



While an acquired cataract is most commonly seen in aging individuals, pediatric patients may also present with lens opacities. Whether acquired or congenital, the management of a cataract in a child is nuanced and requires understanding the role the crystalline lens plays in emmetropia, as well as accommodation.
What are pediatric cataracts?
A cataract is an opacification of the crystalline lens of the eye. This opacification may be total or partial, and the location, density, and size of the opacity drive the need for surgical intervention.1 Cataracts may be congenital in origin, which means they are present at birth (though they may or may not have been identified). They can be bilateral or unilateral.
Acquired cataracts refer to any form of cataract that occurs after birth. This may be due to environmental factors, e.g., trauma or radiation exposure, or later presentation of systemic or ocular conditions (e.g., uveitis or cerebrotendinous xanthomatosis).2
Classifying pediatric cataracts
Similar to age-related cataracts, the classification of pediatric cataracts is based on location, morphology, and etiology. These classifications can provide ophthalmologists with additional information in regard to prognosis and treatment options.
Pediatric cataract laterality
The laterality of a pediatric cataract is important in determining the visual prognosis. A bilateral presentation may be inherited, associated with systemic disease or exposure, or ocular comorbidity.
Unilateral cataracts, when present from birth, are almost always idiopathic.2 Unilateral cataracts associated with microphthalmia should raise suspicion for persistent fetal vasculature (PFV).3
In general, unilateral cataracts that occur at birth or in young childhood have an increased risk of amblyopia due to the obstruction of vision in only one eye.3 Larger, denser, centrally and posteriorly-located densities are more likely to cause amblyopia and thus worsen visual prognosis.3
Figure 1 shows an infant with a unilateral cataract of the left eye.


Figure 1: Image courtesy of Courtney Kraus, MD
Pediatric cataract morphology
The morphology of the cataract also provides information on the nature of the cataract and potential treatment options. Cataracts found in the pediatric population include cortical, lamellar, nuclear, anterior polar, posterior lenticonus, and total cataracts, among others.1,3 PFV cataracts have a spectrum of symptoms, including microphthalmia, stretched ciliary processes, persistent pupillary membrane, the persistence of the tunica vasculosa lentis, and a persistent hyaloid artery.1
Certain forms of cataracts may be classically found in certain conditions, such as:
- Anterior polar cataracts in Down syndrome
- Anterior lenticonus in Alport syndrome
- Posterior lentiglobus in Lowe syndrome1,3,4
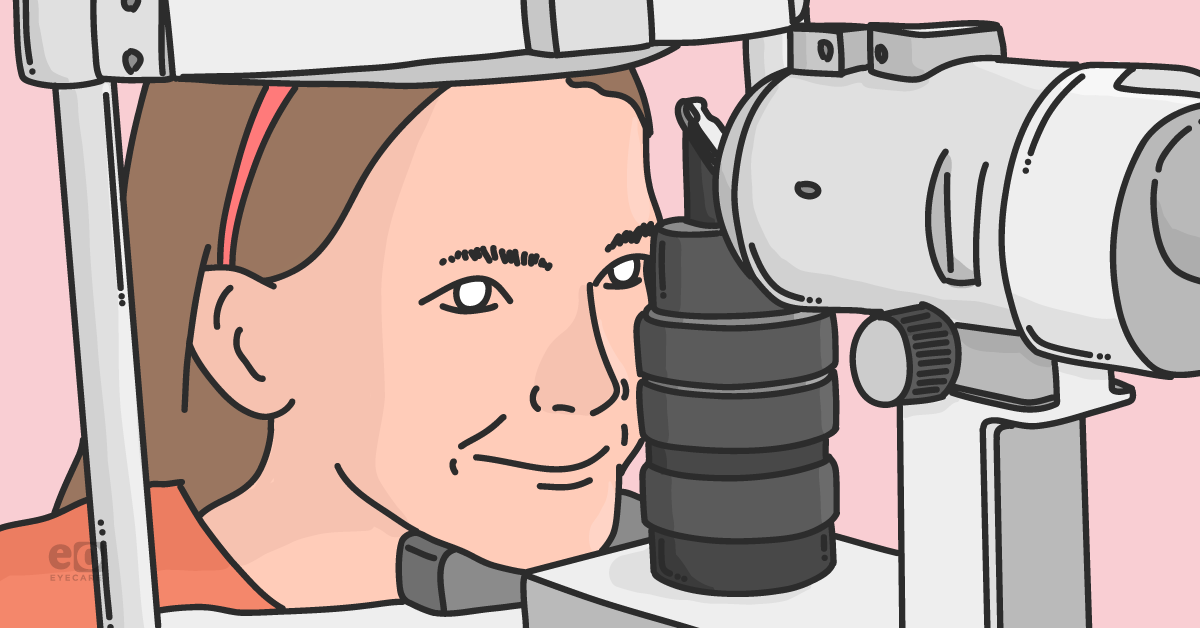
Traumatic cataracts present with a history of eye trauma, either blunt or penetrating, and may have challenges to surgical removal, including corneal scars, irregular astigmatism, and zonular compromise.3 Uveitic cataracts can be diffuse, associated with steroid use, and/or posterior subcapsular opacities.5
Figure 2 highlights a traumatic cataract in a pediatric patient.

