


Optometrists across the continent have been seeing rapid myopic progression in children and young adults since the onset of the COVID-19 pandemic. Stay-at-home restrictions led to increased online activity, less social interaction with peers, and more hours spent indoors on hobbies that require close working distances.
Previous research has confirmed that risk factors for myopia include longer near-viewing time and less outdoor time; therefore, stay-at-home restrictions became a triggering factor for near point visual stress.1,2
Additionally, the modern-day classroom or learning environment relies heavily on devices where children sit at their desks for longer periods of time to complete assignments and homework. The increased effort it takes to read and learn at a closer working distance puts children at a higher risk for near point stress, accommodative or binocular vision issues, and, ultimately, myopic progression.
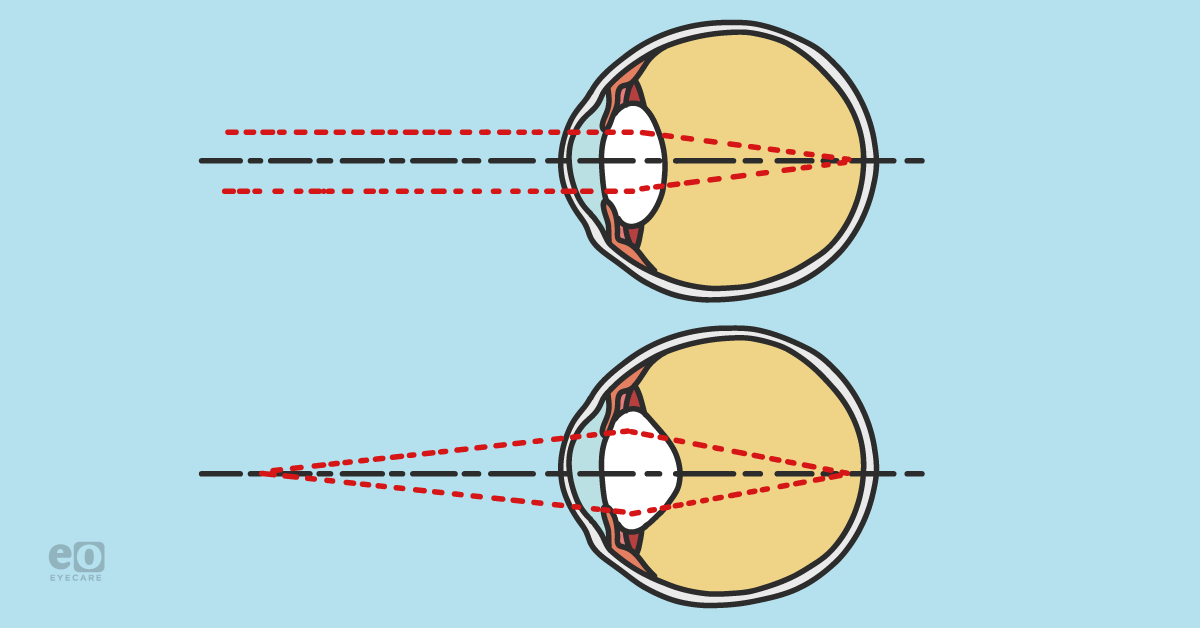
Near point stress is one theory as to why myopia occurs and progresses.
The near point stress model explained
The near point stress model emphasizes how the visual system likely adapts to near point stress by increasing the eye’s axial length, thereby adjusting where the near image falls on the retina to compensate for this constant tug-of-war battle between our accommodation and convergence systems.3-7
Figure 1 breaks down the near point stress model and explains the near point stress theory.

