




Corneal collagen crosslinking (CXL) is the primary intervention for managing corneal ectasia; however, the established protocol is now dated, going back to the 1990s.
CXL consists of several steps that involve epithelial debridement, riboflavin administration to the stroma, and ultraviolet A (UVA) irradiation.1 The procedure works by inducing chemical changes to the collagen network. Specifically, when riboflavin is excited by UVA, a photochemical reaction generates covalent bonds to form between collagen molecules within the stroma, thereby stiffening the cornea and strengthening its architecture.2
Indications
CXL is indicated for the management of progressive corneal ectasias, including keratoconus, pellucid marginal degeneration, post-refractive ectasia, and Terrien’s marginal degeneration.3,4 Additional indications include infectious keratitis and bullous keratopathy.5 Until recently, even if sight-threatening and progressive disease existed, corneal thickness less than 400μm would have been considered a relative contraindication for therapy due to the risk of endothelial toxicity.
Contraindications
CXL contraindications include:6
- Corneal thickness (after epithelial removal) less than 400 μm (endothelial toxicity)
- Prior herpetic infection (risk of herpes reactivation)
- Any concurrent infection
- Severe corneal opacification or scarring
- History of poor epithelial wound healing
- Autoimmune disease
- Severe dry eye or ocular surface disease
- Neurotrophic keratopathy
- Pregnancy
Procedure
Conventional CXL follows the Dresden protocol:1
- Epithelium Removal
- After administration of topical anesthetic drops, the central 7-9 mm of corneal epithelium is debrided with a blunt instrument (e.g., 69 blade) to expose the corneal stroma.
- Riboflavin Administration
- Riboflavin 0.1%, diluted in 20% Dextran, is applied five minutes before UVA irradiation and reapplied every five minutes once irradiation has begun.
- Ultraviolet-A Irradiation
- The riboflavin-saturated cornea is exposed to UVA (370 nm, 3 mW/cm2) for 30 minutes.
- Wound Dressing
- A breathable bandage contact lens is placed until corneal re-epithelialization has been completed.
Variations in cross-linking technique exist and primarily rely on either increasing UVA irradiation intensity to reduce procedure time (accelerated CXL; A-CXL) or attempting to preclude the need to debride the epithelium. Long-term studies are needed to compare outcomes accurately.
Protocol modifications
Hypo-osmolar riboflavin
In cases where corneal thickness is less than 400μm, administration of hypo-osmolar riboflavin is recommended.7 It functions by transiently swelling the cornea to increase its thickness to protect the endothelium better. Wollensak et al. reported that hypo-osmolar riboflavin resulted in successful CXL without endothelial damage.
Notwithstanding the latter, it should be noted that the hypo-osmolar effect of riboflavin can result in variable corneal thickness.7
Contact Lens-assisted CXL
First described by Jacob et al., contact lens-assisted CXL is a technique used to increase corneal thickness with a riboflavin-soaked contact lens.8 The efficacy and safety of this technique are similar to that of conventional CXL with no postoperative pathological changes to the corneal endothelium.9 A recent comparative study demonstrated that visual and anatomic outcomes in patients with progressive keratoconus were similar when comparing contact lens-assisted CXL, transepithelial CXL, and conventional CXL.10
Sub400 protocol
Epithelial removal is generally needed to permit adequate riboflavin saturation within the stroma. However, compromising the corneal endothelium is a potential risk of this procedure, especially in patients with a corneal thickness of less than 400 μm. Transepithelial approaches, which would mitigate the need for epithelial debridement, have been proposed but have not demonstrated similar efficacy as compared to standard technique.11
Subsequently, this protocol was proposed to safely and effectively perform CXL in patients with progressive corneal ectasia and a corneal stromal thickness of less than 400 μm.12 The technique differs from conventional CXL in that ultrasound pachymetry is performed every 5 minutes at the thinnest area of the cornea found on preoperative pachymetry while the exposed stroma is soaking in riboflavin.
Once soaking is complete, pachymetry is again performed to determine the minimum corneal thickness to calculate individualized fluence requirements such that a demarcation line after CXL would be expected to occur 70μm above the endothelium, per this group’s algorithm.13 The fluence requirements are met by titrating the UVA irradiation duration.
Hafezi et al. showed that at one year, 35 of 39 eyes evaluated had stable (less than one diopter of change) or improved Kmax in patients with advanced keratoconus.12
Figure 17 illustrates optical coherence tomography and densitrometry measurements pre-operatively (A), at 2 months (B), and at 6 monthe (C) after the Sub400 CXL procedure. In B, the depth of demarcation line (2 months post sub-400 epithelium off CXL) is indicated with an arrow.7

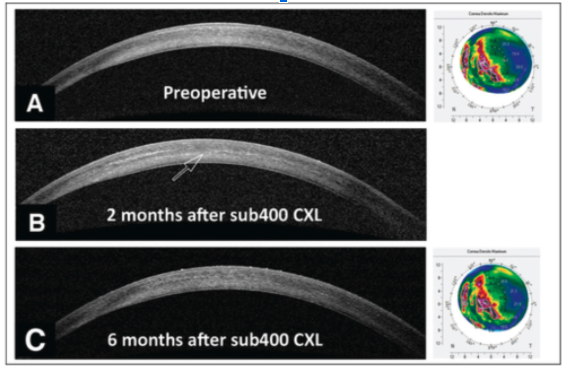
Figure 1
Recent Research
Inclusion criteria
Per the sub400 protocol, patients with progressive corneal ectasia and a corneal stromal thickness of less than 400μm may be considered and are not automatically excluded from CXL. The sub400 protocol authors acknowledge that their treated cohort's minimum preoperative corneal thickness was 325μm. Upon intraoperative removal of corneal epithelium, minimum corneal thickness measured 214μm. Accordingly, patients with corneas as thin as 325 μm may be considered.
