Cornea collagen cross-linking (CXL) is a procedure used to stabilize the cornea in conditions such as keratoconus, pellucid marginal degeneration (PMD), or in patients with corneal ectasia.
The procedure is minimally invasive and is useful in stabilizing and preventing the progression of corneal ectasia for patients with keratoconus, PMD, or post-refractive ectasia.
Overview of corneal cross-linking
Keratoconus is a disorder (incidence about 1 per 2,000) where the central or paracentral cornea progressively thins and eventually can protrude, leading to a cone-shaped cornea.
1 With eventual thinning, the cornea can develop small stress lines called Vogt Striae, which can be seen at the apex of the cone.
In later stages, a tear in the Descemet membrane can occur, resulting in sudden onset pain, corneal edema, or an acute hydrops episode. This leads to corneal scarring, which limits vision.1
Figure 1 is corneal tomography showing inferior corneal steepening and posterior corneal elevation in a keratoconus patient.2
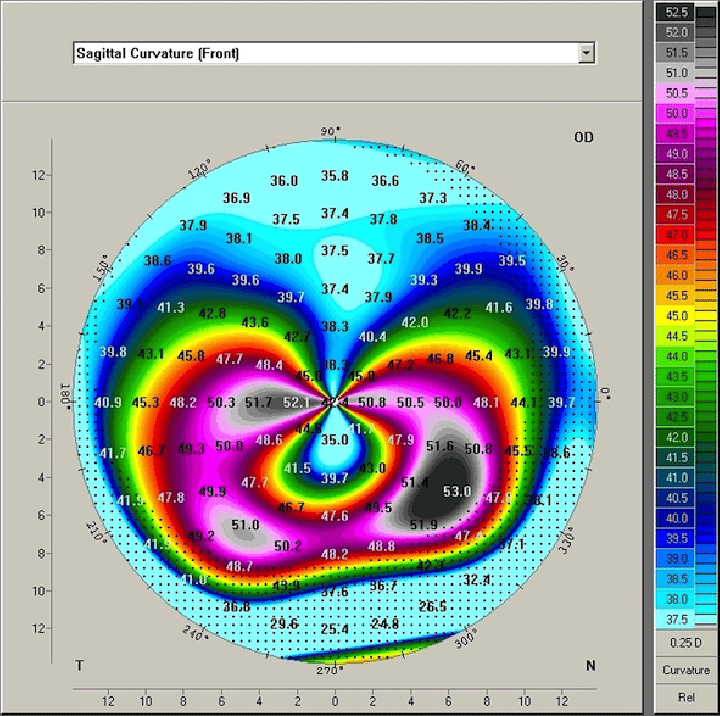
Pellucid marginal degeneration is another corneal ectatic disorder where thinning occurs most frequently at the inferior cornea. PMD has an ectatic zone that lies above the point of maximum
corneal thinning and often is described as a “crab claw” on corneal topography maps.
Figure 2 is an anterior sagittal map depicting the “crab claw” seen in PMD.3
Refractive surgery, such as
laser assisted in situ keratomileusis (LASIK), photorefractive keratectomy (PRK), or small incision lencticule extraction (SMILE), can lead to corneal ectasia in patients with pre-existing corneal ectatic conditions (forme fruste keratoconus, PMD, or keratoconus). Additionally, it can occur in patients with low preoperative corneal thickness and patients left with low residual stromal bed.
For the above patients who have developed corneal ectasia, corneal cross-linking can halt progressive thinning and lead to stabilization of the cornea. If untreated, continued corneal thinning can lead to asymmetric astigmatism, persistent corneal edema, or corneal hydrops with eventual scarring. Corneal scarring and persistent edema may then require more aggressive interventions such as corneal transplant to improve vision.
Goals of corneal cross-linking
The primary goal of
corneal cross-linking is to stabilize the cornea and prevent further ectasia. The first step is to allow sufficient riboflavin drops to diffuse into the cornea. The second component requires exposure of the riboflavin-soaked cornea to UVA light.