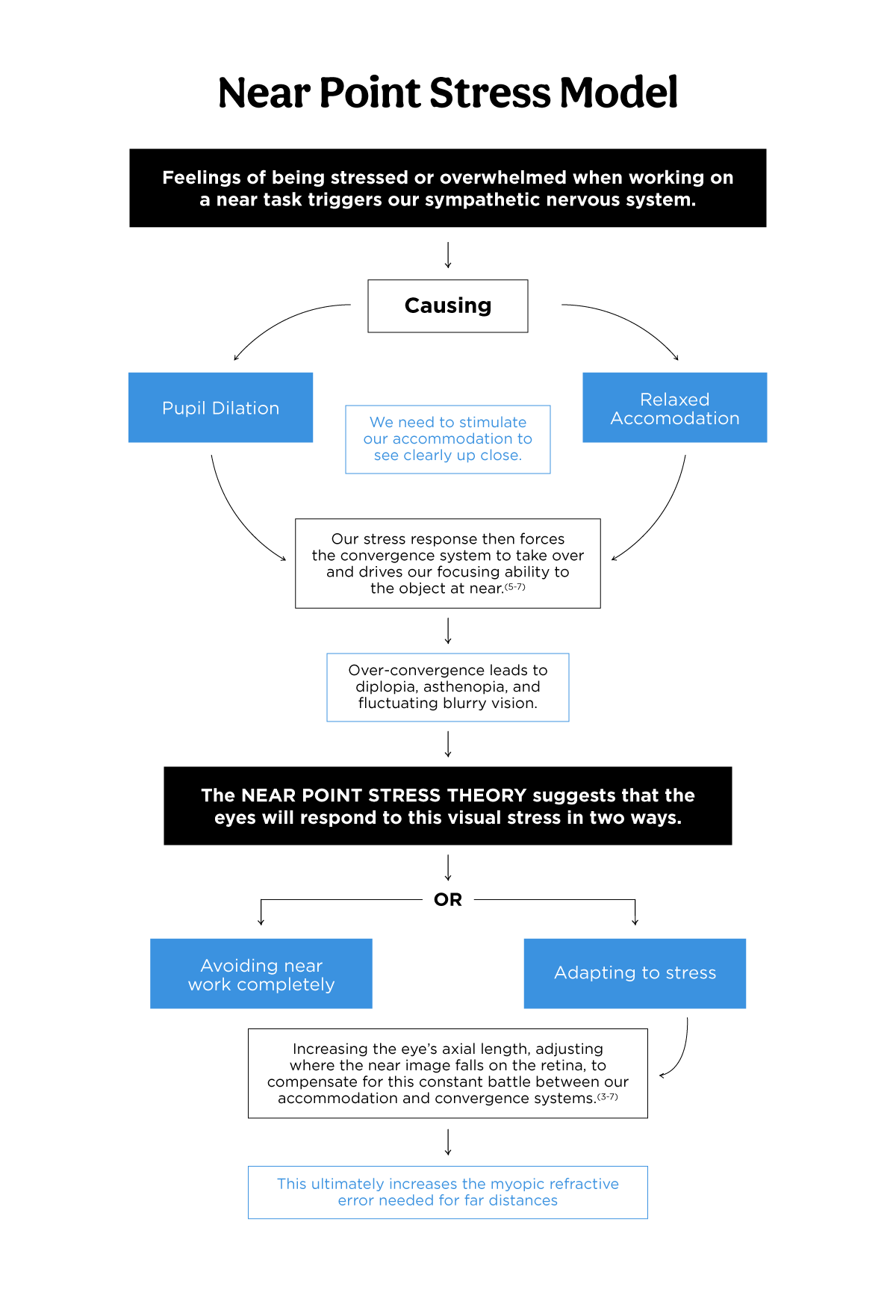
Figure 1
Myopia is not just an inconvenience for the patient to wear glasses full-time. Children with significant myopic progression are at a higher risk of developing sight-threatening conditions such as retinal detachments, macular degeneration, and glaucoma.8
Improving patient outcomes with prevention
Therefore, it is crucial for optometrists to identify risk factors and begin early intervention to slow down myopia progression. There are other theories that have been proposed regarding myopia development, such as peripheral hyperopic defocus, but this runs a bit contrary to what we know about near point stress.
This latter theory suggests certain clinical signs during an eye exam might be the sparks that light the fire of increased risk of myopia onset or progression in young children. These clinical findings can become leading points in discussions with parents on starting their child’s myopia control early by targeting their accommodation and binocular status and encouraging healthy visual behaviors moving forward.
Identifying binocular vision concerns during an eye exam
1) Observe visual behaviors during the exam
When measuring near visual acuities, hand the near card to the child without giving any prompts on where to hold it. Keep an eye on the child’s working distance as they read.
If they begin to furrow their brows or bring the card closer as the lines become smaller, you can suspect that the child feels stressed or overwhelmed when reading and prefers a closer working distance at school or home. You can also assume this if the child prefers to lean towards the test booklet during stereopsis or color vision testing.
2) Watching out for fluctuating blurry vision at near
Children can often see better when focusing on objects up close compared to far distances due to their strong accommodative system, even without correcting the refractive error.
If a child is struggling to see 20/25 or better on the near card at an appropriate working distance, it is safe to assume their vision is fluctuating at near. This highly suggests a disrupted accommodative-convergence system that needs to be addressed.
