


Medical Management of Myopia
Worldwide, 1.5 billion people already have myopia, and it is estimated that by the year 2050, half of the world's population will be myopic.1 This is devastating because myopia is not just a refractive condition but strongly associated with diseases like retinal detachments, glaucoma, and maculopathy.
As optometrists, our primary objectives are to:
- Prevent or delay the onset of myopia
- Slow the progression of the disease
- Monitor the health of patients with high myopia
With these goals in mind, it’s important to understand:
- How to identify patients for treatment (who would benefit most from intervention)
- What the risk factors are
- What technology is best to manage these patients
- What treatments are most effective
Risk Factors
The following factors will increase a patient's risk for myopia progression:
- Asian ethnicity
- Age of onset—being less than 10 years old or less than 0.75 diopters of myopia by age six
- Female gender
- Parental myopia—having two myopic parents increases risk more than just one parent
- Behavioral—patients that routinely spend more than two hours a day on screens or less than two hours a day outdoors
Studies comparing the progression of myopia during the pandemic compared to pre-pandemic demonstrated a concerning trend. One study looked at a group of school-age kids, pre-pandemic, and found a rate of progression of myopia over a year's time at about one diopter in 10 percent of those kids. When researchers studied the same age group during the pandemic, 47 percent of those kids progressed in myopia one diopter or more.2
The combination of more screen time and near work paired with less time outside has been shown to increase myopia risk. In general, if your patients have two or more risk factors, it’s time to start the conversation about myopia management.3
Optical Biometry
It’s critical to be able to objectively measure optical biometry—specifically, axial length—to help you understand the progression of myopia in your patients.
The IOLMaster® delivers incredibly repeatable and accurate measurements. When I mention to parents that we can measure the length of the eye down to the 100th of a