



From November 18 to 20, 2022, eyecare practitioners from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from I. Paul Singh, MD, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
With the recent proliferation of safe and effective treatments for glaucoma, there has been a corresponding paradigm shift to a more interventional mindset and model. Minimally-invasive glaucoma surgery (MIGS) has sparked this expansion in technology, as it allows for eyecare practitioners (ECPs) to tailor the glaucoma treatment model to individual patient needs, better understand the mechanisms of resistance, develop new diagnostics, and focus on patient quality-of-life and earlier intervention.
The glaucoma treatment toolbox is expanding not only with MIGS but also with new molecules that target the outflow pathway, such as Netarsudil ophthalmic solution 0.02%. These products, along with MIGS, allow ophthalmologists to improve the outflow facility and more directly address the pathology in a safe way to prevent further progression.

Watch the full lecture on MIGS procedures!
Sign up for our newsletter to watch the full recording from Eyes On 2023.

Non-compliance in glaucoma treatments
It is widely known that compliance is poor for glaucoma treatment, the main reasons are cost, physical difficulties, side effects, forgetfulness, and the dosing regimen. This poor compliance spurs the development of new technologies as researchers and ECPs work together to improve glaucoma patient outcomes.
Glaucoma and dry eye disease
It is particularly difficult to treat glaucoma patients with concomitant dry eye disease (DED). In fact, DED is a common reason for discontinuation or inadequate compliance with glaucoma treatment. A study of 74 patients with glaucoma showed that DED symptoms were predictors of noncompliance. The compliance rate of glaucoma medications was 89% for patients without DED symptoms and 63% for patients with DED symptoms.
Also, the study showed that exposure to benzalkonium chloride (BAK), a preservative used in ophthalmic solutions, is a risk factor for earlier surgical failure. BAK can cause fibrosis of the trabecular meshwork (TM) and fibrosis and scarring of the episcleral venous system and associated collector channels. Scarring of the goblet cells in the conjunctiva can cause additional inflammation on the ocular surface that further impacts DED patients.
Tips for identifying glaucoma patients with DED:
- Take an accurate patient history and ask about symptoms related to an unstable tear film.
- Use a yellow Wratten filter and a cobalt blue light simultaneously to highlight the epithelial basement membrane dystrophy (EBMD) and look for instability in the tear film break-up time.
Figure 1 shows a table comparing the incidence of DED in glaucoma patients to the number of drops that patients were on.