3) Uncovering orthophoria or esophoria on a near cover test
A natural human eye posture at near should be slightly relaxed into a low exophoria, between 2 to 4 prism diopters. This posture is considered a “natural buffer” that gradually evolved to reduce the impact of near visual stress.9
When the eyes are under accommodative stress, the convergence system will over-stimulate, leading to an orthophoria or esophoric posture at near. This ocular posture suggests an imbalance in the accommodative-convergence system and that the child is developing a closer working distance due to visual stress.
4) How to interpret monocular estimated method (MEM) and fused cross-cylinder (FCC)
Determining the accommodative posture after measuring the subjective refraction will provide further information as to whether the child has an over-focused or weak accommodative system.
Typically, a low MEM or a lead (+0.25D or lower) suggests accommodative excess or spasm, meaning the eyes are over-focused at near. This result typically falls in line with the patients having a close working distance and an orthophoria or esophoric posture.
5) Unbalanced NRA/PRA or poor flipper flexibility
Measure the flexibility of the child’s accommodative system through the subjective refraction with NRA/PRA (negative relative accommodation/positive relative accommodation) or with +/-2.00D flippers.
Viewing through minus lenses drives convergence and stimulates accommodation; therefore, a low PRA result (< -1.75D) or difficulty clearing the -2.00D lens can be a warning sign of a poor convergence-accommodative system.
Take note of all these clinical signs during the eye exam, and use these results to initiate myopia control treatment options that target near point stress.
Visual behaviors to address near point stress management and myopic progression
Children may benefit from wearing a low plus-powered lens for near tasks to relieve visual stress, treat accommodative dysfunction, and slow myopic progression. Certain factors should be considered when determining an add power, such as the NRA/PRA balance, the FCC/MEM result, changes to the phoria posture, and the child’s behavioral response or working distance through a trial frame.
A vision therapy program is an excellent recommendation to target accommodative and binocular dysfunction with or without the use of passive lenses. Vision therapy provides a long-term resolution to near point stress symptoms, strengthens the accommodative-convergence system, and enables the child to develop healthier visual behaviors to slow myopic progression.
Lastly, provide a list of healthy visual behaviors for the child to practice on a daily basis to reduce their visual stress load. Common examples of visual behaviors I discuss in my exam room include the following:
Take visual breaks from near tasks and screen time to prevent accommodative stress and fatigue
The length of the break and recommended recreational screen time can vary depending on the child’s age.
I follow the guidelines recommended by the Canadian Association of Optometrists (CAO), which aligns with both the American Academy of Pediatrics (AAP) and the World Health Organization (WHO):
- Age 0 to 2: minimal to no screen time besides video-calling family members.
- Age 2 to 5: up to 1 hour of screen time or reading/writing activity per day.
- Age 5 to 18: up to 2 hours of screen time or reading/writing activity per day.
Additional breaks are recommended for school-aged children who participate in online learning or use electronic devices during school hours. Children should look far away from their devices for a few short minutes every 30 minutes or so during school hours. The 20-20-20 rule can be applied to teenagers and young adults, but I still encourage longer visual break times throughout the day.
Extend the working distance with all near tasks
An extended working distance prevents over-convergence and requires less accommodative power than closer working distances. Recommend patients to hold devices and books farther from the child’s face. I demonstrate this in the exam room with the child to show them how books and tablets should be held in their lap, not floating in the air.
Sit comfortably and far away from electronic devices placed on a desk. Try switching from smaller handheld devices like phones or tablets to large television screens mounted on the wall when watching videos. Enlarge the font sizes on electronic devices to make it easier for children to sit farther away from the device.
Incorporate physical activity
Physical activity can help reduce the accommodative and emotional stress that triggers myopic progression. It also encourages the child to take more break times from near work. Encourage children to join extra-curricular activities to increase physical activity and social interaction with peers.
Enroll them in sports programs all year round, which provide an additional bonus of encouraging better visual tracking, depth perception, and hand-eye coordination skills to improve overall visual performance.
Regulate internal stress levels
Internal stress levels can influence our accommodative response to completing near tasks. Recommend ways to decrease internal stress levels by getting adequate sleep, eating a healthy diet, regular physical exercise, and spending time on hobbies the child may enjoy outside school.
Conclusion
Taking the time to evaluate these risk factors and educating patients on healthy visual behaviors can help steer the binocular and accommodative system back into a healthy balance and, in turn, potentially slow down myopia progression.
