
In November of 2015, Alcon released Contoura® topography-guided LASIK into the US market. Contoura brought over 100,000 topographic data points into the excimer treatment for each eye instead of simply the standard 2 keratometric indices (steep K and flat K). This was coupled with a blazing fast eye tracker running at 1050 Hz and synchronized to the laser frequency at 500 Hz, yielding a 2 millisecond latency time.
The Gaussian beam was ultra-thin at a 0.68 mm spot size. Here was the future of LASIK—and it performed amazingly well in the US FDA study with 92.6% of eyes achieving 20/20 vision or better and 64.8% experiencing 20/16 vision or better.1 Patient post-operative vision quality was also improved with statistically significant reductions in glare, light sensitivity, difficulty driving at night, and difficulty while reading.1
Yet, when Contoura was released to the US market, it flopped. The FDA study had no less than three corneal specialists evaluating every cornea and agreeing it had perfect topography before it was allowed into the study. But, in the average clinic, patient selection can often be messy. Most corneas (approximately 80 to 90%) are not “perfect.”
Time is precious and surgeons couldn’t spend hours on a single eye’s calculation. The addition of topographic data led to greater complexity and difficulty in determining the correct treatment. The WavelightR Contoura treatment may have had great power, speed, and potential, but it was wasted if the average surgeon using it became frustrated trying to bring it all to bear.
What was needed was new technology to assist the surgeon in driving the powerful topography-guided excimer laser. Phorcides Analytic Engine was developed to meet this need. Phorcides uses geographic imaging software (GIS) to analyze the two-dimensional corneal topographic treatment image produced by the Alcon Contoura planning laptop (Figure 1) and pulls detailed information about the complex three-dimensional cornea (Figure 2).
Figure 1 , below, represents topography-only corneal ablation profile from the Alcon planning laptop.

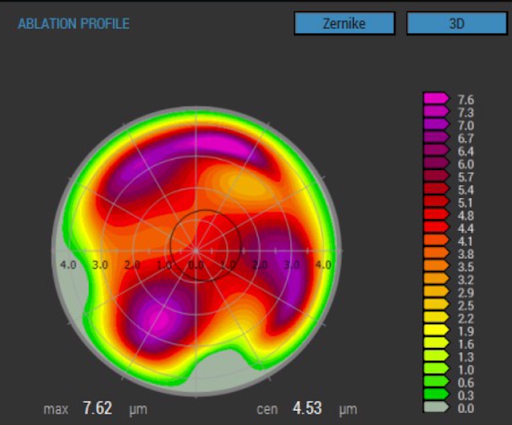
Figure 1
Figure 2 shows phorcides geographic imaging software (GIS) topography refractive analysis of an Alcon planning image.

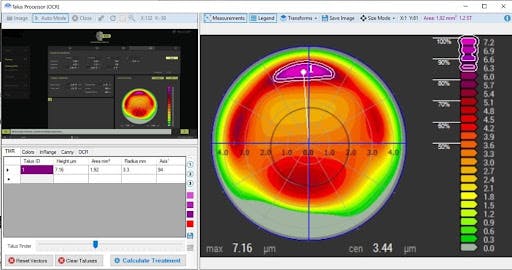
Figure 2
The software then compiles a series of refractive vectors: one vector for each raised topographic feature on the corneal surface, one vector for the anterior corneal astigmatism, one vector for the posterior corneal astigmatism, and one vector for any internal lenticular astigmatism. Finally, it uses a series of advanced computer algorithms to determine the best treatment for each eye (Figure 3).
In Figure 3, we see vector analysis and treatment recommendation.

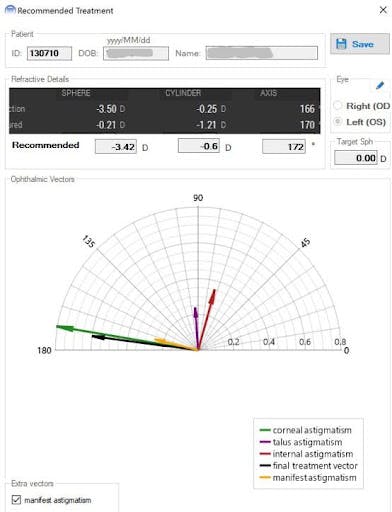
Figure 3
While the analysis is complex, the surgeon’s experience is fast and seamless with treatments calculated in under 10 seconds. What are the results? Exceptional patient experiences with optimal vision. Table 1 shows a comparison of outcomes for current refractive surgery techniques.
Table 1 (below) illustrates the percent of eyes with uncorrected visual acuity greater or equal to 20/20. Data shown is 3 months postoperative for Phorcides Contoura,2 FDA Contoura,1 WFO,3 WFG,3 and Ray Tracing.4 Data shown for SMILE5 is at 6 months postoperative time.