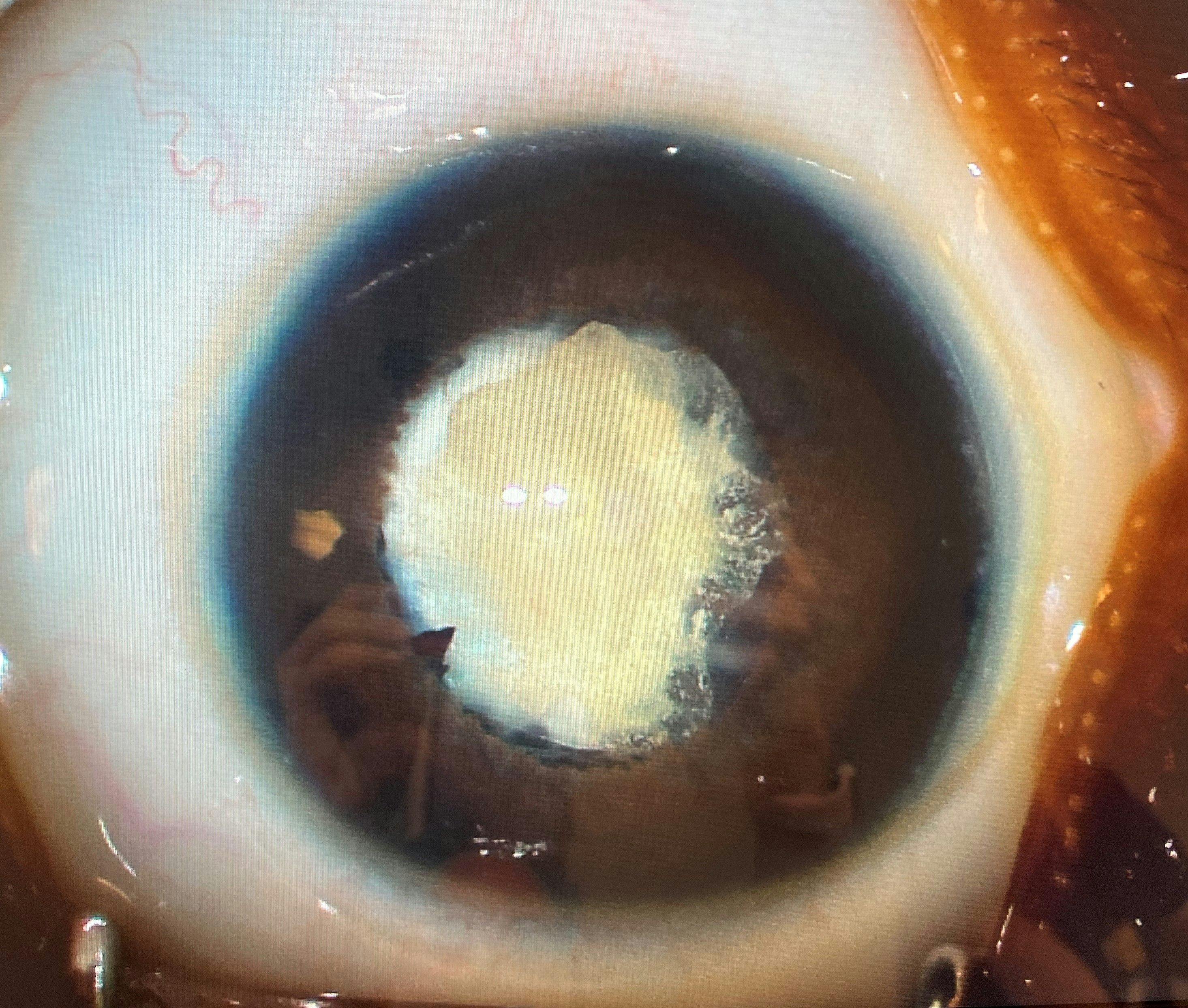
Figure 2: Image courtesy of Courtney Kraus, MD
The etiology and causes of pediatric cataracts
There are three main etiologies for cataracts: hereditary cataracts, cataracts associated with systemic or ocular diseases, and idiopathic cataracts.