millimeter, they start to understand how serious we are about axial length, which is more closely correlated with ocular disease and vision loss than refractive error alone.
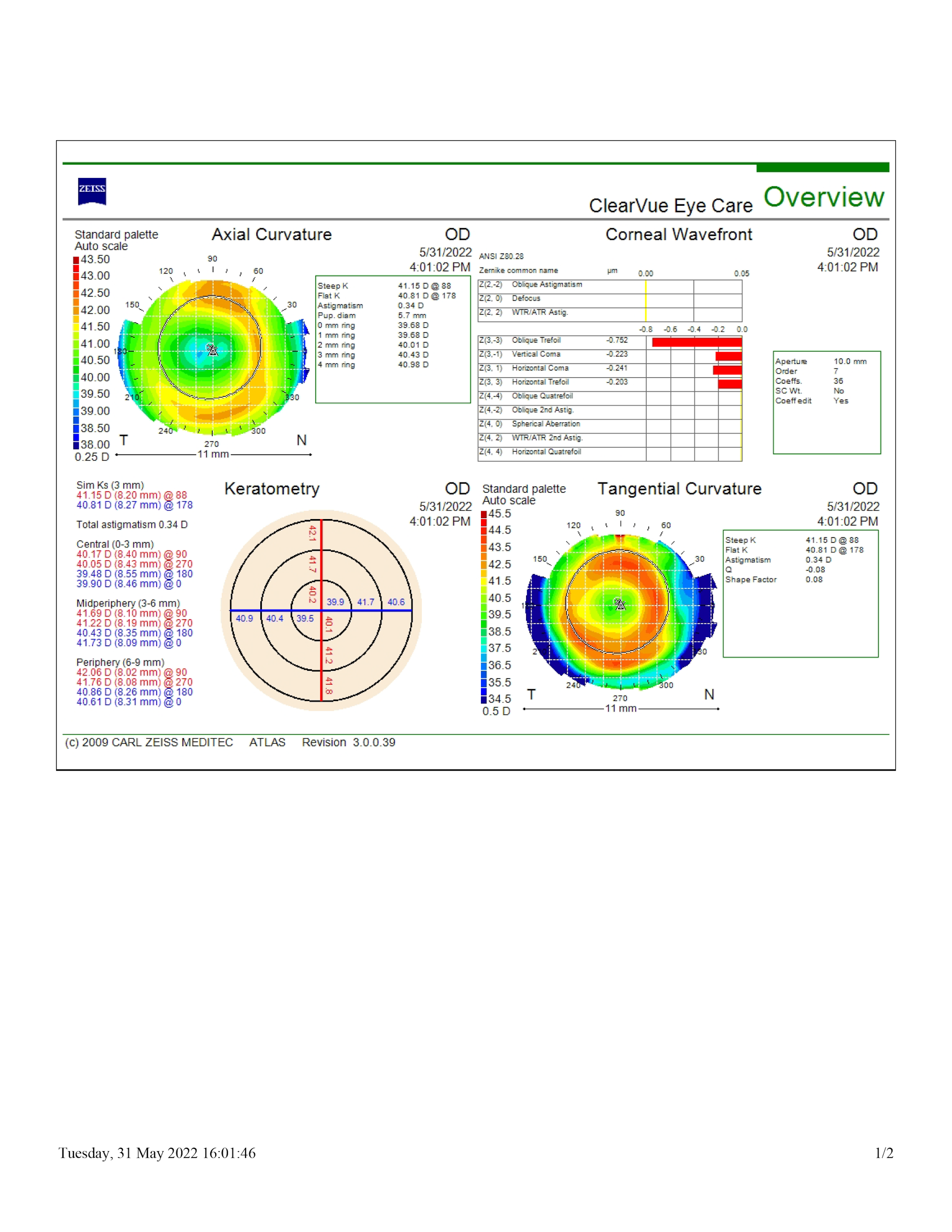
Corneal Topography
The next step is topography, which is critical information to have when fitting ortho-k lenses. Topography also provides objective data on scotopic and photopic pupil size. This is an incredibly important and useful tool when deciding which treatment option to use.
Corneal Wavefront Aberrometry
Something else that is nice, but not mandatory, is corneal wavefront aberrometry. Some higher-order aberrations are associated with myopia progression. So, if you have an instrument that provides that, you may start incorporating that into your treatment plan and use it to monitor progression.
