



Although childhood glaucoma is a relatively rare disease, a missed or delayed diagnosis can have a profound impact on a child’s development. Early recognition, appropriate monitoring, and timely intervention are necessary to optimize visual potential in patients with childhood glaucoma.
There are two main types of primary childhood glaucoma that tend to present in children: primary congenital glaucoma and juvenile open-angle glaucoma. We will review both below.
Primary congenital glaucoma
Primary congenital glaucoma (PCG) is the most common form of primary childhood glaucoma. Although rare, PCG can cause multifactorial visual deficits in children and has been quoted as being responsible for 5% of blindness in children worldwide.1
Epidemiology of primary congenital glaucoma
The incidence of PCG has been reported as high as 1 in 1,250 live births in populations of Eastern Europeans and as low as 1 in 20,000 live births in Western countries. It is more common in children from consanguineous relationships and is frequently, but not uniformly, bilateral in presentation.2
Etiology of PCG
Most cases of PCG are sporadic. In familial cases, the inheritance pattern is typically autosomal recessive, although there have been reports of autosomal dominant inheritance patterns.3,4 Linkage analyses have identified five genetic loci that are associated with PCG: GLC3A, GLC3B, GLC3C, GLC3D, and GLC3E.1,5
The intraocular pressure (IOP) elevation seen in PCG is commonly attributed to an interruption in normal aqueous outflow due to abnormalities in the anterior segment of the eye, more specifically, the trabecular meshwork and angle of the anterior chamber.
Presentation of primary congenital glaucoma
In addition to elevated IOP, the classic “triad” of symptoms of congenital glaucoma include epiphora, photophobia, and blepharospasm—though these are found in <20% of referrals for PCG.
PCG may present at a variety of ages:
- Newborn onset (0 to 1 month of age)
- Infantile onset (between 1 to 24 months of age)
- Late-onset or late-recognized (>24 months of age)
Due to the elasticity of a child’s eye, the elevated IOP leads to enlargement of the eye, termed “buphthalmos,” which, in addition to corneal clouding, represents the more common reasons for referral.
Figure 1 illustrates a pediatric patient with bilateral buphthalmos secondary to primary congenital glaucoma.


Figure 1: Courtesy of Courtney Kraus, MD.
Figure 2 depicts unilateral buphthalmos of the left eye that is evident in a pediatric patient with unilateral PCG.


Figure 2: Courtesy of Courtney Kraus, MD.
Potential sequelae of primary congenital glaucoma
This rapid stretching of the eye causes the aforementioned triad of symptoms, which are byproducts of the corneal enlargement (>12mm less than 1 year of age or >13mm at any age), and horizontal breaks in Descemet’s membrane, termed Haab striae. This may lead to corneal edema, opacification, and scarring and ultimately result in amblyopia and even blindness if intervention and pressure control do not occur promptly and appropriately.
Figure 3 shows a pediatric patient with corneal edema caused by PCG.