Benefits and risks
CXL benefits include stable best-corrected visual acuity at one-year, no cases of endothelial decompensation, and treatment success (defined as tomographical stability) in 90% of their cohort following the sub400 protocol.12 The most significant concern in patients with thin corneas is endothelial compromise. However, as stated above, no evidence of corneal decompensation was noted.
Conclusions
In conclusion, the sub400 protocol for CXL offers an expanded indication for use in patients with progressive corneal ectasias and thin corneal thickness. This is particularly important as this patient population is at high risk for vision-threatening complications.
While initial results are promising, research to further evaluate protocol safety and efficacy is needed as well as providing a standardized treatment approach for this patient population.
References
- Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003 May;135(5):620-7. doi: 10.1016/s0002-9394(02)02220-1. PMID: 12719068.
- Spoerl E, Mrochen M, Sliney D, Trokel S, Seiler T. Safety of UVA-riboflavin cross-linking of the cornea. Cornea. 2007 May;26(4):385-9. doi: 10.1097/ICO.0b013e3180334f78. PMID: 17457183.
- Raiskup F, Spoerl E. Corneal crosslinking with riboflavin and ultraviolet A. Part II. Clinical indications and results. Ocul Surf. 2013 Apr;11(2):93-108. doi: 10.1016/j.jtos.2013.01.003. Epub 2013 Jan 28. PMID: 23583044.
- Hafezi F, Gatzioufas Z, Seiler TG, Seiler T. Corneal collagen cross-linking for Terrien marginal degeneration. J Refract Surg. 2014 Jul;30(7):498-500. doi: 10.3928/1081597X-20140527-02. Epub 2014 Jun 3. PMID: 24892378.
- Balparda K, Maldonado MJ. Corneal collagen cross-linking. A review of its clinical applications. Arch Soc Esp Oftalmol. 2017 Apr;92(4):166-174. English, Spanish. doi: 10.1016/j.oftal.2016.10.004. Epub 2016 Nov 30. PMID: 27914659.
- Galvis V, Tello A, Ortiz AI, Escaf LC. Patient selection for corneal collagen cross-linking: an updated review. Clin Ophthalmol. 2017;11:657-668. Published 2017 Apr 7. doi:10.2147/OPTH.S101386
- Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009 Apr;35(4):621-4. doi: 10.1016/j.jcrs.2008.10.060. PMID: 19304080.
- Jacob S, Kumar DA, Agarwal A, Basu S, Sinha P, Agarwal A. Contact lens assisted collagen cross-linking (CACXL): A new technique for cross-linking thin corneas. J Refract Surg. 2014;30:366–72.
- Srivatsa S, Jacob S, Agarwal A. Contact lens assisted corneal cross linking in thinectatic corneas - A review. Indian J Ophthalmol. 2020;68(12):2773-2778. doi:10.4103/ijo.IJO_2138_20
- Malhotra C, Gupta B, Jain AK, Dhar S, Gupta A, Balyan M. Comparison of contact lens-assisted and transepithelial corneal crosslinking with standard epithelium-off crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2022 Feb 1;48(2):199-207. doi: 10.1097/j.jcrs.0000000000000732. PMID: 34174043.
- Subasinghe SK, Ogbuehi KC, Dias GJ. Current perspectives on corneal collagen crosslinking (CXL). Graefes Arch Clin Exp Ophthalmol. 2018 Aug;256(8):1363-1384. doi: 10.1007/s00417-018-3966-0. Epub 2018 Apr 6. PMID: 29623463.
- Hafezi F, Kling S, Gilardoni F, Hafezi N, Hillen M, Abrishamchi R, Gomes JAP, Mazzotta C, Randleman JB, Torres-Netto EA. Individualized Corneal Cross-linking With Riboflavin and UV-A in Ultrathin Corneas: The Sub400 Protocol. Am J Ophthalmol. 2021 Apr;224:133-142. doi: 10.1016/j.ajo.2020.12.011. Epub 2021 Jan 30. PMID: 33340508
- Kling S, Hafezi F. An Algorithm to Predict the Biomechanical Stiffening Effect in Corneal Cross-linking. J Refract Surg. 2017 Feb 1;33(2):128-136. doi: 10.3928/1081597X-20161206-01. PMID: 28192592.