Once exposed, the riboflavin generates a reactive oxygen species, which induces the formation of covalent bonds between collagen molecules, stabilizing the cornea. Riboflavin has an absorption peak of 370nm, which in combination with UVA light, works to stabilize the cornea and, when done in a standardized fashion, should not damage nearby ocular structures.4
Corneal cross-linking procedures and protocols
Different procedures have been used to perform corneal cross-linking, including the original Dresden protocol, transepithelial CXL, and accelerated CXL. Initially, riboflavin was unable to diffuse into the cornea; thus, the standard Dresden protocol required the corneal epithelium to be removed.
4 Newer formulations of riboflavin have been able to penetrate intact corneal epithelium and may not require the removal of the corneal epithelium leading to less pain and a faster visual recovery. These procedures are still being studied.
Standard Dresden protocol for corneal cross-linking
The standard Dresden protocol is used in patients with a minimal cornea thickness of 400μm.5
Steps in the CXL standard Dresden protocol include:
- Topical anesthetic is instilled in the eye, and the central 7 to 9μm of corneal epithelium is then debrided.
- Next, 0.1% Riboflavin 5-phosphate and 20% dextran solution are instilled every 5 minutes for 30 minutes.
- UVA light (370nm) is then exposed for 30 minutes while riboflavin is continued to be instilled in the eye every 5 minutes.
- After 1 hour, the procedure is finished, topical antibiotics are applied, and a soft bandage contact lens with good oxygen permeability is placed.5
Different variations include the epithelium-on or trans-epithelial methods, however, studies thus far have shown variable effectiveness with these methods. Epithelium-off CXL is still the preferred (and currently only FDA-approved) method for stabilizing the cornea.4
Side effects of corneal cross-linking
Commonly seen after-effects of CXL include corneal flattening, reduction in corneal cylinder, and corneal thinning. The corneal thinning is proposed to be due to the compaction of corneal tissue after CXL. Other common side effects of corneal cross-linking include pain during the first few days after the procedure and stromal haze.
The corneal epithelium will typically heal in 3 to 4 days, and it is important to discuss this discomfort with the patient prior to performing the procedure. Riboflavin penetrates the anterior cornea more than the posterior cornea; therefore, the effects are seen more in the anterior cornea.
No endothelial damage is caused when CXL is correctly performed. More severe risks/complications can include infectious keratitis, persistent corneal edema, and endothelial damage if the minimum corneal thickness is too thin.6
CXL contraindications
Contraindications to corneal cross-linking include a corneal thickness of less than 400μm. This is because when the corneal is less than 400μm, riboflavin can penetrate and damage the corneal endothelium. For patients with corneal thickness between 320 to 400μm, hypotonic riboflavin can be used to swell the cornea to reach the 400μm threshold to perform safe corneal cross-linking.
Other contraindications include severe corneal scarring or opacification, concurrent infection, prior herpetic infection, history of poor epithelial wound healing, severe ocular surface disease (dry eye), or uncontrolled autoimmune disorders.6
Alternative therapies for CXL
If CXL were performed on a patient who was not an ideal candidate (i.e., history of herpetic keratitis), reactivation could occur, leading to worsening inflammation and potential
corneal scarring. Patients with poor epithelial wound healing could develop a non-healing epithelial defect which may require intensive therapy such as an amniotic membrane graft if lubrication and bandage contact lens treatments fail.
6 Proper patient selection is critical prior to the procedure.
Another potential concern would be if the patient had persistent corneal haze after cross-linking. This would limit their visual potential, and a discussion of a corneal transplant to improve visual potential would be indicated. If a patient’s corneal thinning were too advanced at the time of presentation, this would also be a patient with the potential to fail CXL.
For these patients, even if corneal cross-linking were to be performed, their corneal thinning may continue to progress to the point of persistent corneal edema. A corneal transplant (such as a penetrating keratoplasty) would be recommended in this scenario. Additionally, for many patients, CXL does not provide an increase in functional vision. Often, patients present for CXL later in the disease course where the corneal ectasia is advanced.
Although corneal cross-linking can stabilize the cornea, the procedure does not correct their vision since they have developed high and irregular astigmatism. For these patients, spectacle or contact lens correction is usually needed to provide functional vision.
Combining intracorneal ring segments with CXL
Ophthalmologists have attempted to combine CXL with other refractive techniques for select patients. One of these techniques includes placing intracorneal ring segments (ICRS) with sequential or subsequent CXL. Intracorneal ring segments have been approved for mild to moderate keratoconus. A clear cornea and a corneal thickness >450μm are required for the procedure.