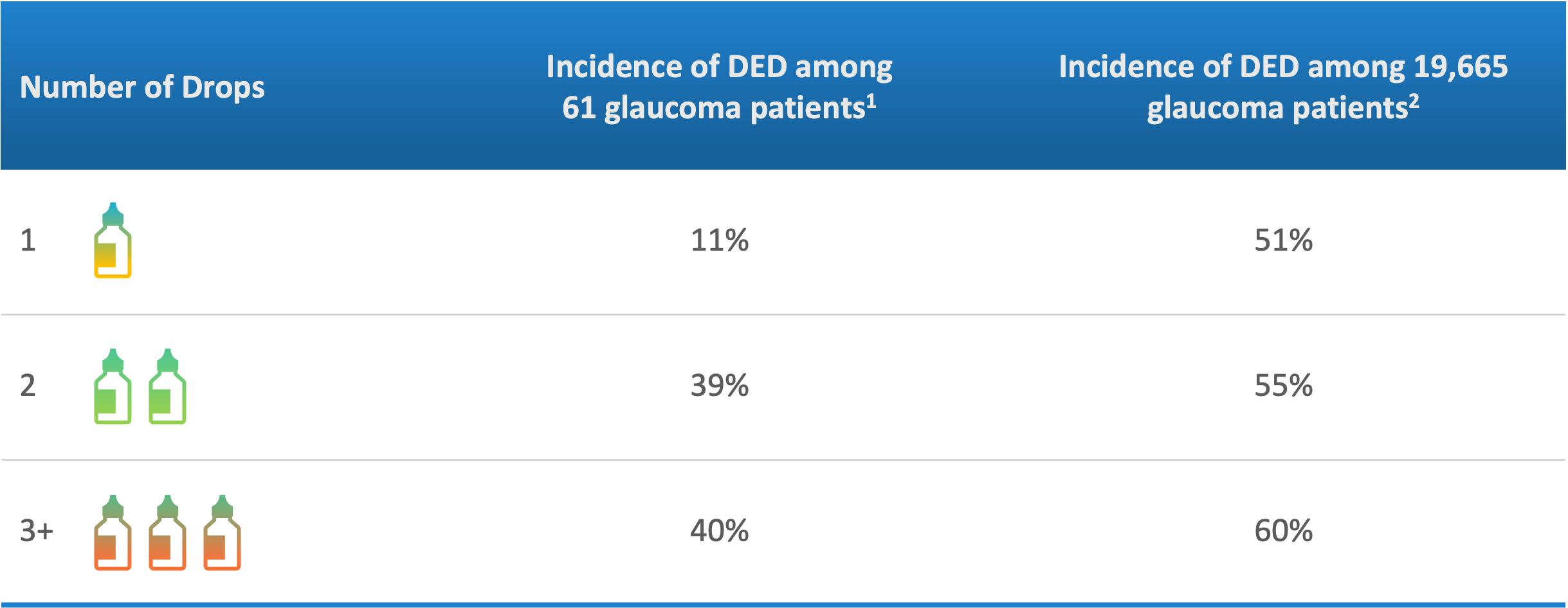
Figure 1: Image courtesy of I. Paul Singh, MD.
Redefining controlled glaucoma
Current metrics for well-controlled glaucoma include lowered intraocular pressure (IOP), acceptable visual field, and stabilization of the optic nerve. By adding patient quality of life to this list of metrics, ECPs can factor in the likelihood that a patient will stay on a specific regimen long-term.
This requires paying attention to clues for noncompliant behavior, as noncompliance causes an increase in IOP fluctuation for patients with glaucoma. The Advanced Glaucoma Intervention Study found that higher amounts of long-term IOP fluctuation are associated with visual field progression.
While putting a patient on a long-term dosing regimen is likely to result in noncompliance, the LiGHT trial showed that first-line selective laser trabeculoplasty (SLT) treatment has the same efficacy as eye drops. On top of that, 74.2% of SLT patients reached the target IOP and were drop-free at 36 months. Patients who received SLT were five times less likely to have medication-drop-related adverse events. All in all, SLTs provide ECPs with even more options for treating glaucoma.
MIGS and interventional glaucoma management
The hallmarks of MIGS are safety, less trauma to the target tissues with an ab interno or microincisional approach, high intraoperative safety, and rapid recovery with minimal impact on the patient’s quality of life. Combined, MIGS helps keep options open for patients requiring future procedures.
A MarketScope study in 2021 found that 40% of comprehensive cataract surgeons do not offer MIGS, so it’s clear that a disconnect remains between ophthalmologists and the large-scale adoption of MIGS procedures into glaucoma treatment management. This could potentially be because surgeons are struggling with getting reimbursements for procedures and because, overall, there is a lower confidence level that MIGS will provide the same results as drops.
Conventional pathway MIGS
Regardless of the device, conventional alpha pathway MIGS have all been shown to produce results that get you to the middle teens for IOP. The best way to approach these procedures is to ask yourself which option is best for the patient’s anatomy based on your expertise as a surgeon.
It is vital to manage patient expectations by communicating what you define successful treatment to be. This could include reducing IOP, reducing the patient’s medication burden, and reducing future chair time at the ophthalmologist’s office.
Breakdown of conventional outflow MIGS:
- Outflow stents: Approved at the time of cataract surgery
- iStent Inject
- Hydrus
- Dilation of the outflow system: Approved both with cataract surgery and as a stand-alone
- Streamline
- Omni iTrack iPrime
- Trabecular meshwork stripping and/or removal: Approved both with cataract surgery and as a stand-alone
- Kahook dual blade (KDB)
- Gonioscopy-assisted transluminal trabeculotomy procedure/Omni system
Surgical pearls for MIGS
1. Establishing an en face view
Getting a clear en face view during the MIGS procedure is vital for improving patient outcomes. To do this requires not only understanding the patient’s anatomy but also understanding how to get the trabecular network to face you during the procedure. The more en face you are, the easier it is to complete MIGS procedures and produce consistent results. Fortunately, the skill sets needed for the various MIGS devices are very similar.
2. Using a 6-0 silk suture
Another pearl for surgeons is to use a 6-0 silk suture to place episcleral bites to the episclera. The 6-0 silk sutures are clamped to the drape and provide perfect counter-traction for the procedure. This way, during the procedure, there is no torsion or torquing of the eye.
Figure 2 is a still taken from a surgical video where the 6-0 silk sutures are placed in the episclera to prevent traction during the MIGS procedure.

