 with the following parameters OD:
- Base curve (BC): 44.06D (7.66mm)
- Diameter: 9.0mm
- Power: +19.50DS
- Optical zone (OZ): 7.4
- Secondary curve: 8.36
- Peripheral curve: 12.00
- Center thickness: 0.45
- Design: (-) edge lenticulation
- Material: Fluoroperm 60/Blue
Microcornea patient long-term findings
The patient was followed over the course of 10 years with corneal gas permeable lenses and patching. A significant shift in the clinical data was noted. Best-corrected visual acuity with patching and the use of corneal GP lenses improved from 20/40- to 20/20-2 OD in 10 years. Left eye vision was stable at 20/20 over the course of 10 years.
Topography was performed in 2012, and simulated keratometry (sim-K) values were noted as 38.10/43.73D @ 133 OD with inferior temporal steepening and 41.40/42.60D @ 91 OS (Figure 2). In 2018, simulated keratometry values were recorded as 36.90/42.72D @ 134 with stable inferior temporal steepening OD and 41.00/42.31D @ 82 OS (Figure 3).
As is evident in Figure 2, topography performed in 2012 with observed simulated keratometry produced a measurement of 38.10/43.73D @ 133 OD with inferior temporal steepening. A slight with-the-rule pattern was noted in the left eye with simulated keratometry as 41.40/42.60D @ 91.

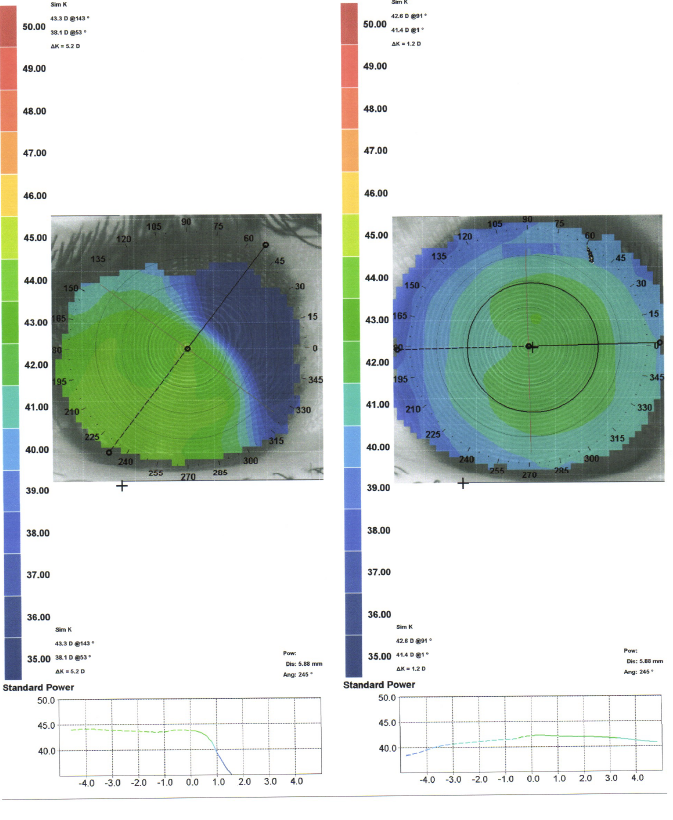
Figure 2: Courtesy of Manveen Bedi, OD, FAAO, FSLS.
Figure 3 demonstrates topography performed in 2018 with observed simulated keratometry measurement as 36.90/42.72D @ 134 OD with inferior temporal steepening. A with-the-rule pattern of astigmatism was noted with simulated keratometry as 41.00/42.31D @ 82 OS.