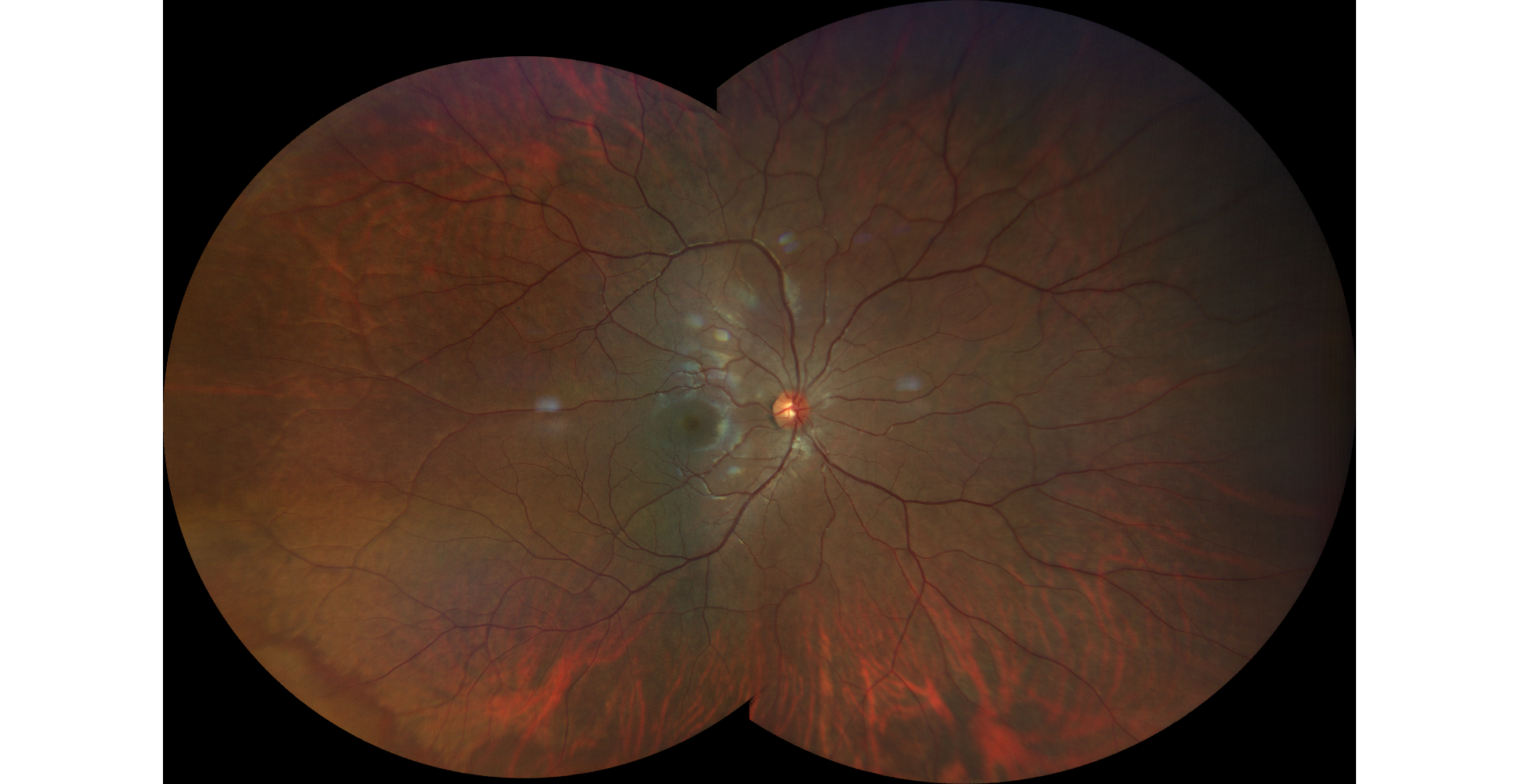
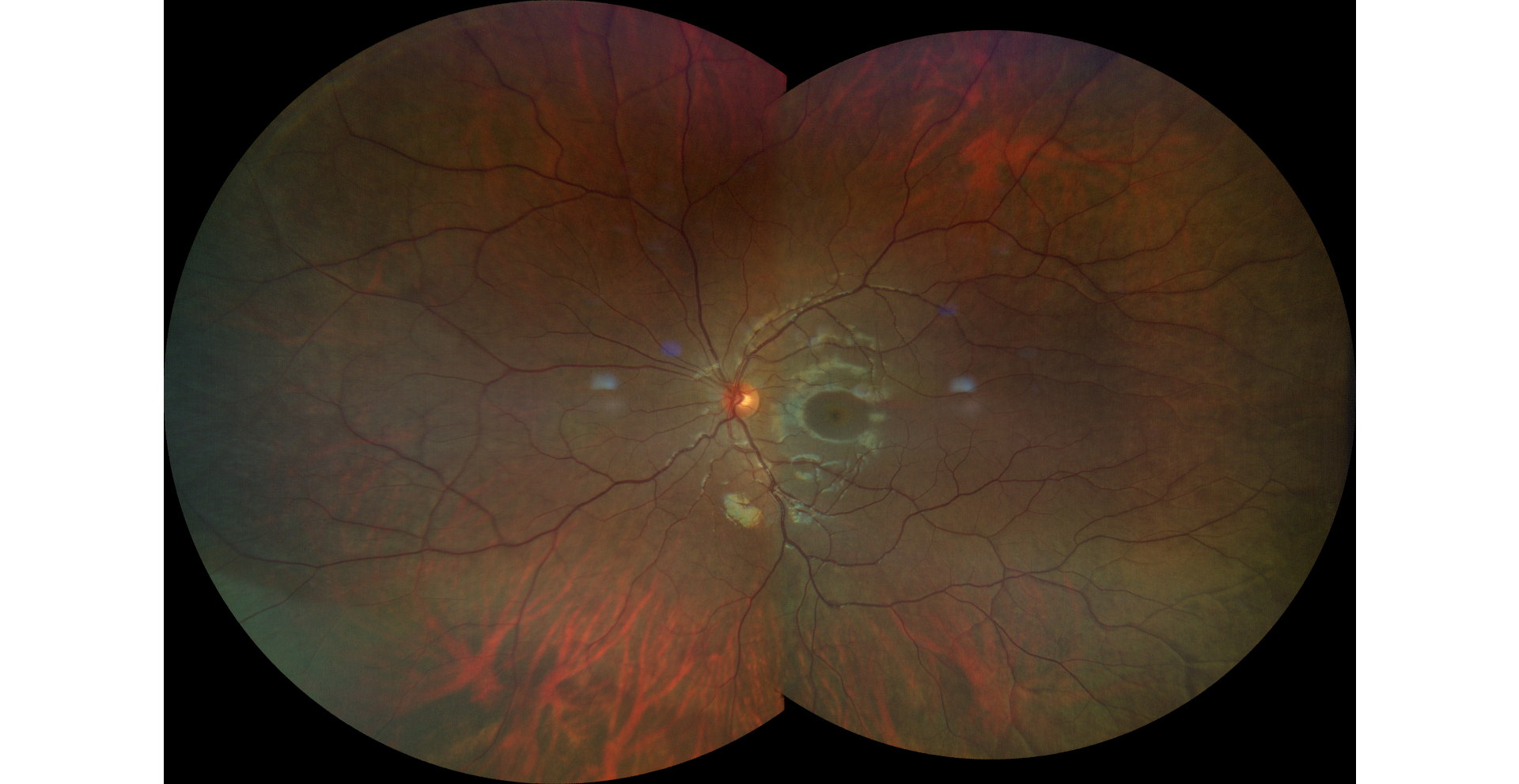
Fundus Imaging
Since we are advocating for the lifelong health of our patients' retinas, we need to monitor for the presence of disease. Access to an ultra-widefield fundus camera ensures nothing is missed. It’s an important tool and very easy to use.
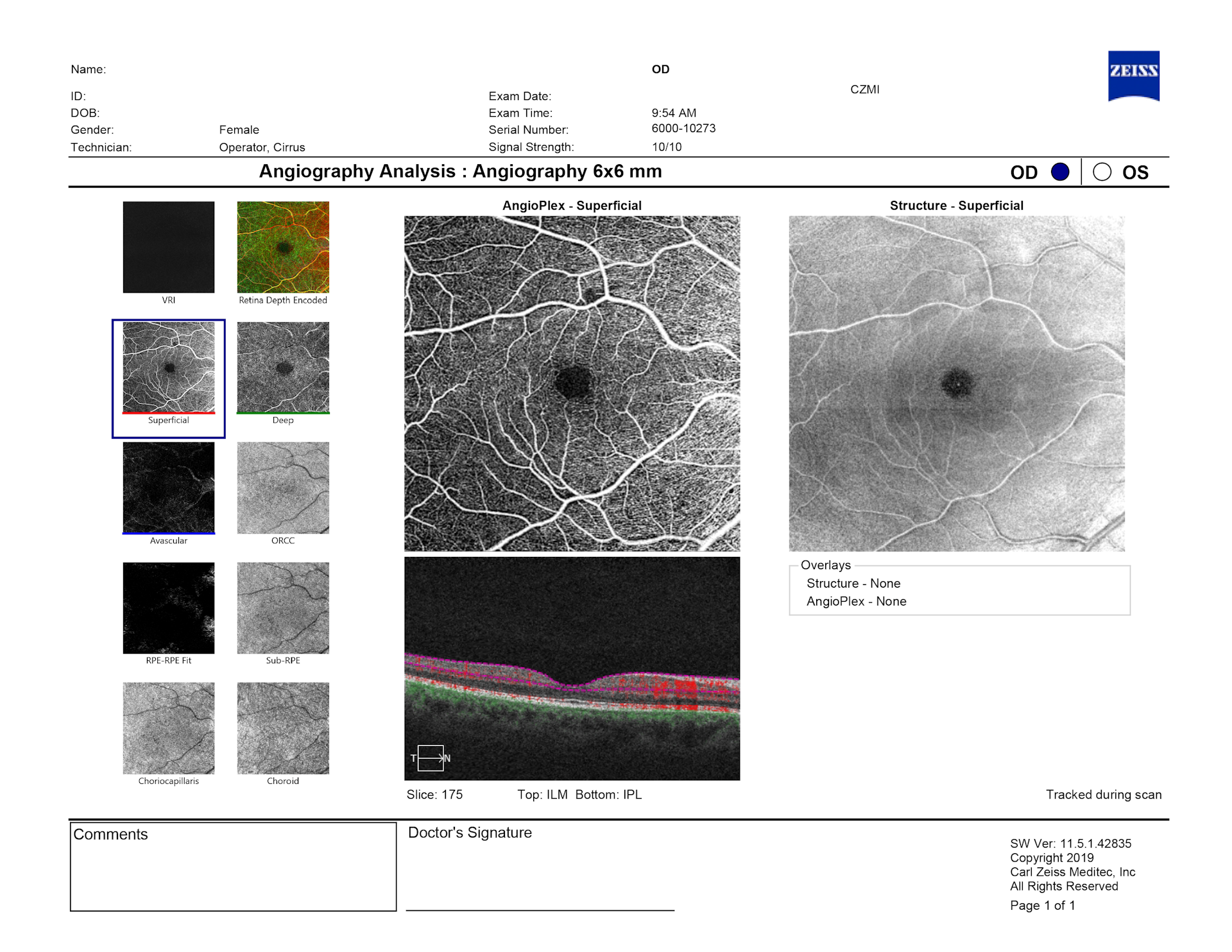
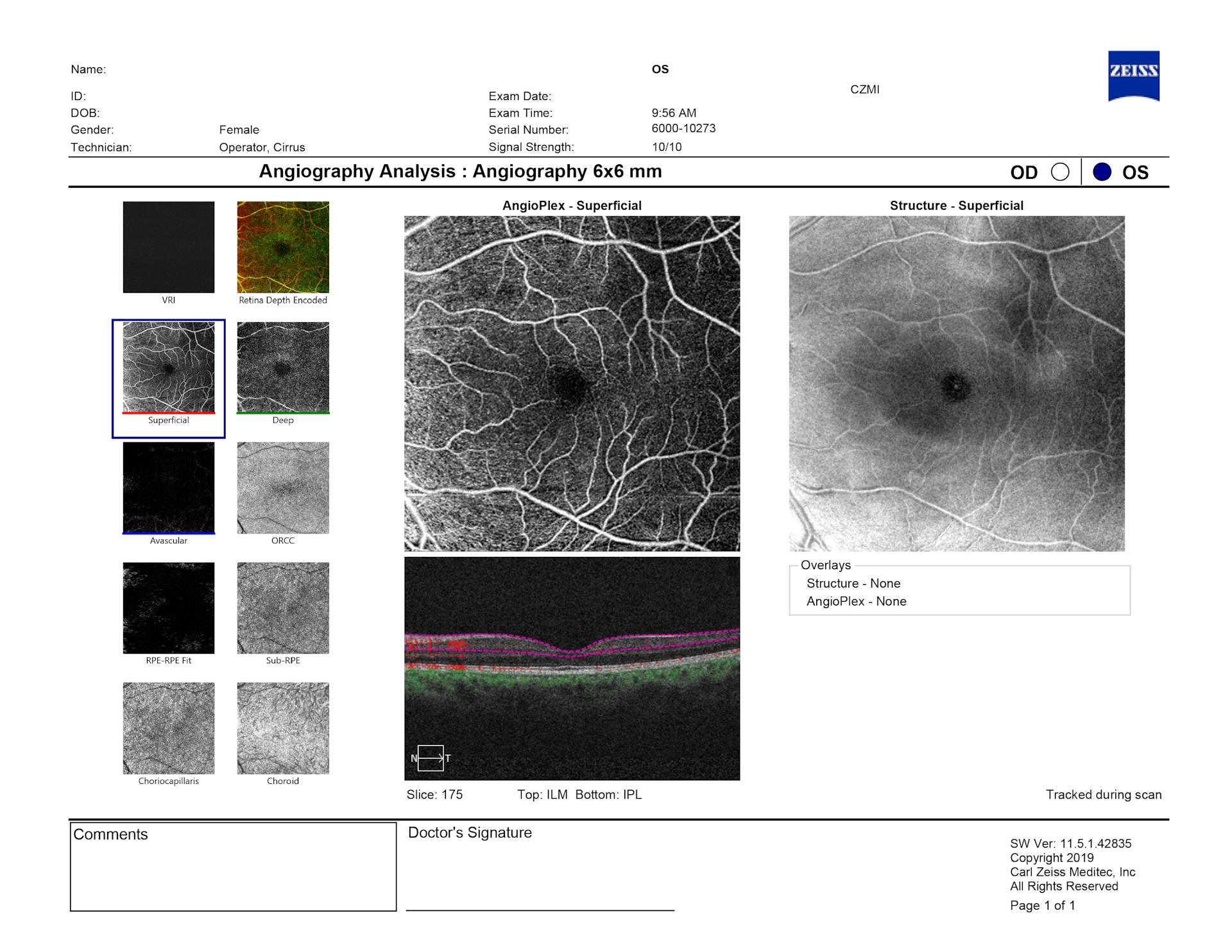
Optical Coherence Tomography (OCT)
Optical coherence tomography (OCT) and optical coherence tomography angiography (OCT-A) are invaluable when monitoring the health of the patient's macula, as well as retinal blood flow.
