Eyes On Dry Eye 2023 provided eyecare professionals with the latest research and education, live sessions, and interactive Q&As with renowned specialists. Attendees could earn up to 7 hours of free COPE-accredited CE on topics directly related to patient care, including how to get started with a dry eye practice, learning about the most promising treatments in the pipeline, and many more.
Enjoy this presentation from William Trattler, MD, and Ahmad Fahmy, OD, FAAO, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
The speakers, Ahmad Fahmy, OD, FAAO, and William Trattler, MD, discussed how to recognize treatment challenges and side effects related to the treatment of OSD and co-morbid disease. They also identified important ocular co-morbid conditions and factors that can complicate
OSD assessment and treatment.
Over the years, both speakers have developed protocols to narrow down ocular co-morbidities that are often the culprits for patients with persisting symptoms in order to improve the patient’s quality of life and get a subjective improvement in symptoms.
Listen to the full lecture from Drs. Fahdy and Trattler!
Sign up for our newsletter to watch the full recording and to register for more Eyes On events.
Overview of the 4 kinds of ocular surface disease
The four main characteristics of OSD include evaporative, aqueous deficiency, inflammation, and obstruction. These features of dry eye tend to overlap; for example, an aqueous deficiency causes inflammation, and in turn, inflammation can lead to a reduction in aqueous tears.
When creating a treatment plan, it is important to consider all of these factors and decide how to best devise a comprehensive treatment plan.
Identifying and treating patients with corneal neuropathic pain
For patients with
corneal neuropathic pain, often their eyes will present normally, but they report discomfort, irritation, burning, or foreign body sensation, as the corneal nerve response to sensation, temperature, and pressure is altered.
“Disruption of the corneal nerves can lead to attrition or aberrant regrowth of those corneal nerves.”
However, in the case of neurotrophic keratitis, with staining and rapid tear breakup time (TBUT), you can see that their corneas are very dry, but the patients will often report that their eyes feel fine. Identifying these traits early on is important because, over time, they can negatively impact a patient’s quality of life.