Hereditary cataracts
Hereditary congenital cataracts are most often inherited in an autosomal dominant pattern.1,3 Bilateral nuclear opacities are the most common form of cataract with an autosomal dominant inheritance.1
Figure 3 features a fetal nuclear cataract in an otherwise healthy infant with a family history of cataracts.

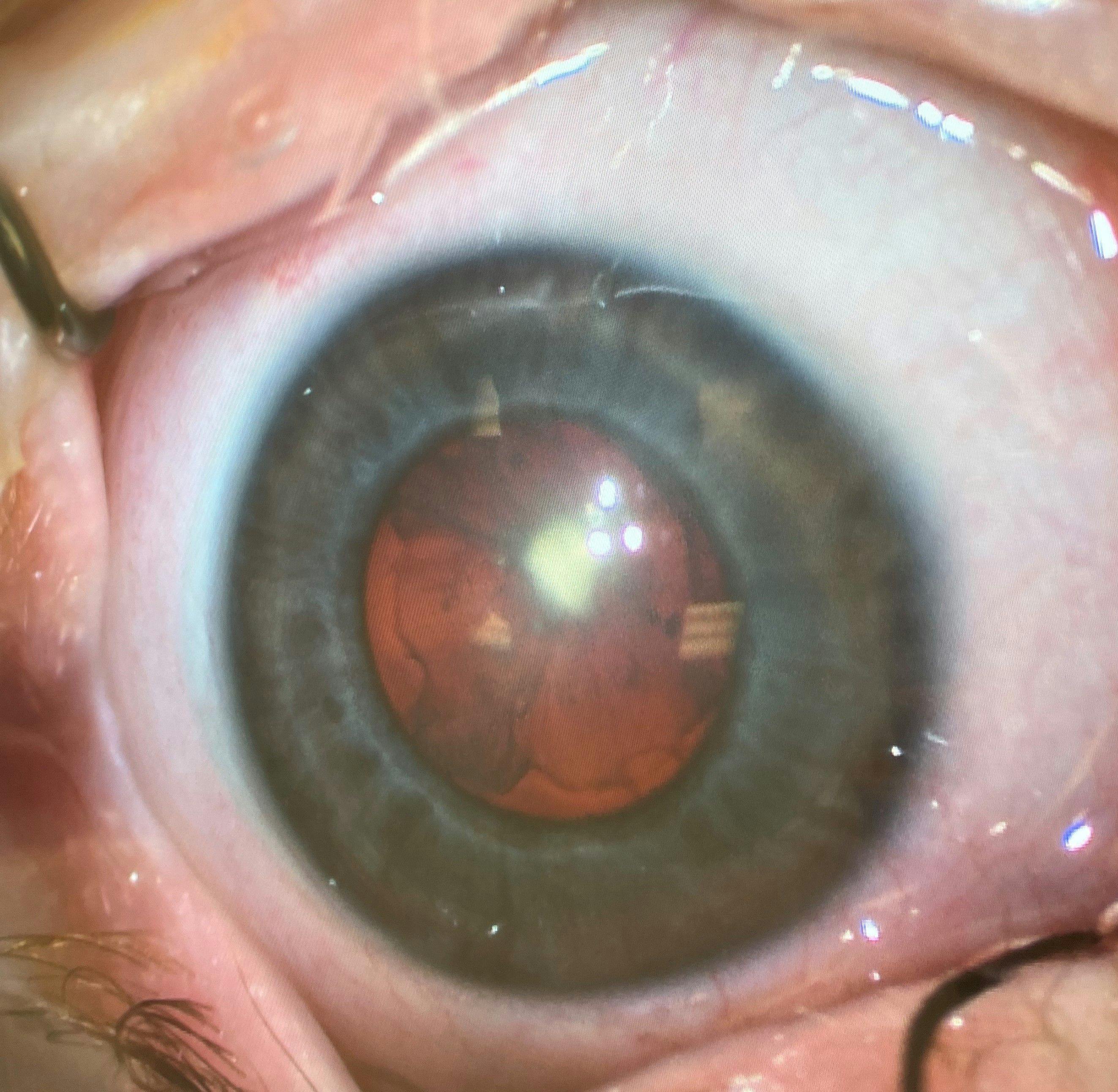
Figure 3: Image courtesy of Courtney Kraus, MD
Cataracts caused by systemic or ocular diseases
Non-familial bilateral cataracts are often associated with systemic diseases. Cataracts may be the first sign of a systemic disorder, so a thorough work-up should be performed, and referral to a genetic counselor should be considered.