Treatment Options
The basic thinking regarding myopia management is called peripheral defocus theory—meaning that if we can bring the light falling on the peripheral retina to a focus in front of the retina, we can signal a slowing or even cessation of axial length growth.
Three optical strategies address this, as well as biochemical tools and recommendations related to environmental and behavioral factors.
Optical Strategies
- Ortho-k lenses that can be worn overnight.
- Soft multifocal contact lens worn during the day (we use center-distance designs).
- DIMS spectacle lenses. These specifically-designed spectacle lenses are not bifocals and not progressives. They’re called DIMS technology, which stands for Defocus Incorporated Multiple Segments. As we further understand how the mechanism of treatment works, we've been looking at exactly how much of the retina needs to be involved with this peripheral defocus. The newest thinking is looking at a dual-focus approach in which we’re taking a volume of space in front of the retina and focusing some light there—while also keeping a fair amount of light focused on the plane of the retina, obviously for clarity. Some of the spectacle lenses incorporate that type of strategy.4
Biochemical Strategies
From a biochemical approach, atropine eye drops have demonstrated the ability to slow myopia progression. While the exact mechanism of action isn’t known,5 atropine dilates the pupil and may relax the focusing mechanisms in the eye. Research suggests that myopia in children may be connected to focusing fatigue, so using atropine may help manage myopia by disabling the focusing mechanism.6 Atropine drops range in concentration from 0.01% to 0.05% dosed one drop into each eye at bedtime. It can be helpful to dose that way because it reduces side effects.
Environmental and Behavioral Strategies
Environmental adjustments can be prescribed as well. This means literally prescribing that a patient spend an average of two hours or more outdoors every day,7 weather permitting.
I also recommend that my patients make a reduction in screen time—which is a big ask, especially for older kids in school—but two hours or less is optimal.
Some current studies have indicated that increasing the working distance may be even more important and protective in myopia.8 A general rule to tell patients is that nothing should be closer than 16 inches from their faces. That includes books, papers, and handheld electronic devices. If they can be pushed out to 20 inches or so, even better.
Treatment Approach
Treatment approaches are based on a number of factors, including the patient’s:
- Age
- Current amount of refractive error
- Likely compliance
- Binocular status
- Pupil size
- Preference of the patient and parent
The higher the number of risk factors a patient has, the sooner treatment should begin, even if the patient is as young as five years old. If a patient already has refractive error, contact lenses are viable options, depending on their age. If they're really young, a single-use disposable contact lens is probably the easiest for them to use. As patients get older, it’s appropriate to incorporate ortho-k lenses.
Based on a patient’s binocularity, if they are esophoric—especially if they're esophoric at near—I prefer a multifocal contact lens. The same is true for patients who have an accommodative lag, because those patients are going to potentially benefit from that added plus in the bifocal at near.
If they are exophoric at near, it’s better to stay away from the add and consider working with atropine, unless a patient has a photopic pupil size of greater than 3mm, in which case those patients are more likely to experience photophobia when they go outside.