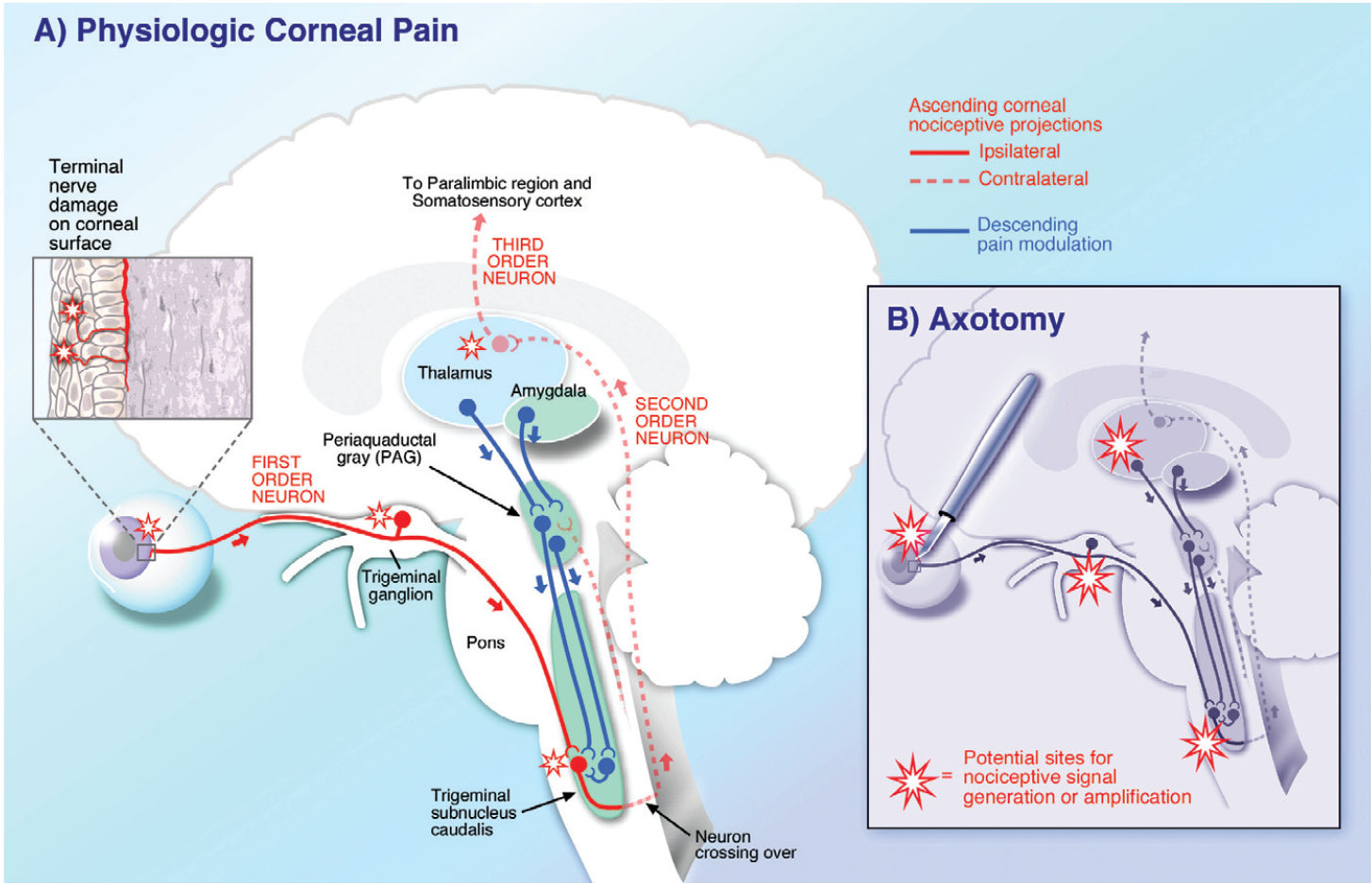
Figure 1 outlines the pathophysiology of corneal neuropathic pain.
Figure 1: Courtesy of Perry Rosenthal, MD
The value of peripheral findings when treating patients
A patient seen by Dr. Fahmy with ocular surface disease reported that she was mostly bothered by symptoms of dryness and irritation, with ongoing hemifacial spasms. Her medical history included treatment for the blepharospasms with
Botox injections. After an examination, Dr. Fahmy observed that the patient had an incomplete blink and diagnosed her with another co-morbid condition: conjunctivochalasis.
Dr. Trattler saw a patient with similar findings who also had conjunctivochalasis, which led to further ocular surface inflammation and mechanical dry eye. The patient required patching during the night to treat the exposure. He observed that the conjunctivochalasis and also damage to the lash line were potentially caused by the repeated use of
eyelash extensions.
While subtle peripheral findings might not be the main source of the patient’s complaints, they can still play an important role in their experience. It’s important to note that blepharospasm treatments need to be carefully titrated when treating OSD patients because it can increase exposure.
The staged management and treatment of dry eye disease (DED)
Dr. Tattler mentioned that the most common treatment that he uses for dry eye patients is
topical steroids for a short pulse of twice a day for 3 to 4 weeks, as they tend to treat multiple factors of OSD, including evaporative, aqueous deficiency, and reducing inflammation.
Comparing treatments for dry eye disease
For patients with symptoms stemming from
meibomian gland dysfunction (MGD), aqueous deficiency, evaporative dry eye with MGD issues, or blepharitis, leaning toward a hypochlorous acid spray a couple of times a day to kill the bacteria impacting the meibomian gland secretions has proven helpful. Patients with evaporative dry eye also tend to benefit from topical cyclosporine-based treatments, lifitegrast, or punctal plugs.
Dr. Tattler expressed that he tends to lean towards prescribing DED patients a hypochlorous acid spray with heating compresses or other heating therapies, such as Lipiflow or TearCare, as MGD patients have responded very well to this treatment protocol.