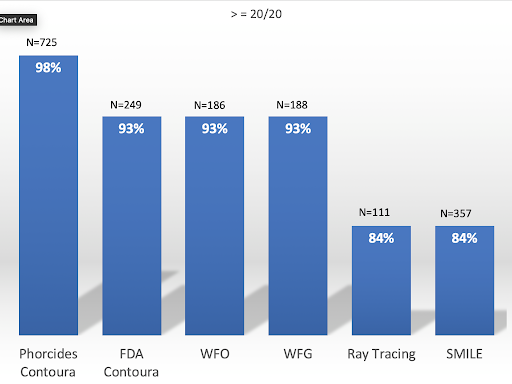
Table 1
The data for the Phorcides Contoura group comes from a retrospective analysis of 5 US clinics examining 725 eyes.2 From this analysis, 100 % of eyes achieved visual acuity of 20/25 or better, 98.3% 20/20 or better, and 60.1% 20/15 or better at 3 months postoperative time. Over half of the eyes achieved 20/15 or better which provides surgeons the opportunity of a new vision “normal” beyond 20/20.
It’s worth noting that the Phorcides Contoura group delivered better results than the US FDA study, yet the FDA study severely restricted entry to only “perfect” corneas. The Phorcides Contoura cohort included all clinic patients, even the 90% of eyes with mildly abnormal corneal topographies that led the manifest astigmatism to differ from the measured anterior corneal astigmatism.
Surprisingly, Phorcides Contoura delivered far superior results to ray tracing LASIK, the technology that is supposed to supplant topography-guided LASIK in the future.
Notwithstanding the positive results described above, great patient outcomes from LASIK go beyond just achieving 20/20 or 20/15 uncorrected visual acuity. Not all 20/20 vision is the same quality. Two patients can read a 20/20 line on the Snellen chart but they may not be seeing the same crisp outline of each letter.
Figure 4 illustrates the Snellen chart as viewed by a patient with no aberrations on the left and with a small amount of coma on the right. Contoura allows for the correction of topographic irregularities on the corneal surface that generate higher-order aberrations such as coma. When these are eliminated, the result is a patient vision of higher quality. All of this translates into a better experience for the patient and the surgeon.
Figure 4 represent image quality affected by coma (right).

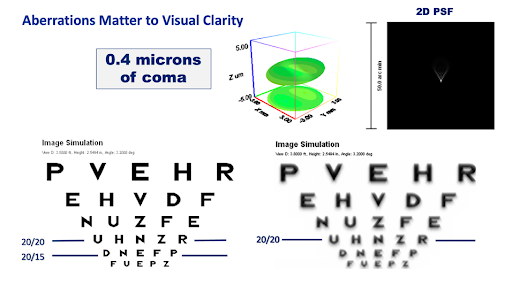
Figure 4. *Used with permission from Alcon
Disclosures: Dr. Lobanoff is the founder and owner of Phorcides LLC and a paid consultant for Alcon.
References:
- FDA Clinical Trials. Allegretto Wave Eye-Q Addendum Procedure Manual T-CAT Topography-Guided Treatments. http://www.accessdata.fda.gov/cdrh_docs/pdf2/P020050S012d.pdf
- Lobanoff M, Mann M, Stonecipher K, Tooma T, Wexler S,. Clinical Outcomes after Topography-guided LASIK Calculated with New Topography Analysis Algorithm: Retrospective Results from 5 US Clinics. Dovepress, In press
- Stonecipher K, Kerzirian G. Wavefront-optimized Versus Wavefront-guided LASIK for Myopic Astigmatism with the ALLEGRETTO WAVE: Three-month Results of a Prospective FDA trial. J Refract Surg. 2008 Apr;24(4):424-30
- Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical Ray Tracing-guided Laser In Situ Keratomileusis for Moderate to High Myopic Astigmatism. J Refract Surg. 2012 Jan;38(1):28-34.
- Sekundo W, Kunert K, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011 Mar;95(3):335-9
- Stonecipher K. Topography Guided Laser Outcomes Using a New Vector Software Program (Phorcides). ESCRS, 2019 Sep