A workflow to manage myopia in your practice
Patient Workflow
After check-in, patients complete needed paperwork so we can obtain as much of the patient’s history as possible. They are then taken for a comprehensive exam in our diagnostic testing center, where we have a variety of instruments and technologies that provide excellent, repeatable, and accurate baseline data.
- We start with measuring axial length with the IOLMaster. This provides extremely accurate objective data on the length of the eye.
- Next, we obtain corneal topography. The topographer we use also provides baseline data on scotopic and photopic pupil size, as well as corneal wavefront aberrometry.

- After that, the patient moves to the OCT, which provides information regarding the health of the macula and the optic nerve—as well as ocular and retinal blood flow. We have OCT-A (optical coherence tomography angiography), as well.
- As part of advocating for lifelong health of the patient's eyes, an ultra-widefield (UWF) fundus imaging system is used for assessment, helping to ensure that we don't miss anything. I’ve found that with proper instruction, we can obtain very good images using this technology for patients as young as five years old.
Additional elements of the comprehensive exam include:
- Measuring objective and subject refraction
- Conducting a binocular evaluation screening
- Conducting a thorough eye health exam
If a patient has two or more risk factors, this is a good time to explain that myopia is actually a disease in which the retina is stretching and thinning, making it susceptible to holes and tears and ultimately disease. Patients may experience distance blur, but it’s important to emphasize that this is just one small symptom of a much bigger concern.
Patients will likely be curious about different treatment options, and it’s helpful to take advantage of this willingness to learn by providing any material you recommend so they can start to familiarize themselves with the different options that will be discussed at a later visit.
As the patient grows, the eye continues to stretch unless myopia management protocols are put into place. During scheduling, it’s critical to explain this to parents and ask them to procure all the previous eye exam records, in order to confirm age of onset and rate of progression up to this point.
Diagnostics and Imaging Prior to Initiating Therapy
- Axial Length
- Topography
- Photopic and Scotopic Pupil Size
- Ultra-Widefield Imaging
- OCT
- Subjective and Objective Refraction
- Binocular Vision Workup
- Ocular Health Assessment
Follow-up Schedule
In terms of follow up, the majority of my patients are seen at:
- 3 months
- 6 months
- 9 months
If a patient is started on atropine for the first time, a one-month follow up is also scheduled to check for photophobia outdoors or the need for a single-vision reader for small print up close.
In general, at the three-, six-, and nine-month checks, we double check refraction, talk about any side effects they might be having, and evaluate corneal integrity with a slit lamp.
Each year, at the comprehensive exam, I talk to the patient and parent about whether we need to continue working with the myopia management treatment, wean the treatment, or stop all together.
What we've learned from the COMET study is that by age 15, 50 percent of myopes are still progressing and won’t stabilize until about 24 years of age.9 The majority of my patients stay in treatment until around age 16.
Case studies
When I was still new to myopia management, I was concerned that prescribing multifocal soft contact lenses for my school-age kids might reduce their distance clarity. I was also concerned about reducing their contrast sensitivity, picturing these patients struggling to look at a whiteboard and take notes during class. However, the following case changed my perspective.
Myopia management case: I.S.
I.S. is a 12-year-old female of Indian descent. She was referred because her parents are both highly myopic and she's already in the danger zone.
- 12-year-old female of Indian descent
- Referred due to risk factors and concerning assessment data
- RE: OD -6.50 -0.50 x 100
OS -6.25 -0.50 x 067
- Axial Length (AL) at eval: OD 26.31mm OS 26.33mm
- Risk factors: Two highly-myopic parents
- One diopter increase in myopia previous year, esophoric at near
The patient and parents were eager to move forward and I chose to fit her with a multifocal soft contact lens. She came in wearing really thick glasses, heavy on her nose, and I wanted to relieve the weight for her by putting her into contact lenses. I chose the NaturalVue® multifocal contact lens and put her in powers of right eye -6.25 and left eye -6.00.
TX: Daily disposable multifocal soft contact lens with center distance design and +2.50 add
Contact Lens (CL) Rx: OD: -6.25DS OS: -6.00DS
Three-month follow-up
At her first follow-up, she mentioned that she was having some trouble with her distance vision. She was seeing about 20/40 and her spherical over-refraction was about -0.75 on each eye.
