



A growing number of patients who have had previous laser refractive surgery are presenting to our practices for cataract surgery.1-4 However, intraocular (IOL) calculations and meeting patient expectations can sometimes prove challenging after a patient has had laser vision correction; the combination of possible inaccurate biometry, variable refractive targeting, and high patient expectations regarding visual outcome requires extra steps on the surgeons’ behalf.1-6
Although cataract surgery can be successfully performed after LASIK, it is important to carefully detail preoperative steps, as well as patient education, to ensure optimal visual results.
When to consider the timing of post-LASIK cataract surgery
In general, cataract surgery is performed years after LASIK; there is no time limit (short or long) for when cataract surgery can be done after a patient has had LASIK. However, if the patient is presenting for a cataract evaluation within a few months of LASIK surgery, it is important to investigate why (e.g., what are the relevant patient complaints). Was the patient previously diagnosed with cataracts prior to LASIK surgery? Are cataracts acute or in relation to trauma or systemic disease? These factors all play a role in surgical planning.1,2,5
Preoperative considerations for cataract surgery after LASIK
With any patient who is post-LASIK, a scrutinizing examination of the ocular surface, topography, tomography, and higher order aberrations (HOA) is critical. Moreover, if the patient wishes to consider a diffractive premium IOL technology, nuanced assessment of pre-existing aberrations is necessary.1,6-11
When planning cataract surgery, especially with respect to IOL calculations, accurate axial length and keratometry readings are very important. Any historical data (pre-LASIK keratometry and refraction) is important, as this can help guide IOL selection. Unfortunately, it is quite common for patients to not have access to this data. However, we do have excellent resources to get around this; for example, post-refractive surgery calculators such as the ones provided by the American Society of Cataract and Refractive Surgery (ASCRS) can help best calculate the appropriate IOL power.1-5
Additionally, intraoperative aberrometry can be used to confirm the IOL at time of surgery (e.g., ORA, Alcon, Fort Worth TX).1-5 Missed refractive result is also possible due to history of LASIK, and the patient should be counseled regarding this and what options are available in such an occurrence (e.g., glasses, IOL exchange, laser vision correction enhancement).1-5,10,12
In general, it is recommended for total HOA to be <0.3µm to plan for optimal results with a multifocal IOL.1,13 Devices such as the Pentacam (Oculus, Arlington WA), OPD-3 (Marco, Jacksonville FL) and iTrace (Tracey Technologies, Houston TX) can be helpful for measuring HOA.1,2,13 If the patient has acceptable preoperative HOA, optimized ocular surface, and is willing to accept the risk of visual disturbance associated with multifocal IOL implantation (and has been educated that an IOL exchange can be performed, if necessary), then it may be reasonable to proceed with a presbyopia-correcting IOL.1-3,5,6,12-15
It is always advisable to counsel the patient of increased risk of glare, halos, and starburst as well as decreased contrast sensitivity with diffractive multifocal IOLs due to past history of laser vision correction.1-3,5,6,10,12-15
Alternatively, an extended depth of focus IOL (Vivity, Alcon Fort Worth TX or Symfony, Johnson & Johnson Vision, Jacksonville FL) may be used with a slightly lower risk of visual aberrations, though near vision may be limited in comparison to trifocal IOLs.1-3,5,6,10,12,13-15
It is also important to examine the eyes and topography for signs of decentered ablations (Figure 1) as well as post-LASIK ectasia (Figure 2). If ectasia is present, it is necessary to determine if the ectasia is stable or progressing. Though it is unusual to have ectasia progression after age 40-45, it can occur. Additionally, in the case of progressive ectasia, corneal crosslinking should be performed to halt progression.16,17 Once the cornea has stabilized (which can take several months), planning for cataract surgery can be performed.
IOL options for a cataractous eye with post-LASIK ectasia do include toric monofocal IOLs. Bausch and Lomb Envista IOLs come in higher toric powers, which can be very helpful in higher levels of corneal cylinder. Alcon and Johnson & Johnson Vision toric IOLs have also been documented to give good results in these patients.13,16-18
In the case of stable, but severe/irregular ectasia, it may be best to implant a monofocal (i.e., non-toric IOL), and have the patient fitted for a contact lens postoperatively; topography-guided photorefractive keratectomy (PRK) may be an option in some cases as well.16-18
Figure 1 demonstrates de-centered, old LASIK ablation.