Establishing a workflow for treating and managing OSD
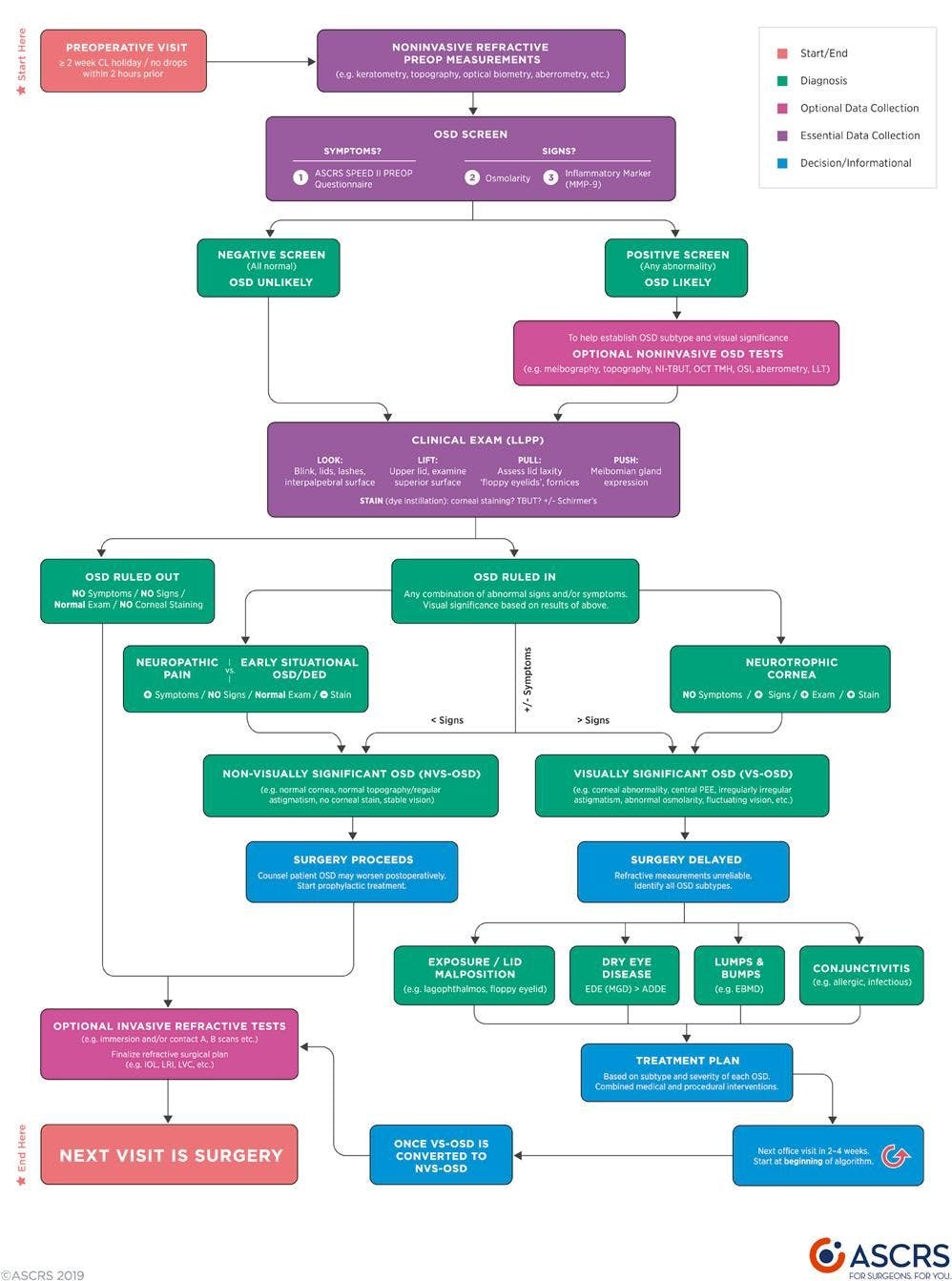
Determining a workflow for treating OSD patients is key to accurately identifying, diagnosing, and treating the condition. Dr. Fahmy expressed that the “look, lift, pull, push” recommendation from the
Preoperative OSD Algorithm by the American Society of Cataract and Refractive Surgery (ASCRS) is very helpful in identifying OSD patients, especially those with MGD.
