


I was fortunate to have been one of the original investigators of the excimer laser way back in 1989, six years prior to its FDA approval in 1995.

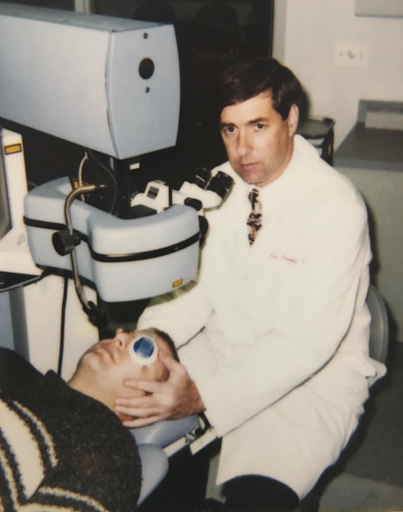
Fig 1 Performing LASIK in 1995.
Over the last 32 years, I have performed over 100,000 refractive laser procedures and have learned a great deal in the process. I have witnessed and participated in all of the advances in technology including pupil tracking (yes, in the beginning we had to aim the laser manually), advanced ablation profiles, femtosecond flap formation, wavefront aberrometry, and topographic ablations. Despite these wonderful technological advances I am absolutely convinced that the preoperative examination is the most important aspect of being a quality refractive surgeon.
Choosing the right procedure for a given patient and knowing when to say “no” to refractive surgery when it is not in the best interests of the patient has been an ongoing learning experience.
The preoperative evaluation is the key to surgical success and beneficial postoperative outcomes. Any abnormal finding should be documented and discussed with the patient. I have a motto that I abide by for all surgical procedures: “a finding prior to surgery sets an expectation. The same finding discussed postoperatively becomes the surgeon’s complication.”
The preoperative evaluation starts with an accurate patient history. Patients with an active lifestyle and increased risk of traumatic flap dislocation or pre-existing epithelial basement membrane dystrophy may be better candidates for photorefractive keratectomy (PRK). A history of tearing, foreign body sensation, or visual fluctuation is suggestive of dry eye disease. It has been demonstrated that the safety of LASIK is not affected by pre-existing dry eye.1
However, pre-existing dry eye is a risk factor for symptomatic post-LASIK dry eye with measurably lower tear function and supra-vital staining of the ocular surface.1 We consider conjunctival staining a risk factor for dry eye postoperatively and corneal staining to be a relative contraindication for surgery. In patients who have dry eye symptoms preoperatively, it is important to maximize the health of the ocular surface prior to initiating surgery, as it is easier to pre-treat these patients than to react to them postoperatively.
The most common reason patients present for refractive corneal surgery is contact lens intolerance. Every year 4 million Americans discontinue contact lens wear and the overwhelming reason is dry eye disease. All patients presenting for a LASIK examination should have a dry eye evaluation.2
I do not perform a Schirmer’s test, but every patient seen in my office has a tear osmolarity, which in my opinion is the most sensitive test for dry eye. A measurement in either eye of over 308 or a difference between the two eyes of greater than 8 mOsm/l bilaterally is a strong predictor of dry eye. In addition, a high osmolarity has a deleterious effect on keratometry reducing surgical accuracy.3
In addition, I find lissamine green staining to be very helpful as it is more sensitive than fluorescein staining. However, whether you use lissamine green or fluorescein, any central corneal staining is a surgical stoplight for me to treat the dry eye prior to LASIK.
In the preoperative evaluation, do not forget to evaluate the eyelids. Meibomian gland dysfunction is the most common cause of dry eye. Look for inspissated meibomian glands and compress the lids to evaluate the quality of the secretions. I now also have the patient look down to evaluate the patient for cylindrical collerettes, which are pathognomonic for demodex that is highly associated with dry eye. A new technology, which is not universally employed, but I find very helpful for evaluating lid pathology, is meibography.
Finally, all refractive surgery candidates should have a topography or tomography. Irregular images or drop out of information is very suggestive of dry eye disease. All patients with aqueous deficient and/or evaporative dry eye should be treated preoperatively to improve their candidacy, refractive accuracy, and post surgical satisfaction.
The next evaluation I concentrate on is the corneal topography or tomography. The quality of the cornea curvature looking for forme fruste keratoconus is the most important risk factor for the development of ectasia. Conversely, I find the thinnest pachymetry to be of a much lesser value in evaluating risk factors for ectasia. In looking at the topography, make certain to use a scale that is not too sensitive as to find irregularities that are not significant but that also capable of picking up irregularities (I use a scale with 1.5D increments).
Forme fruste keratoconus is a topographic diagnosis, rather than a clinical one. It is not a variant of keratoconus. Asymmetric inferior corneal steepening or asymmetric bowtie topographic patterns with skewed steep radial axes above and below the horizontal meridian are risk factors for progression to keratoconus and ectasia after LASIK.4
Figure 2, below, depicts skew deviation.