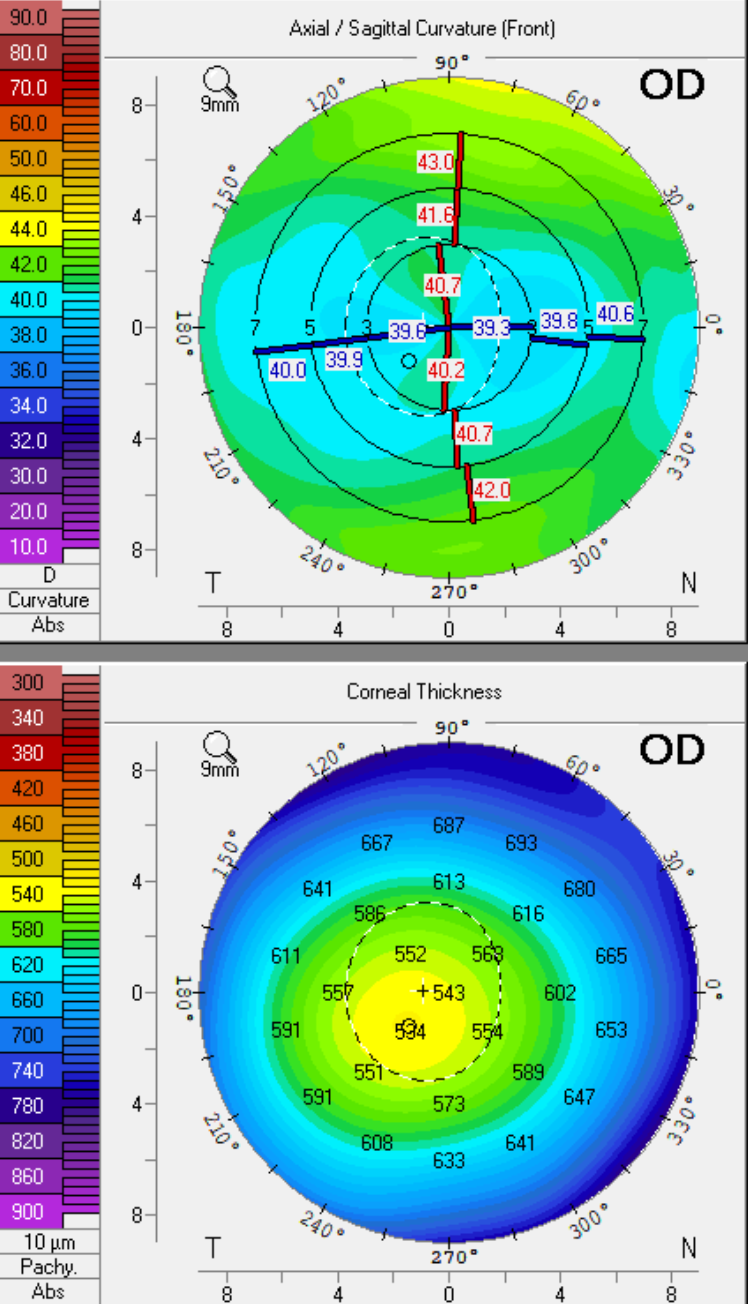
Figure 1
Figure 2 represents post-LASIK ectasia.

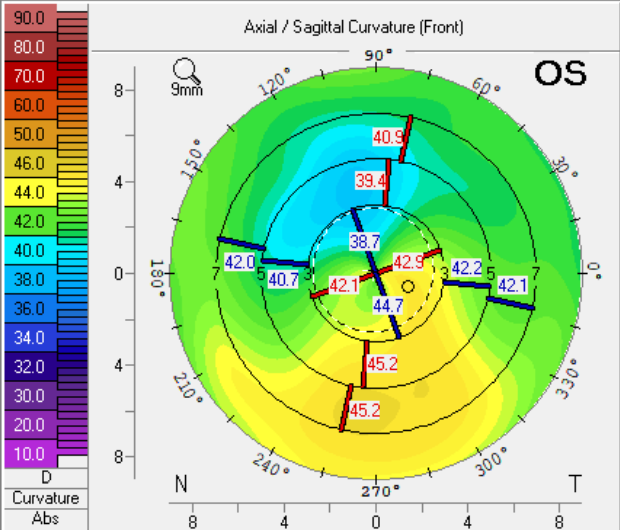
Figure 2
Postoperative considerations of post-LASIK cataract surgery
In general, post-LASIK cataract patients should follow a routine healing course. However, there are a few things to look out for that are specific to these post-refractive eyes.