Figure 2 features the ASCRS preoperative ocular surface disease algorithm.
Figure 2: Courtesy of ASCRS Understanding the results of the PHACO study
The
PHACO study, led by Dr. Trattler, was a multicenter, observational study that included 136 patients (>55 years of age) undergoing cataract surgery. The incidence and severity of DED were measured per the International Task Force scale.
While researchers initially expected to see a 15% prevalence of DED in patients undergoing cataract surgery, the data showed that the prevalence was in fact much higher. Many patients in the study were asymptomatic but showed central corneal staining. This study showed that self-reported symptoms are not enough to identify and diagnose dry eye; it also requires corneal staining and corneal epithelial assessment because it is such a prevalent ocular condition.
The PHACO study found that:
- More than 60% of patients had a tear breakup time of <5 seconds
- Almost 80% of eyes had positive corneal staining
- 50% of the eyes had positive central corneal staining
- 18% had a Schirmer score (with anesthesia) of <5mm
Some patients will undergo
cataract surgery and come back to their eyecare provider frustrated that their eyes feel uncomfortable after the procedure, and they think it is a result of the cataract surgery. However, this occurs because the patient had pre-existing dry eye, and there is now short-term exacerbation by the cataract surgery, so the patient’s symptoms feel worse.
Protocols for identifying ocular surface disease prior to surgery
Performing a thorough
preoperative evaluation is key to identifying ocular surface disease in patients prior to any kind of ocular surgery.
Dr. Tattler explained that in his practice, meibography is not a default part of the preoperative evaluation; however, if the results of the exam point to potential MGD, meibography and meibomian gland assessment work well to identify the problem. Checking the patients’ oil gland production is a vital part of a preoperative evaluation.
Prior to ocular surgery, ECPs should make note of:
- A soft refractive endpoint is a big red flag
- OSD evaluation before ocular surgery
- OSD re-evaluation if unexpected symptoms arise before enhancement
OSD caused by limbal stem cell deficiency
A condition that can feel like a puzzle to identify and diagnose is limbal stem cell deficiency (LSCD). These patients have often undergone initial treatments for
dry eye but are unable to get rid of the foreign body sensation and symptoms of recurrent erosion.
“Limbal stem cells (LSCs) are vital to the ocular surface and the overall health of the cornea.”
They act by maintaining the integrity of the corneal surface and transparency of the cornea and acting as a barrier to the invasion of conjunctival epithelial cells onto the clear cornea. The disruption of the limbal niche environment eventually leads to neovascularization within the corneal epithelium and stroma, as well as scarring and corneal staining with epithelial thinning in a hallmark vortex pattern.
It is critical to identify this condition early, as a
corneal transplant will not be successful until the limbal stem cells are restored.
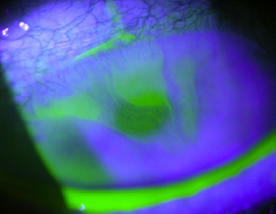
Figure 3 is a clinical image of corneal staining in the hallmark vortex pattern epitheliopathy associated with limbal stem cell deficiency patients.
Takeaways for treating limbal stem cell deficiency
Limbal stem cell deficiency can be a difficult condition to treat, Dr. Tattler recommended using punctal plugs to raise the tear volume and topical anti-inflammatory drugs. Some patients may benefit from
amniotic grafts for further anti-inflammatory treatment.
The goal is to medically supplement the tear film to get the limbal stem cells available to repopulate and grow into the area where they are missing. However, sometimes you won’t get enough improvement with just medical treatments, so stem cell transplant surgery is required.
Final thoughts
Treating ocular surface disease requires having a broad understanding of DED, as dryness is a common co-morbidity for other
systemic and ocular conditions.
“It’s always important to balance polypharmacy in patients with multiple co-morbidities.”
To navigate the waters of treating OSD, remember to follow your protocol with complex diseases and try to match symptoms to the main factors. Also, make sure to pay careful attention to patients with an incomplete blink, blepharospasms, conjunctival chalasis, limbal stem cell deficiency, and epithelial basement membrane dystrophy (EBMD).