


Modern laser-assisted in situ keratomileuses (LASIK) refractive surgery is one of the safest and most successful procedures in medicine. LASIK boasts high patient satisfaction rates ranging from 95% to 98%, with 20/20 or better-uncorrected vision in 90.8% to 92% of eyes.1,2 Moreover, 20/40 uncorrected vision—which is the legal driving limit even in the most restrictive of states—is achieved in 99.5% of patients.1,3
False historical barriers: astigmatism and pupils
Many LASIK patients who eventually present to our practice arrive having been told by their prior optometrist or ophthalmologist they are not LASIK candidates. The most common reason we encounter is the myth that LASIK cannot correct astigmatism. Not only can LASIK correct astigmatism, but modern LASIK uses pupil tracking and iris registration for cyclotorsion compensation for excellent alignment when correcting astigmatism.4
Another myth about LASIK is that those with large pupils may have permanent issues with nighttime glare or dysphotopsias. This was a well-intentioned point of caution decades ago, considering that dilating patients pharmacologically does increase glare.5 Upon evaluating large amounts of patient data, there is no connection between pupil size and glare after 6 months of healing by either multivariate regression analysis or analysis of variance (ANOVA).6
When looking beyond simply pupil size at nighttime quality of vision, the FDA’s PROWL studies indicate that patients are more likely to have better nighttime quality of vision than with their prior glasses or contacts.7 These encouraging data are news to patients and other ophthalmologists who do not practice in the refractive space.
“Do you feel more dryness with your contacts or your glasses?”
To respect the ocular surface is to respect vision, and patients with signs or symptoms of dryness need to be evaluated wisely. Studies evaluating LASIK and photorefractive keratectomy (PRK) do not always agree on which may respect the surface best. Some studies show fewer post-operative dryness issues with LASIK and some with PRK.8,9,10 Small-incision lenticule extraction (SMILE), which cuts fewer clock hours of the corneal surface, has shown improvements in post-operative dryness measures in some studies but not all.11,12
Modern LASIK, however, can be very helpful for contact lens-induced components of dry eye. Those with dryness in their contact lenses who have LASIK are more comfortable after their laser vision correction.10 In a cohort study, contact lens-wearing patients who had LASIK had less dryness than those who continued wearing contact lenses.13 In my experience, those patients with symptomatic dryness due to contact lens use tend to be the happiest and most comfortable of our LASIK patients.
Sometimes better is better—both for cataracts and LASIK
Many of our cataract patients have more than one issue, with ocular surface abnormalities being perhaps the most common.14 They may have cataracts and glaucoma. Perhaps cataracts and macular degeneration. Even cataracts and amblyopia. With appropriate expectations, specifically that our goal is “as much better as possible” and not absolute perfection, these patients can be very happy.
Similarly, the extended-depth-of-focus (EDOF) category of intraocular lenses has been growing, even though they do not provide a completely full range of vision. These EDOF lenses provide a happy medium when surgeons want to deliver more range than a monofocal IOL but may not be comfortable with how a patient’s eye can handle the light splitting of a trifocal IOL for daytime or nighttime vision quality. Our EDOF IOL patients tend to be very happy as long as they understand their goal is more range and not all.
Absolute numbers give helpful context
Screening for preexisting keratoconus remains one of the most crucial aspects of a refractive evaluation. Keratoconus is a disease of thinning and weakened tissue, so further removing tissue in these cases should be avoided. The corneal shape is evaluated as a surrogate for proper anterior segment structure-function. Patients with irregular corneal shapes suspicious for keratoconus should instead have a non-ablative method of vision correction,15 such as the EVO ICL, our most common recommendation for myopic patients with accommodation who cannot have laser vision correction.
But what about those whose corneas fit neither the textbook's perfect nor the diseased pages? It turns out that high corneal steepness in the absence of abnormal topography is not predictive of post-LASIK ectasia risk on univariate analysis, and neither is an asymmetric bow tie.16 Forme fruste keratoconus (FFKC) is topographically defined as inferior steepening of 1.4D or greater.17
Some surgeons would consider PRK but not LASIK in such a case if the ablation depth is small, others would pair PRK with prophylactic corneal crosslinking, and still, others would only recommend EVO ICL or a lens-based procedure. After all, the risk of post-LASIK ectasia in an eye with FFKC is 20 times the normal risk.16
Table 1 illustrates Post-LASIK ectasia risk from a large, retrospective study. PRK ectasia risk would be expected to be even lower.
| Preoperative Finding | Ectasia Risk as Ratio | Ectasia Risk as Percent |
|---|---|---|
| FFKC | 1:161 | 0.6% |
| Inferior steepening (IS) or skewed radial axis (SRA) | 1:484 | 0.2% |
| Age ≤ 30 | 1:830 | 0.1% |
| (IS or SRA) and Age ≤ 30 | 1:367 | 0.3% |
Data from Schallhorn S. "Can we eliminate the risk of ectasia? " as presented at: American Society of Cataract and Refractive Surgery annual meeting; April 13-17, 2018; Washington.
A twenty-fold increased risk is indeed high, and we avoid LASIK in these FFKC patients. The actual number we are avoiding in such cases surprises many who might have overestimated it. FFKC eyes actually have a post-LASIK ectasia risk of only one in 160, or 0.6%. We know from a different review study that PRK has a lower incidence of ectasia than even LASIK in the general population (0.02% versus 0.09%).18 As a result, we can give the vast majority of patients very low-risk procedure recommendations. A zero risk with LASIK is unattainable, just as the risk of a contact lens infection will never be zero even with perfect compliance.
Belt and suspenders approach
The idea of someone with both a belt and suspenders is that a backup support system exists. We are fortunate to have that backup, which is thankfully seldom needed. Corneal cross-linking (CXL) is mostly used for naturally occurring keratoconus, but it is also effective in post-refractive ectasia. Success rates in stiffening the cornea, generally defined as halting progressive steepening, range from 75 to 93%.19, 20
Look at the full picture
In the corneal OCT in Figure 1, a ceramic sliver (white) is visible in his posterior cornea but not extending through Descemet’s membrane. Many may consider an intracorneal foreign body a contraindication to corneal refractive surgery. While corneal applanation for LASIK flap creation would have been unwise, careful counseling and PRK resulted in a great result and a happy patient.

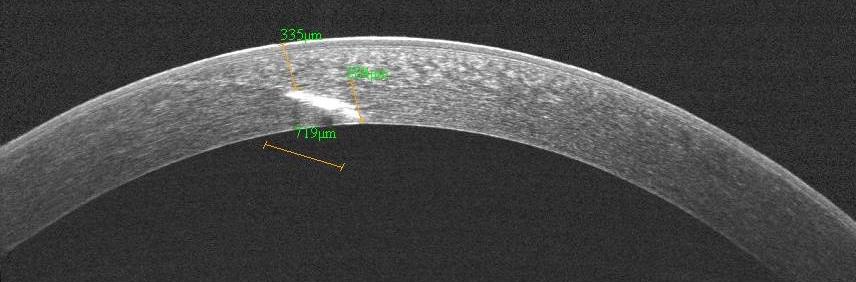
Figure 1
When evaluating patients for laser vision correction, we must consider the whole patient. There are some patients whose eye health or psychological and emotional stability would be better served by glasses, contacts, or a non-refractive method of vision correction. Others check all the traditional boxes. How we handle and counsel those caught in the middle gives us a chance to make a significant difference in our patients’ quality of life.