VA c CL: 20/40 in each eye with Subjective Over Refraction: -0.75DS OU
So I decided to incorporate that over-refraction into her contact lens powers and see what happens. I put her right eye in a -7.00DS and I put her left eye in a -6.75DS with this power change.
TX update: New contact lenses dispensed: OD -7.00DS 20/20 OS -6.75DS 20/20
With the change, her distance visual acuity improved to 20/20 on each eye. She was super happy with her vision and actually felt she was seeing better in the contact lenses than she was in the glasses.
Six-month follow-up
At her six-month follow-up, her axial length had changed by less than 0.05mm. She had ongoing clarity at a distance, allowing her to comfortably see the board at school. Everyone was very happy.
Axial Length: OD: 26.38mm
OS: 26.37mm
- A change in axial length of less than 0.05mm in each eye
- Ongoing clarity at a distance, allowing her to comfortably see the board at school
Since then, I have not hesitated to add between -0.50 and -0.75 to the distance prescription in multifocal contact lenses to help ensure patients have good distance clarity. In doing so, I can go ahead and use the +2.50 add to get maximum amount of peripheral defocus for myopia progression. That has worked extremely well with excellent results in my clinic.
Myopia management case: C.G.
C.G. is a nine-year-old Caucasian female who loves to read for hours at a time and has one myopic parent. Her initial evaluation revealed a refractive error of her right eye being -3.75 with 2.5 diopters of cylinder and her left eye being -3.5 with 1 diopter of cylinder.
- C.G. 9-year-old female Caucasian
- RE: OD -3.75 -2.50 x 011
OS -3.50 -1.00 x 166
- AL at evaluation: OD 25.65mm OS 25.53mm
- Binocular posture: 8 exophoria at near, monocular accommodative amplitudes of 12D in each eye
C.G.’s refractive error would normally equate to an axial length of about 24mm, maybe 24.5mm. In this case, her axial length had progressed even further than that, at lengths of 25.65mm and 25.53mm, respectively. So, it's worth remembering that lower myopia doesn't always equate with shorter axial length.
That was my first concern. She was getting really close to that 26mm cutoff, so I wanted to slow the progression right away.
Also worth noting, she was exophoric at near, and her photopic pupils were about 2mm to 2.5 mm, so we were good there. I also decided to verify her monocular amplitudes of accommodation to make sure she had excellent reserves, which she did. She had about 12 diopters on each eye.
I prescribed the 0.05% of atropine because I wanted to slow things down immediately.
TX: Atropine drops (gtts), 0.05% instilled one drop into each eye at bedtime nightly.
Six-month follow-up
At her six-month follow up, her axial lengths had changed by 0.17mm on her right eye and 0.12mm on her left eye. She reported no photophobia and no difficulty reading small print.
Axial Length: OD: 25.82 (change of 0.17mm)
OS: 25.62 (change of 0.12mm)
I was mildly concerned as that was slightly more than I wanted to see at six months, but I decided to keep her on the atropine and measure her again in a year, then 18 months, and so on.
Two-year follow-up
If you fast forward two years, she’s now age 11, and her axial length over that last year only changed 0.05mm over 12 months and her left eye didn't change at all over 12 months. Her refraction over those last two years was only increased by -0.5 diopters of myopia on the right eye and -0.25 diopters in the left eye. There was no change in cylinder in either eye, as you would expect.
Axial length:
OD: 25.87mm (change of 0.05mm over 18 months)
OS: 25.65mm (no change over 18 months)
Refraction:
OD: -4.25 -2.50 x 011 (0.50D increase)
OS: -3.75 -1.00 x 166 (0.25D increase)
She's never had any side effects from the atropine and we were able to locate a compounding pharmacy in our area that's willing to auto-renew for the patients each month. They mail the drops to them, delivering them to their doorstep on ice. The parents really appreciate that convenience.
When you integrate myopia management into your practice, the professional fulfillment and gratitude from families is something to absolutely look forward to, and I encourage you to start today.