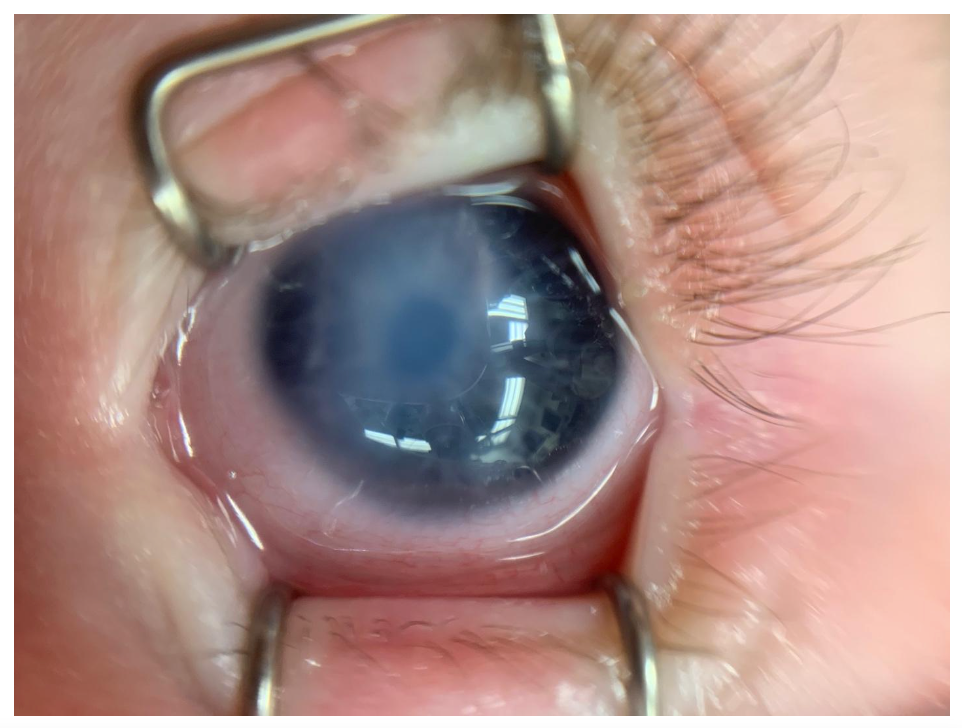
Figure 3: Courtesy of Courtney Kraus, MD.
These findings represent a key distinction separating childhood from adult-onset glaucoma. The Childhood Glaucoma Research Network and World Glaucoma Association in 2013 defined childhood glaucoma as IOP-related damage to the eye, which may manifest with buphthalmos, corneal edema, or progressive axial length elongation, as compared to the more commonly-known adult-onset glaucoma, which is defined as IOP-related damage to the optic nerve.3
Additional signs of stretching or enlargement of the eye due to elevated IOP include an abnormally deep anterior chamber, progressive myopia out of proportion to that expected for age, anisometropia, and optic nerve cupping. In children presenting with the above constellation of symptoms, as well as other ocular or systemic abnormalities, PCG is less likely and secondary childhood glaucomas must be considered.
Diagnostic tests for primary congenital glaucoma
The most important clinical diagnostic test for primary congenital glaucoma is a reliable measurement of IOP. In many children, an accurate IOP measurement may be obtained during the clinic visit, especially if the child is calm, sleeping, feeding, distracted, or old enough. However, in some situations, patients may be uncooperative and crying, and an exam under anesthesia may be required to obtain an IOP measurement as well as perform several other of the diagnostic tests listed below.
During an exam under anesthesia, IOP should be measured immediately upon or as soon as possible after induction of anesthesia prior to intubation, as the volatile anesthetics used can have effects on IOP. Typically, IOP measurements in PCG are greater than 20 mmHg and often in the range of 30 to 40 mmHg.
“Asymmetric IOP measurements, especially in a calm or anesthetized child, should also raise concern for glaucoma.”
Additional diagnostics include anterior examination (slit lamp, portable slit lamp, or pen light), optic nerve exam, corneal pachymetry, gonioscopy, serial axial length measurements, and cycloplegic refraction, which will often reveal myopia and astigmatism. The cornea should be examined for size, clarity, and the presence of Haab striae, which are best visualized on retroillumination.
In most patients with PCG, the cup-to-disc ratio (CDR) is often greater than 0.3. Asymmetry of cup-to-disc appearance between fellow eyes greater than 0.2 may also be suggestive of glaucoma. Formal visual field testing and optical coherence tomography (OCT) imaging should be obtained to help follow disease progression once the child is old enough to participate in testing.
Figure 4 highlights an example of measuring corneal diameter in a glaucoma suspect.