Prenatal factors that may lead to congenital cataracts include TORCH infections (toxoplasmosis, syphilis, rubella, cytomegalovirus, or herpes simplex) or fetal alcohol exposure.3
Metabolic conditions in childhood that may lead to cataract development include galactosemia, neonatal hypoglycemia, hypoparathyroidism, and diabetes mellitus.3 It's important to note that trisomies 13, 14, and 21, as well as Turner syndrome, can present with cataracts.3 Additionally, juvenile idiopathic arthritis (JIA) and other forms of uveitis (HLA-B27) may lead to cataracts. Lastly, Marfan syndrome, as well as certain craniofacial disorders, are also associated with cataracts.3
Figure 4 demonstrates lens subluxation in Marfan syndrome.

Figure 4: Image courtesy of Courtney Kraus, MD
Idiopathic cataracts
Infantile or early-onset, idiopathic cataracts are most often unilateral.6 Acquired cataracts can be due to ocular trauma, inflammation such as uveitis, or exposures such as chronic steroid use or radiation.
Figure 5 shows a posterior subcapsular cataract associated with extensive oral steroid use.


Figure 5: Image courtesy of Courtney Kraus, MD
Presentation of pediatric cataracts
With few exceptions (e.g., blood sugar control in diabetics and maternal vaccination in prenatal infections), there are no preventative measures to avoid the development of pediatric cataracts. Therefore, screening examinations and early diagnosis are crucial in maximizing the visual prognosis. Because congenital cataracts are often associated with systemic disease, a detailed medical history and exam are important during the screening process.
Taking a patient history
Any of the following should prompt referral and further work-up:
- Patient Signs: Leukocoria, nystagmus, strabismus, asymmetric eye size, photophobia, and decreased vision or visual response in preverbal child.3
- Medical History: Birth weight, prematurity, trauma, development delay, evidence of maternal infections (TORCH exposures), radiation history, drug, or alcohol exposure.3,6
- Family History: A family history of congenital cataracts or other ocular or systemic conditions associated with cataracts.3
Exam findings
Pertinent exam findings for pediatric cataracts include decreased visual acuity, leukocoria, an absent or abnormal red reflex, strabismus, and nystagmus. It’s important to note that even subtle abnormalities can be appreciated as an irregularity in the retinoscopy streak. A non-mydriatic assessment may help in evaluating the extent that opacity is visually significant. Additionally, strabismus is likely seen in unilateral or asymmetric cataracts and is often seen in long-standing or amblyogenic cataracts.
Figure 6 highlights a cataract associated with iris coloboma.