Patients may require spectacles or contact lenses after the procedure for best vision. The intrastromal ring segment can help flatten the cornea, making it easier to use contact lenses. If the patient is unhappy after the procedure, the ICRS can be removed. Of note, ICRS are not a contraindication to corneal cross-linking.7
Combining photorefractive keratectomy with CXL
Other techniques include photorefractive keratectomy either before or after CXL to improve visual acuity and stabilize keratoconus. PRK is an outpatient refractive surgery performed with an excimer laser (193nm) to apply light energy to reshape the cornea. For patients with mild to moderate
astigmatic changes which have been stable over time, PRK could be used to make the astigmatism more symmetric, allowing for use of a contact lens.
4There have been multiple studies evaluating PRK and CXL; both sequentially and in a same-day fashion. Choosing the correct candidates for the procedure and setting expectations are key.
Combining CXL with a toric intraocular lens
Corneal cross-linking, followed by implantation of a toric
intraocular lens (IOL), has been performed in patients with mild to moderate keratoconus with cataract. This would require the patient to undergo cataract extraction with the insertion of a toric lens after the eye has stabilized post-CXL.
A toric IOL is used to decrease astigmatism induced by the cornea; therefore, the CXL would be performed to stabilize the cornea first. Patient selection is critical for these patients, as toric lens placement is not recommended in patients with astigmatism that cannot be corrected by an IOL (e.g., if the corneal cylinder is too high or irregular, if IOL power falls out of range).4
Additionally, a triple therapy including topography guided PRK to regularize the corneal shape, CXL procedure, and subsequent placement of a toric IOL can be used to optimize refraction for a patient.4 For this triple therapy, patient selection is critical.
Corneal cross-linking aftercare
After corneal cross-linking therapy, depending on residual astigmatism and corneal ectasia, spectacles or soft toric contact lenses can be used in mild cases. Soft toric lenses can be used in cases of mild astigmatism <1 diopter (D).
As the astigmatism increases between 1 to 3D, a custom soft toric contact lens or a spherical rigid gas-permeable (RGP) toric lens may be recommended. For more than 3D of astigmatism, a toric RGP is recommended.8 Additionally, a scleral contact lens can provide excellent visual correction in these patients with very high astigmatism.
Aftercare for patients with advanced irregular corneal astigmatism
For patients with more advanced irregular corneal astigmatism, hard or gas-permeable contact lenses are associated with a dramatic improvement in vision. Gas-permeable lenses have smaller diameters than soft lenses and allow for the circulation of tears with each blink.8
An RGP maintains its shape, and a tear lake fills the space between the lens and the cornea, referred to as the sagittal vault. Other special lenses designed for keratoconus include custom-designed, scleral, and hybrid lenses.4
A scleral lens is recommended in cases of moderate to advanced keratoconus and is boasted to have improved comfort with good oxygen permeability.9 Scleral lenses are indicated for patients who are intolerant to RGP and, in some cases, can be used to prevent the need for corneal transplant in advanced keratoconus.10
Aftercare for patients with keratoconus or PMD
For patients with keratoconus or PMD, progressive monitoring with corneal topography is critical in identifying those who would benefit from early corneal cross-linking.
A minimum stromal thickness of 400μm is important to prevent riboflavin damage to the corneal endothelium. If the stromal thickness is between 320 to 400μm, a hyperosmotic version of riboflavin can be used to reach the minimum corneal thickness of 400μm.
Final thoughts
Early diagnosis of worsening corneal ectasia and prompt intervention with corneal cross-linking is key to allowing patients to retain adequate vision with spectacle or contact lenses throughout their lifetime. Corneal cross-linking is a well-tolerated procedure for patients with corneal ectasia after refractive surgery or those with advanced corneal ectasia from keratoconus or PMD.
CXL can stabilize the cornea and prevent long-term vision dysfunction associated with corneal edema or scarring.
For patients who fail CXL due to advanced corneal thinning leading to chronic corneal edema, a corneal transplant (such as a penetrating keratoplasty) may be indicated. Also, for patients with advanced astigmatism or corneal ectasia, CXL can be performed to stabilize the cornea, and functional vision can then be provided through the use of soft contact toric lenses, toric RGP, scleral lenses, or hybrid lenses in most cases.