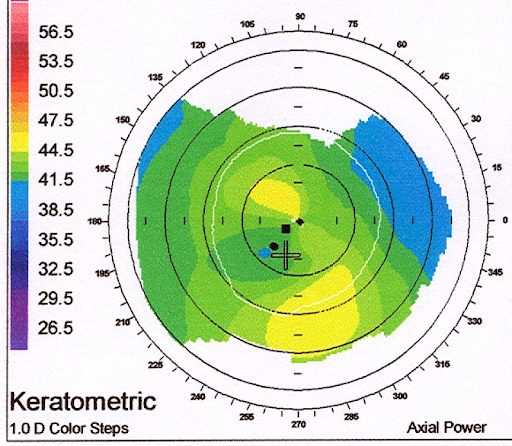
Figure 2
Patients with these topographic patterns who are stable could be offered photorefractive keratectomy (including the option for transepithelial photorefractive keratectomy) with informed consent, indicating that there may still be a risk for progression to keratoconus. Patients with an inferior “crab-claw” pattern accompanied by central flattening (“blue spot”) are at risk for the development of pellucid marginal degeneration even if there are no clinical signs of it. This pattern should be designated as a pellucid suspect and LASIK should be avoided in eyes exhibiting this topographic pattern.
Smart software incorporated into many topographers may help diagnose forme fruste keratoconus but may register as normal in patients with pellucid marginal degeneration. I do look at the posterior float but a readily available bit of information that can be very helpful is a pachymetry map. The apex of the cornea should be near its center and should also be the thinnest location.
Figure 3: Thinnest pachymetry is decentered from optical apex.

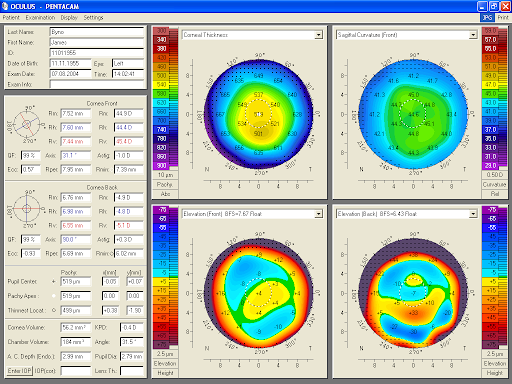
Figure 3
When the thinnest area of the cornea is not at the apex, especially in the setting of an unusual topography, I regard this as a significant risk factor for ectasia.
Additionally, I would suggest a physical finding and new test are very helpful in the preoperative LASIK examination. I have been impressed by how often patients with post LASIK ectasia have floppy eyelid syndrome. Many of these patients also have sleep apnea and sleep on their side with their hand or pillow pressed against their eye. They frequently have asymmetric ectasia with the more involved eye being the side they sleep on and having the worse floppy eyelid syndrome as well.
I now screen for floppy eyelid syndrome in all patients considering LASIK and add this to the information I receive from their topography.
Figure 4 shows the sleeping habit of patient with floppy eyelid syndrome.