Anatomical considerations
With most contemporary cases of cataract surgery, a limbal clear corneal incision is created. Care should be taken to avoid catching the edge of the LASIK flap during this incision (or any incision, for that matter) creation, as this can potentially cause flap dislocation, striae, and delayed visual recovery. The edge or a sector of the LASIK flap may become edematous postoperatively, leading to decreased vision, irritation, and a slightly prolonged healing period. 1,2
In general, as long as the flap remains in a good position, no extra steps need to be taken, and observation is usually all that is required. However, the patient may need to be monitored slightly more frequently until the flap edema resolves, to ensure a good visual recovery without new flap striae or development of a fluid cleft.
Visual Acuity
As discussed above, due to inaccuracy in preoperative measurements in post-LASIK eyes, it is possible to have a missed refractive target. The latter is especially noticeable in patients who have multifocal IOLs implanted at the time of surgery. 1-5,10,12,14,15 It is important to give the eye an adequate time to heal. Often, two to three weeks postoperatively is not enough time to assess for the final visual result, as even microscopic flap edema may cause blurred vision. 1-5,10,12,14,15
Instead, it may take four to six weeks for the vision to stabilize after cataract surgery in these patients, and they should be educated and reassured appropriately. In the case of a missed refractive target and a consequently unhappy patient, there is a step-wise approach to management to help improve the patient’s vision.
In a patient with a substantial refractive error, options for correction range from glasses, contact lenses, laser corrective procedures, as well as IOL exchange. 1-5,10,14,15 Some patients may choose to use glasses or contacts, whereas others that wish to remain free from spectacles or contacts may choose laser vision correction (this may be especially true for patients who have had multifocal IOL implantation). 1-5,10,12,14,15 In the case of a large refractive miss, the surgeon may need to weigh the risk/benefits of performing a repeat laser ablation versus IOL exchange.
When considering laser vision correction (enhancement) post-cataract surgery in a post-LASIK eye, a proper refractive surgery evaluation is necessary. This includes assessment of the ocular surface, determining refractive stability (i.e., that the vision has stabilized post-cataract surgery), topography, tomography, pachymetry, and determining if laser vision correction can be performed safely. 7-9,12,14,15
Oftentimes, it may not be possible to lift the previously created LASIK flap for enhancement surgery, therefore, PRK may be used as an alternative for refractive error treatment. It is important to carefully plan the refractive enhancement and discuss all risks associated with repeat laser vision correction, including overcorrection, undercorrection, and increased risk of visual disturbances (e.g., glare, halos) postoperatively. 7-9,12,14,15
Visual disturbances
Fortunately, in most patients who undergo cataract surgery with monofocal IOL implantation, visual disturbances are rare. The risk of postoperative glare and halos increases in these post-refractive patients once a multifocal (especially diffractive-IOL-based technology) IOL is implanted. 6,10,11,14,15,19,20
Elaboration of symptoms is important here: Are glare and halos mainly nocturnal in nature or occur during the day as well? A thorough ocular exam, including uncorrected and best-corrected visual acuity, as well as anterior and posterior segment exam, should be performed.
It is important to remind the patient that often the presence of glare and halos will diminish over time post-surgery. 6,10,11,14,15,19,20 As the eye heals and neuroadaptation occurs, the patient may not notice these visual aberrations much or at all. 6,10,11,14,15,19,20 In addition, during this early postoperative healing period, the use of topical brimonidine as needed for glare/halos has been documented to help reduce nocturnal visual aberrations.6,10,11,14,15,19,20 However, it is also important to search for other causes of visual disturbances.
Occasionally, residual refractive error can lead to visual aberrations–if this is the case, determination of how to best treat this (glasses, contacts, laser vision correction) can be explored. 6,10,11,14,15,19,20 Inspection of the ocular surface is also incredibly important, as even mild dry eyecan cause fluctuations in vision; the presence of a diffractive IOL can accentuate these disturbances and can become bothersome both during the day and at night. 6-11,15,19,20
Intensive treatment of ocular surface disease as well as meibomian gland dysfunction and blepharitis, is key for all cataract surgery patients to best optimize vision. 6-11,15,19,20
Centration of the IOL is also important–even slight decentration or malposition can lead to increased higher-order aberrations and visual dissatisfaction (this is especially true for toric mulitifocal IOLs). 6,10,11,14,15,19,20
When possible, IOL decentration should be managed early and surgically in order to best optimize vision. If there is a compromise of the capsular bag and the IOL is unstable, the patient should be informed of the need for IOL exchange for a monofocal, as a compromised capsular bag will ultimately lead to further IOL decentration and worsening visual aberrations and decline.
