From November 18 to 20, 2022, eyecare practitioners (ECPs) from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from David L. Kading, OD, FAAO, FCLSA, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
The
prevalence of myopia has increased by 66% in the United States since the 1970s, and it continues to rise across the globe. In parts of China, 90% of children graduating from school have myopia. In fact, the Chinese government recognizes that this disease state will have significant visual and ocular ramifications for the future of these children.
Consequently, there are optometry schools and centers opening across China to try to manage this rise in myopia, potentially stifle disease progression, and protect against the risk of permanent vision loss. The Chinese government has mandated changes in schools, such as increasing lighting in classrooms and implementing vision therapy exercises throughout the day, in the hope of mitigating the effects of myopic progression.
The United States should and will need to take a firmer stance on myopia management. In my opinion, our greatest challenge surrounding myopia is not that we don’t have
myopia treatments but the refusal to call it a disease. The fact of the matter is there is a paucity of optometrists and ophthalmologists who recognize it as this type of progressive entity or are taking the necessary steps to include myopia management as a treatment program.
Interest in the myopia epidemic is rising
Between 2019 and mid-2022, over 1,000 scholarly articles were written focusing on the rise of myopia, and this research has provided us with a plethora of startling statistics. Interestingly enough, the increase in myopia didn’t just happen over the span of 30 or 40 years.
Between 2020 and 2022, researchers have identified what is being called “Quarantine Myopia,” where myopia in 6-year-old children rose from 5.7% to 21.5%. All told, that's an almost 16% rise in cases from just these 2 years, along with an eye-popping overall 277% change.
This means that in the US, optometry and ophthalmology practices are going to be seeing an influx of younger myopic patients. Although we have not been able to specifically map the genes associated with myopia, there appears to be a genetic, or at least familial, component. We know that if a child has two parents who are myopic, that child is six times more likely to be myopic. Children who are myopic prior to the age of 6 or 7 are also 6.6 times more likely to develop high myopia as an adult, which further increases the risk for progressive disease.
Figure 1 compares the increased risk of developing myopia in pediatric patients myopic family history.
Figure 1, courtesy of David L. Kading, OD, FAAO, FCLSA
We see the greatest progression of myopia occurring in children during the winter months and see a corresponding reduction during the summer months. This suggests a correlation between longer days,
spending time outdoors, and reduced screen time with the reduction of myopia. Uninhibited sunlight appears to be a key contributing factor in reducing myopia.
In addition to these trends, increased reading and higher education follow a similar trajectory for myopia progression, which suggests a correlation. Admittedly in my professional opinion, there are not enough randomized trials that have been done to state with authority there is causation.
How much myopia is too much?
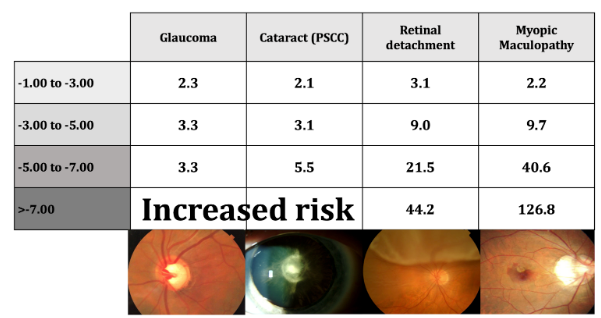
With every diopter increase in myopia, there is a 67% increase in myopic maculopathy. Increased myopia is also associated with
glaucoma, posterior subcapsular cataracts (PSC), and
retinal detachments. Even a patient with just one diopter (D) of myopia is twice as likely to develop glaucoma than an emmetropic patient.
When I see a 6- or 7-year-old who is a 1.00D myope, I imagine in the future that might progress to a -5.00 to -7.00D. That makes this patient over 20 times more likely to have a retinal detachment than someone who is emmetropic and 40 times more likely to develop myopic maculopathy.
As eyecare practitioners, we can do something about that because these increases in myopia have a life-long impact. Patients over the age of 75 who are (or were prior to cataract surgery) highly myopic patients have a 90% chance or more of having severe visual impairment.
Figure 2 compares ranges of diopter values to the corresponding rise in the risk of developing specific ocular diseases.
Figure 2, courtesy of David L. Kading, OD, FAAO, FCLSA
What are we doing to slow the progression of myopia?
Gas permeable lenses have been studied specifically to see if they slow the progression of myopia. It was found that they do not, and some studies even suggested they may have slightly increased the progression of myopia. Another common practice that has been attempted as a control mechanism is under-correction.
“In fact, multiple studies have shown that undercorrecting patients increased the amount of myopia.”
Studies show that prescribing spectacle bifocals may help slow myopia slightly but is more indicated for patients who have an eso posture or
accommodative dysfunction. In our practice, we prescribe vision therapy to treat accommodative issues rather than prescribing spectacles.
Spectacles
However, there is hope for spectacles in myopia management. There are spectacle lenses on the horizon, such as
MiYOSMART and
Stellest, which are currently being prescribed in other parts of the world that do appear to slow the progression of myopia. DIMS (defocus incorporated multiple segment) lenses will allow optometrists to manage myopia in young children. That being said, these lenses will likely be more expensive than a polycarbonate single-vision lens.