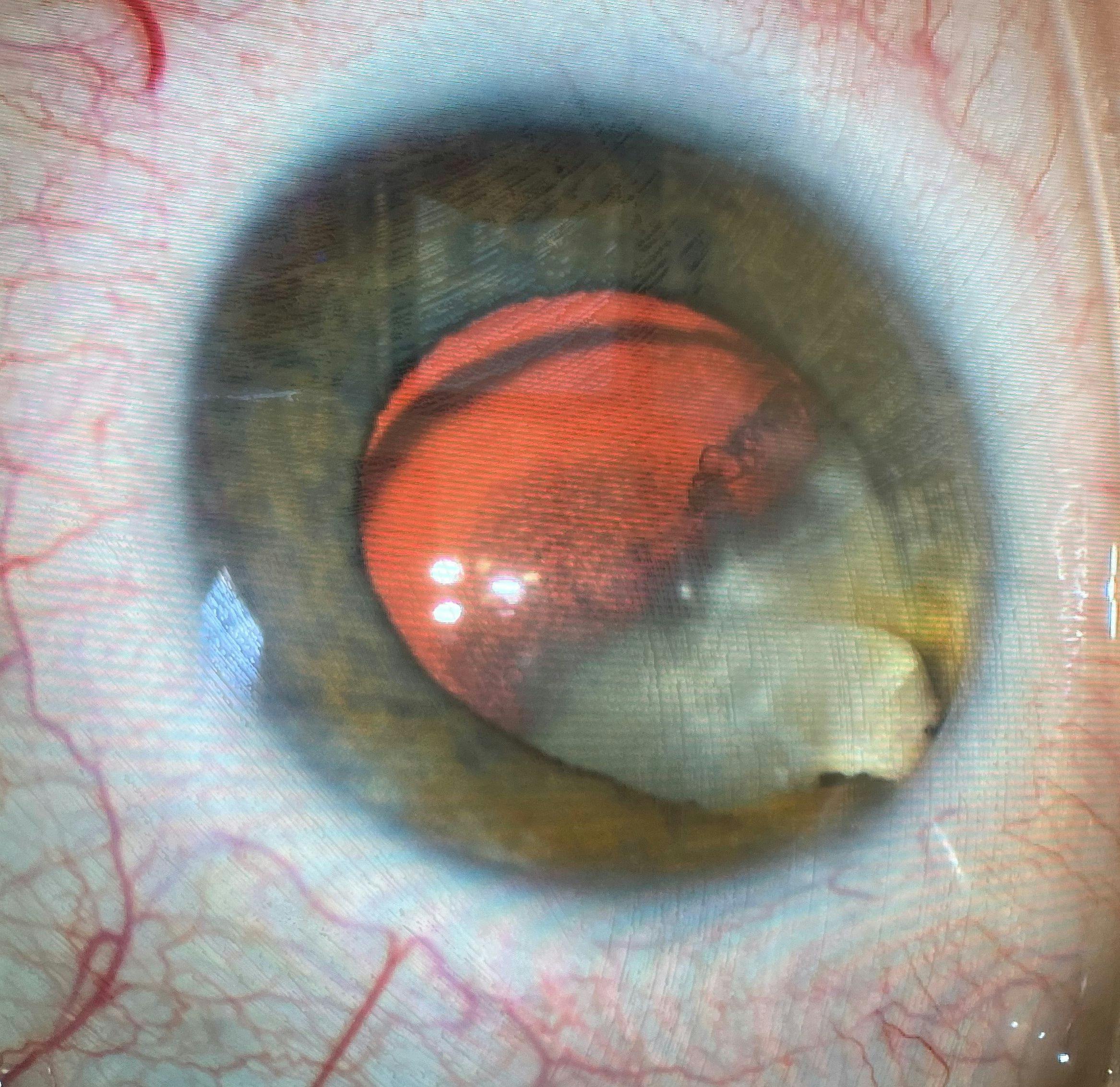
Figure 6: Image courtesy of Courtney Kraus, MD
Additional testing for congenital cataracts
Unilateral cataracts are often idiopathic; thus, additional laboratory testing is usually unnecessary.3,6
“However, cases with a positive family history of congenital cataracts may need further testing.”
For patients with bilateral cataracts without a definitive etiology, additional laboratory testing is needed to rule out associated conditions. A serology work-up can rule out TORCH infections, diabetes, and metabolic disorders, such as hypoparathyroidism. Hypotonia, failure to thrive, and severe developmental delay are concerns for galactosemia or Lowe syndrome, which can be further confirmed with a urine test.3 A genetic counselor may be involved to further guide genetic evaluations.
Indications for imaging and other diagnostic procedures
If the in-office examination is challenging or the lens opacity prevents view to the posterior segment, ocular ultrasonography and examination under anesthesia are recommended to better view the ocular structures posterior to the density and the cataract itself.3 For visually significant cataracts, these additional procedures are typically performed immediately prior to cataract removal.
Treatments for pediatric cataracts
Removing a cataract is not as straightforward as verifying the presence and location of a cataract, as the act of removal comes with a loss of accommodation. The risks and benefits of preserving natural accommodation should be weighed against the current vision and visual prognosis. If the cataract does not obstruct vision and has low amblyogenic potential, observation is an option, but the patient should be closely followed.3
When is surgery indicated for pediatric cataracts?
If the cataract presents with vision obstruction or high amblyogenic potential, then cataract removal is necessary.