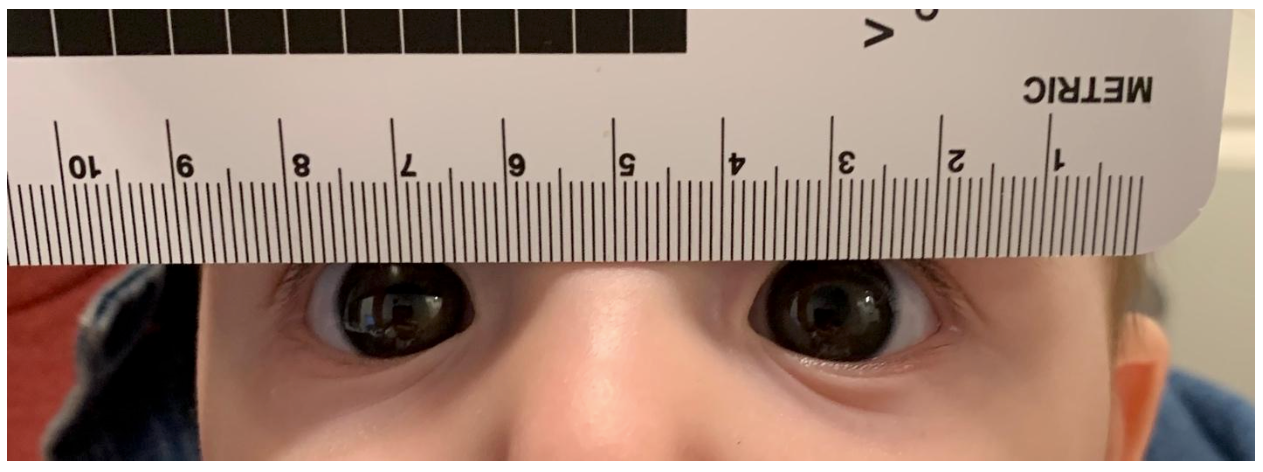
Figure 4: Courtesy of Courtney Kraus, MD.
Juvenile open-angle glaucoma
Juvenile open-angle glaucoma (JOAG) is a rare form of early-onset open-angle glaucoma, presenting between 3 and 40 years of age. Reports of the estimated prevalence of JOAG range between 0.4 and 2 in 100,000 persons between the ages of 4 and 20 years.6–8
It is inherited in an autosomal dominant fashion with high penetrance and has been linked to the GLC1A myocilin (TIGR/MYOC) gene.6,7 Mutations in myocilin are thought to occur in up to 36% of individuals with JOAG, with a lifetime risk of developing glaucoma in myocilin mutation carriers of 60 to 100%.9,10
Presentation of JOAG
Patients typically lack the corneal enlargement and Haab striae seen in PCG. It is hypothesized that JOAG occurs due to abnormalities in the trabecular meshwork that restrict aqueous outflow.6 As compared to adult-onset open-angle glaucoma, JOAG tends to be more rapidly progressive, marked by more severe elevations in IOP, and often requires surgical therapy as it tends to be refractory to maximum tolerated medical therapy.
A significant number of patients with JOAG are asymptomatic, and accordingly, JOAG is often diagnosed late, after advanced optic nerve damage has already occurred.11
Diagnostic tests for juvenile open-angle glaucoma
The diagnostics for patients with JOAG are similar to those for children with PCG, although patients are often older and more able to participate in the examination and formal visual field and OCT testing in the clinic. Patients should be asked about a family history of glaucoma, and their family members (especially younger siblings) should be screened for glaucoma.
Medical and surgical management of pediatric glaucoma
Surgical management of pediatric glaucoma
Both PCG and JOAG often require surgical intervention. PCG is often effectively treated with angle surgery, such as goniotomy or trabeculotomy. In goniotomy, an incision is made in the trabecular meshwork under direct visualization of the angle, whereas in a trabeculotomy, Schlemm’s canal is cannulated via an external approach and connected to the anterior chamber by incising a small portion of the trabecular meshwork.
Both goniotomy or trabeculotomy can be performed if the patient has a clear cornea. If the view through the cornea is difficult, a trabeculotomy is typically preferred, as goniotomy requires a relatively clear cornea to visualize the trabecular meshwork. Angle procedures are often highly effective for patients with PCG, and if the first angle surgical procedure is not sufficient, then a second angle procedure is often performed prior to considering other types of surgical interventions, such as trabeculectomy, tube shunt implantation, or cyclodestructive procedures.3,12–16
Surgical management of juvenile open-angle glaucoma
In JOAG, a mainstay of treatment has traditionally been glaucoma filtration surgery, with trabeculectomy being the most common. However, eyes with JOAG often have a robust healing response after filtration surgery that can cause bleb failure.17–19 Furthermore, the presence of a bleb may prove troublesome in a young patient who may desire to wear contact lenses, play contact sports, or live, work, or play in environments that predispose to infection.
Glaucoma drainage implants have been used as an alternative surgical intervention for JOAG, especially in the setting of significant scarring of the conjunctiva.20,21 Although angle surgeries are used most commonly in the setting of PCG, there is increasing evidence of successful angle surgery in the management of JOAG, in particular involving 360-degree trabeculotomy and goniotomy-assisted transluminal trabeculotomy (GATT).22,23
When IOP is normalized after the intervention, there may be a reversal of cupping noted, especially in young children. However, any damage that may have occurred to the retinal nerve fiber layer secondary to the elevated IOP is permanent.
Figure 5 is an intraoperative image of a direct gonioscopy view during angle surgery in a patient with JOAG.


Figure 5: Courtesy of Courtney Kraus, MD.
Medical management of pediatric glaucoma
In general, medical therapy for childhood glaucoma is typically less successful than that for adult-onset open-angle glaucoma. In childhood glaucoma, however, medical therapy can play an important role in lowering IOP prior to surgery in both JOAG and PCG, the latter of which benefits from efforts to reduce corneal edema secondary to the elevated IOP to optimize the view through the cornea during surgery.
IOP-lowering medications, whether topical or systemic, may also be used after surgery to help augment the IOP-lowering effect.24 Similarly, medical therapy can often be used as a bridge to adjunctive surgical intervention in JOAG.
Topical medications to treat JOAG
Among the topical medications, therapy with beta-blockers have been shown to be most efficacious in IOP-lowering, although their use may be limited by the risk of bronchospasm, apnea, and bradycardia. Topical carbonic-anhydrase inhibitors and prostaglandin analogs are often well-tolerated.
Of note in this age group of patients, while alpha-2-adrenergic agonists such as apraclonidine and brimonidine may effectively reduce IOP, both medications carry a significant risk of somnolence and respiratory depression in young children. Accordingly, the alpha-2-adrenergic agonists should be used with caution in children less than 6 years of age and are contraindicated in children less than 2 years of age.
Pediatric glaucoma prognosis
The prognosis in terms of visual outcome and IOP control is worst for patients with PCG who present at birth, with over half of patients eventually becoming legally blind despite intervention. Prognosis in PCG is most favorable in infantile-onset PCG, wherein the IOP can be controlled in 90% of patients between surgical and medical interventions.25
“In JOAG, prognosis is favorable for patients who are diagnosed and treated early in the disease course.”
Even in individuals with advanced damage from JOAG, often due to a delay in diagnosis, the patient's visual field loss can be stopped, and IOP can often be controlled with surgical intervention.26 Vision loss due to childhood glaucoma may result from optic nerve damage due to elevated IOP in both JOAG and PCG, as well as from corneal scarring, myopic astigmatism, or anisometropic amblyopia that tend to occur more commonly with PCG.
Children with childhood glaucoma, as well as children who may be childhood glaucoma suspects, require diligent follow-up and ongoing life-long monitoring and management to optimize visual outcomes.