Soft multifocal contact lenses
Research shows giving younger patients higher add powers in the
soft multifocal lenses improves the results of myopia management. Of note, there is mounting evidence that soft multifocal lenses have a subtle amount of decentration in the pupil region, which allows for some crossover between the distance and near correction, contributing to a potential slowdown in myopic progression.
Furthermore, it appears the glare and halos that occur with these multifocal lenses, which often make them less than ideal for adult wearers, is the very thing that might contribute to the slowing of myopia in younger patients.
MiSight and NaturalVue lenses
Of course, I can’t give a State of the Union without talking about the
MiSight lens. This is the first FDA-approved device for myopia management in the United States. There has been a tremendous amount of research done on this lens, with 6 years of data illustrating a considerable reduction in the progression of myopia with respect to dampening the axial length curves (less than 0.5mm growth).
The other lens available is
NaturalVue, with a center distance design in a daily disposable modality which touts a larger power range (up to -12.25D) but less longitudinal data at 3 years total.
Atropine
Atropine is a common form of myopia management, and it appears that this is the direction that myopia management is headed. Atropine is just another example of how younger patients can tolerate these treatments much better than if we were to give atropine to a 35-year-old adult, who would be greatly impaired.
The Low-Concentration Atropine for Myopia Progression (LAMP) study shows that atropine slows both refractive error and axial length out to 36 months. It is also important to take into consideration the patient’s eye color. The LAMP study was conducted in Asia, where most children had darker-pigmented irises, which could have contributed to their higher tolerance.
In my office, we recommend prescribing patients atropine ophthalmic solution 0.05% whenever possible and decreasing if that concentration isn’t well-tolerated. It’s important to follow up with the patient by either having them come in for an appointment or calling them to check in, so you can evaluate how they’re tolerating the atropine. One pearl to share is that
tapering the atropine dosage might extend the effectiveness of reducing myopic progression.
Orthokeratology (Ortho-K)
Orthokeratology is a valuable treatment option for myopia management, either on its own or in conjunction with atropine treatment. Ortho-K uses a lens to both flatten the central cornea and steepen the mid-peripheral cornea, which reduces the elongation of the eye and, thereby progression of myopia. Research studies show a reduction in myopia between 47 to 64%, but in standard practice, where we might change or adjust treatments to best suit the patient, these numbers could actually be much higher.
“Orthokeratology can absolutely slow the progression of myopia.”
Unfortunately, only between 4 to 7% of all optometrists are currently taking on orthokeratology, but it is an incredible way to slow the progression of myopia, and I highly encourage you to add this tool to your practice. Another
benefit of adding ortho-K to your practice is that it has an incredible success rate with fitting. The 3-year SMART study showed that 80% of patients were successfully fit with the first set of lenses. Even young patients who are already high myopes can benefit from orthokeratology.
Starting up myopia management
I think it's important for you to understand that the population is getting more myopic, and getting into myopia management is not an easy thing because it means you’ll have to think differently.
You will need to ask yourself the following questions:
There may be an investment when you elect to move forward with introducing myopia management into your clinic. Most practices will be able to pay off any of the equipment that they purchase for myopia management within the first year. Ultimately, the barrier to entry of cost is a relatively simple one to overcome.
“One of the true barriers, though, is getting your team on board.”
One way to gain alignment is to find someone on your team, sit down with them, and explain in clear terms why you want to bring this into your practice. Additionally, you will need to tell this team member that you need to develop one other person who is going to be a champion and help bring this out to our patients and our staff. Having that staff member spearhead this new service will aid in the development of content and resources by learning through direct practice experience when
talking with parents or by
creating FAQ sheets.
What do we charge patients?
Failure to value your services means that you’re not going to be excited about them. Often with myopia management, practices charge a global fee that covers all of the follow-up visits, similar to a vision therapy clinic. Some people charge a la carte or per visit. After you decide how you’re going to charge the patient, then you need to develop a
cost model for your new patients versus your established patients.
“An important step to introducing any new service is having the proper paperwork.”
Develop an agreement that spells out what happens if they discontinue treatment or lose or break a lens. Our office came up with a warranty policy for patients if they lose or break a lens. Then, create a video that explains myopia management and shows some statistics, and share that video on your social media. Explain to patients why it’s important.
If you don’t create demand, it's going to be very difficult. So, get out there and
talk to your community, start marketing with Google Ads or Facebook, and talk to pediatricians, naturopaths, and pediatric offices. The people crushing it in myopia management are doing this very thing. It’s not complicated—it just takes a little bit of time.
“I recommend that you designate 2 hours a week to lay out what needs to be done to get this accomplished.”
Myopia management can exponentially grow your practice in just a few years. It’s not difficult for myopia management to become 10 to 25% of the total revenue in your practice.
The final word: What’s next?
The most important lesson to take away is that you are not just doing this for the money but primarily in the name of patient care, with consideration given to
slowing down myopia-related pathology, including maculopathy inclusive of choroidal neovascularization, glaucoma, and peripheral retinal disease (i.e., retinal detachment, retinal tears, lattice degeneration, and more). Ultimately, we are making our best effort to stop it at the source rather than letting the disease progress.
We’re at a tipping point, and we need all ECPs to do their part in decreasing the progression of myopia for today, tomorrow, and the future for our children’s visual quality of life.