The presence of early posterior capsule opacification (PCO) is one of the most common causes of visual disturbances post-multifocal IOL implantation.6,10,11,14,15,19 If this is the case, the patient can be educated on the option of YAG capsulotomy to help improve symptoms.6,10,11,14,15,19 However, it is advised to wait at least two to three months postoperatively in order to ensure the patient is otherwise satisfied with the extended range of vision from the IOL, as IOL exchange post-YAG is significantly more difficult to perform.6,11,14,15,18,19
Conclusions
Cataract surgery after LASIK can be successful but it is important to remember to check for anatomical nuances that may be present during the pre- and postoperative period and contribute to visual dissatisfaction. Proper patient education regarding cataract surgery post-LASIK is of utmost importance and must include the possible need for further surgery, glasses, or contact lenses as well as why their eye is different from a surgically naïve eye. Fortunately, with clear communication and precise surgical planning, post-LASIK patients can become incredibly happy pseudophakic patients!
References
- McDonald M, Maloney R, Kanellopoulos AJ, Epitropoulos A, Khodabakhsh AJ. Take Care with Cataract Surgery After LASIK. Cataract and Refractive Surgery Today. August 2018
- Raviv T. Choosing an IOL After LASIK. Cataract and Refractive Surgery Today. July 2014
- McCarthy M, Gavanski GM, Paton KE, Holland SP. Intraocular lens power calculations after myopic laser refractive surgery: a comparison of methods in 173 eyes. Ophthalmology. 2011; 118(5): 940-944
- Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology. 2014; 121(1): 56—60
- Tang M, Wang L, Koch DD, Li Y, Huang D. Intraocular lens power calculation after previous myopic laser vision correction based on corneal power measured by Fourier-domain optical coherence tomography. J Cataract Refract Surg. 2012; 38(4): 589-594
- Rudalevicius P, Lekaviciene R, Auffarth GU, et al. Relations between patient personality and patients’ dissatisfaction after multifocal intraocular lens implantation: clinical study based on the five factor inventory personality evaluation. Eye. 2020; 34(4): 717-724
- Trattler WB, Majmudar PA, Donnenfeld ED, et al. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) Study: the effect of dry eye. Clin Ophthalmol. 2017;11: 1423-1430
- Luchs JI, Buznego C, Trattler WB. Asymptomatic or minimally symptomatic blepharitis in patients having cataract surgery. Poster presented at: American Society of Cataract and Refractive Surgery Annual Meeting; May 25-29, 2011; San Diego CA
- Epitropoulos AT, Matossian C, Berdy GJ, et al. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41:1672-1677
- Gibbons A, Ali TK, Waren DP, Donaldson KE. Causes and correction of dissatisfaction after implantation of presbyopia-correcting intraocular lenses. Clin Ophthalmol. 2016; 10(10): 1965-1970
- Bizer W. How can I reduce halo and glare from my multifocal lenses after cataract surgery? American Academy of Ophthalmology. 2013
- Ayala MJ, Perez-Santonja JJ, Artola A, Claramonte P, Alio JL. Laser in situ keratomileusis to correct residual myopia after cataract surgery. J Refract Surg. 2001; 17(1): 12-16
- Kim CY, Chung S, Kim T, Cho YJ, Yoon G, Seo K. Comparison of Higher-Order Aberration and Contrast Sensitivity in Monofocal and Multifocal Intraocular Lenses. Yonsei Med J. 2007;48(4): 627-633
- Gunvant P, Ablamowicz A, Gollamudi S. Predicting the necessity of LASIK enhancement after cataract surgery in patients with multifocal IOL implantation. Clin Ophthalmol. 2011;5: 1281-1285
- Macsai MS, Fontes BM. Refractive enhancement following presbyopia-correcting intraocular lens implantation. Curr Opin Ophthalmol. 2008;19(1): 18-21
- Wollensak G., Spoerl E., Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. May 2003;135(5):620–627
- Nattis AS, Rosenberg ED, Donnenfeld ED. One-year visual and astigmatic outcomes of keratoconus patients following sequential crosslinking and topography-guided surface ablation: the TOPOLINK study. J Cataract Refract Surg. 2020 Apr;46(4):507-516
- Allard K, Zetterberg M. Implantation of toric intraocular lenses in patients with cataract and keratoconus: a case series. Int Med Case Rep J. 2018; 11:185-191
- Rosa A, Miranda A, Patricio MM, et al. Functional magnetic resonance imaging to assess neuroadaptation after bilateral cataract surgery. Ophthalmol. 2013;120(12): 2449-2455.e1
- Lee J, You Y, Choe C, Lee E. Efficacy of brimonidine tartrate 0.2% ophthalmic solution in reducing halos after laser in situ keratomileusis. J Cataract Refract Surg. 2008; 34(6): 963-967