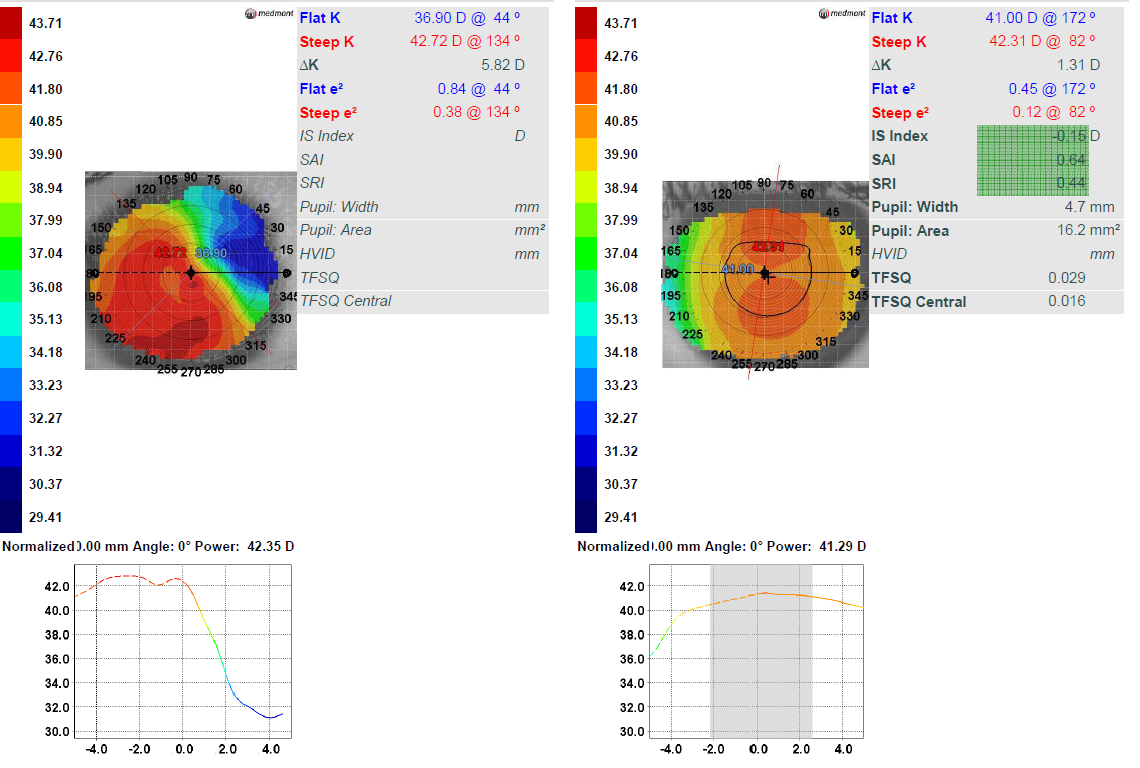
Figure 3: Courtesy of Manveen Bedi, OD, FAAO, FSLS.
Corneal GP contact lens modifications
In 2018, the corneal GP contact lens parameters were modified to account for over-refraction of -3.00D with the presenting GP lens and to flatten the lens for better alignment overall.
The finalized parameters were as follows OD:
- BC: 43.00D (7.85mm)
- Diameter: 9.2mm
- Power: +17.25DS
- Secondary curve: 9.75
- Peripheral curve: 12.00 x 0.2
- Optic zone diameter (OZD): 7.8
- Design: Lenticular, optic cap=OZD
- Material: Boston Extra/green
For every 0.05mm change in base curve, the power needs to be adjusted 0.25D per the SAM/FAP (steep add minus, flat add plus) rule. In this case, since the base curve was flattened 1D (0.19mm) and power was compensated, the OZD was increased by 0.4mm, which increased the sagittal height of the lens.
As a result, this steepened the lens and altered the base curve by 0.05mm with a power change of 0.25D. Therefore, it was accounted for during the modification. A lenticular design was used to reduce the mass of the lens and bring the center of gravity closer to the cornea to help with lens centration.
Normally, a lenticular design is used for all plus power prescriptions to aid lid interaction with increased edge thickness. The optic cap diameter was matched with the optic zone to allow for better contact lens centration while maintaining visual quality. In primary gaze, the lens was lid attached with trace apical clearance. The lens demonstrated sufficient peripheral clearance with good movement.
When eyelids were pulled away to assess the lens, it was inferiorly decentered with apical clearance and sufficient edge clearance (Figure 4). Visual acuity was recorded as 20/20-2 OD with the corneal gas permeable lens.
Figure 4 depicts the corneal gas permeable lens fitting in the right eye with lids interaction (picture on the left) and when eyelids are pulled away (picture on the right).

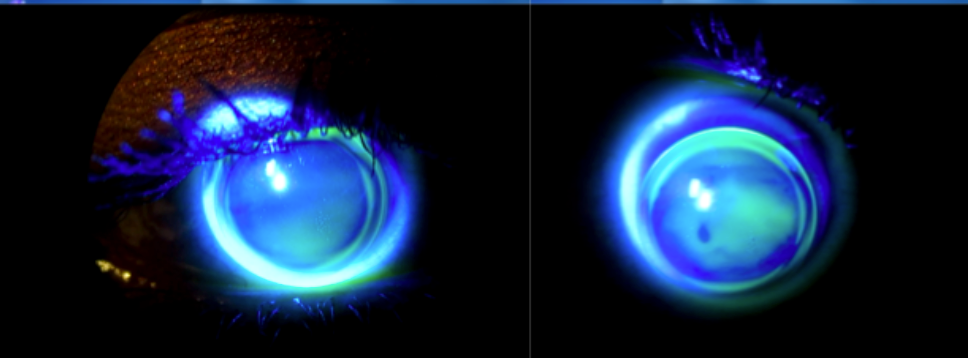
Figure 4: Courtesy of Manveen Bedi, OD, FAAO, FSLS.
Management of microcornea
Microcornea is often associated with other ocular abnormalities such as optic nerve hypoplasia, scleroderma, cataracts, iris abnormalities, and glaucoma. All of these ocular co-morbidities pose a limitation on visual prognosis.
In the pediatric population, where patients are undergoing critical periods of visual development, it is crucial to intervene early with optical correction with contact lenses to minimize adverse effects. In addition, patching with long-term vision monitoring is important to ensure that there is improvement in visual outcomes.
Corneal curvature has been reported to be steeper in infants and normally stabilizes to adult keratometric readings by 3 years of age.17,18 There is limited data on the stabilization of corneal curvatures in patients with microcornea due to differences in the severity of co-morbidities.
Soft contact lenses, such as Silsoft, are a great option for aphakic patients, however, as the patient history gets complex with corneal irregularity, a gas permeable option may be a suitable option to maximize visual outcomes. Corneal GP lenses have the advantage of good tear exchange underneath the lens surface, which can reduce hypoxia-related concerns with high refractive errors and thicker lens profiles.
Scleral lens use might be complicated in infants due to application and insertion concerns; however, a fenestrated scleral lens may be an option if there are stability and centration issues with corneal GP lenses.
In closing
Long-term management of microcornea with congenital cataracts necessitates cataract surgery and co-management with specialty contact lenses for optimizing visual benefit.