Indications for cataract surgery include:
- Decreased vision (20/50 or worse)
- Distortion of the retinoscope reflex
- Inability to obtain accurate refraction
- Obstructed view of the posterior pole
For a patient with amblyopia, the optimization of patching or atropine penalization should occur prior to surgical intervention or be established as impossible. Amblyopic patients on appropriate therapies should undergo cataract removal when they stabilize, have decreased visual acuity, or when the lens opacity progresses. Other indications for surgeries include intolerance to glare, a persistent eye preference, or asymmetric saccades of one eye with visual fixation.
Considering cataract morphology
Cataract morphology can provide information on the decision to operate, as some opacities are less visually significant and less amblyogenic than others. Anterior polar and cortical cataracts are often managed conservatively without surgery, whereas total, nuclear, and PFV cataracts are more likely to be removed.1,3 Cortical cataracts often have a very good visual prognosis due to their frequent bilateral nature, and appearance later in life.1,3
The ideal time for cataract surgery in children
For older children, especially those beyond amblyogenic age, the best time for surgery is driven by convenience and patient preference. For cataracts diagnosed at birth, however, there are significant considerations for the timing of the surgery to balance optimal prevention of amblyopia with the least risk of anesthesia-related complications in an infant.
For unilateral congenital cataracts, the preferred age of treatment is 4 to 6 weeks old.7 Bilateral cataracts diagnosed at birth can be operated on before 8 weeks of age.7 The recommended timeline for the surgeries is to separate the two eyes by no more than a week.7
“It is important to keep the time between the two surgeries minimal to avoid amblyopia in the eyes with asymmetric vision.”
Immediate bilateral sequential surgery (i.e., operating on both eyes in one session) is usually reserved for cases where anesthesia presents a greater risk to the patient.7
Intraocular lens implantation considerations
Intraocular lens (IOL) implantation in a child is unique despite following much of the same surgical steps as in adults. Calculating an IOL strength in a child requires the same formulas and variables (axial length and keratometry) as in adults. However, a special consideration for children is the continued growth of a child’s eye, with exponentially greater growth in the first year of life.8 The axial elongation that occurs with age is usually countered by changes in the refractive power of the crystalline lens.
Accommodating myopic shifts in children
When this lens is removed during cataract surgery, the child loses the natural counterbalance to the myopic shift of eye growth. An implanted IOL cannot change power like a natural lens; therefore, surgeons must select a postoperative refractive status of intentional hyperopia to attempt to minimize adult refractive error.9-11
More hyperopia is left for younger patients due to the greater potential for growth. For this reason, many surgeons choose to leave the eye aphakic when operating on children less than 1 year of age.
For patients with bilateral cataracts, opting for aphakia allows correction with contact lenses or aphakic glasses. These are relatively easily tolerated. Many surgeons will consider secondary IOL implantation after age 5, as much of the eye growth has occurred, and the expected residual uncorrected refractive error in adulthood is expected to be minimalized.7
Managing cataracts with contact lenses
For unilateral cataracts in patients younger than 7 months, surgeons tend to favor aphakia with contact lens management.10 Contact lenses are preferred over glasses as there is tremendous aniseikonia with significant unilateral high hyperopic correction. However, data from the Infant Aphakia Treatment Study (IATS) found that if there are concerns for poor follow-up or the cost of contact lens handling is too burdensome for parents; then an IOL may be placed primarily at the time of the surgery.10
Potential complications of cataract removal
Operative and postoperative risks include posterior capsule opacification, reproliferation of lens material into the visual axis, IOL displacement, pupil size and shape abnormalities, and variability in postoperative refractive error.3
“Posterior capsule opacification is a common complication, especially for younger patients and those with IOL placements.”
For this reason, surgical techniques in young children undergoing IOL implantation often include a primary posterior capsulorrhexis with or without anterior vitrectomy.3 Surgery to remove proliferated epithelial cells is necessary when opacity prevents retinoscopy or fundus visualization.
Rare risks, such as endophthalmitis, retinal detachment, and complicated associated conditions may appear years after surgery and should be discussed prior to the procedure.3,12 Glaucoma is a common condition that may present years following cataract surgery.3,10
Parental education on pediatric cataracts
Parents who understand the goals, risks, advantages, and potential complications of cataract surgery are more likely to comply with the treatment plan. Thus, it is crucial for ophthalmologists to have a thorough discussion on the risks and benefits of the surgeries as well as the postoperative treatment plan. With early screening, early management, and strong parental compliance, a patient with congenital cataracts can have a good visual outcome.