Figure 4
The new test that I now employ is Avagen, the first genetic test to quantify risk factors for keratoconus by evaluating 75 genes and over 2,000 variants. I find the Avagen test for keratoconus to allow for more accurate decision making in patients considering LASIK who might otherwise have subtle risk factors that would previously have influenced me to perform PRK or no surgery at all.
I am deeply committed to a well-informed patient, which is why I value the time in consult and the fostering of honest patient rapport. However, I am aware the consultation is likely not the only source of information for a patient, which is why I point them to reliable educational resources online. For more than a decade I have served on the Refractive Surgery Council (RSC), supporting its mission to educate the public on vision correction options by publishing content designed to answer prospective refractive questions.
As an editorial advisor, I know the content on the RSC site is relevant, clinically accurate and designed to help patients reach an informed decision about laser vision correction. Articles like these, and many others, help prepare patients for their consult: “Your Eye Doctor Will See You Now: Tips for Your Virtual Eye Care Visit,” “Are You a Candidate for LASIK?5 Guidelines You Should Know,” and “Your LASIK Consultation: A Deeper Look Into What to Expect.”
The RSC’s robust library of patient-friendly articles is available to eye doctors, making it easy for any practice to incorporate patient education into a blog and social media platforms. It is a great resource that is readily available to practices.
Finally, below are my LASIK pearls which have been curated over the last 30 years.
Donnenfeld LASIK Pearls
- If you can refract the eye to good visual acuity, you can usually treat the patient to good visual acuity.
- If you cannot refract the eye to good visual acuity and you cannot capture a good wavefront or topographic treatment, you cannot treat the patient to good visual acuity. Look for corneal scars, epithelial basement membrane dystrophy, central islands, keratoconus, and amblyopia.
- Do not treat patients with ocular surface disease. They are refractively unpredictable, and an enhancement will worsen ocular surface disease. Corollary to Rule #3: Resolve the ocular surface disease and the patient will become a good candidate for a treatment.
- Do not treat patients with unstable refractions especially with progressive myopia as it is difficult to hit a moving target and it is the earliest sign of a nuclear sclerotic cataract and ectasia.
- Beware of treatments, which will leave the cornea too flat, too steep, or too thin. I prefer postoperative Ks < 49.5 or > 33.
- Patients with previous corneal surgery often have less predictable outcomes with PRK including penetrating keratoplasty, radial keratotomy and LASIK.
- When in doubt do PRK. Avoid flap recuts and lifting flaps after 3 years.
- Beware of unrealistic expectations. Mild amblyopic patients do not get 20/20 vision; presbyopes will not be able to see near; monovision patients will not have perfect distance vision.
- Beware of the presbyopic hyperope. Hyperopic ablations are not as accurate as myopic ablations and hyperopia returns over time. Consider clear lens extraction.
- Presbyopic patients are never completely happy. Monovision may make them less unhappy, but their distance vision is never as good as it was when they had binocular distance correction and reading with monovision is never as good as it was with a good pair of reading glasses.
- Presbyopic low myopes will never forgive you for correcting them to plano (you cannot take off your glasses once you have had refractive surgery). I strongly recommend a contact lens trial before considering surgery on a presbyopic low myopic.
- Listen to your staff. When they warn you about a patient having unrealistic expectations they are almost always correct.
In conclusion
In conclusion, LASIK is one of the most studied, safest, and highest satisfaction elective surgical procedures available. LASIK dramatically improves quality of life and every day function. A thorough preoperative evaluation is the key to optimizing results and improving patient outcomes.
References
- Yu EY, Leung A, Rao S, Lam DS. Effect of laser in situ keratomileusis on tear stability. Ophthalmology. 2000 Dec;107(12):2131-2135.
- Donnenfeld ED, Solomon R, Perry HD. Prevention and Management of Dry Eye Following LASIK. In: Probst L (ed). LASIK Advances, Controversies, and Custom. Ch. 15, Thorofare, NJ: SLACK, Incorporated, pp. 187-194, 2004.
- Epitropoulos AT Matossian C, Berdy GJ, Malhotra RP, Potvin R . Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refractive Surgery,41 (8) 1672-7, 2015.
- Binder PS, Lindstrom RI, Stulting RD, Donnenfeld E, Wu H, McDonnell P, Rabinowitz Y. Keratoconus and corneal ectasia after LASIK. J Refract Surg 21:749-252, 2005
- Solomon KD. Fernandez de Castro LE, Sandoval HP, Biber JM, Groat B, Neff KD, Ying MS, French JW, Donnenfeld ED, Lindstrom RL; Joint LASIK Study Task Force. LASIK world literature review: quality of life and patient satisfaction. Ophthalmology 116:691-701, 2009
- Sandoval HP, Donnenfeld ED, Kohnen T, Lindstrom RL, Potvin R, Tremblay DM, Solomon KD. J Cataract Refract Surg. 2016 Aug;42(8):1224-34