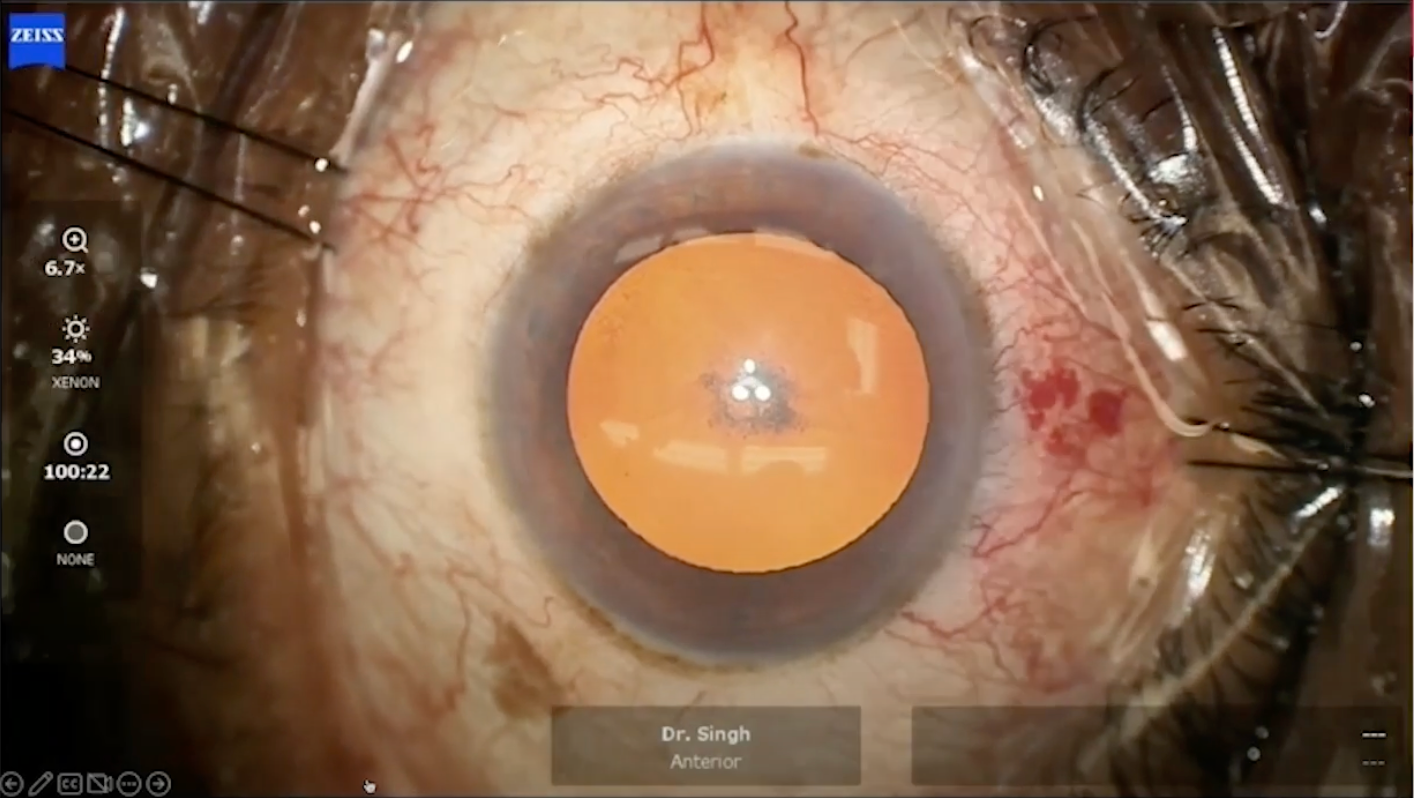
Figure 2: Image courtesy of I. Paul Singh, MD.
3. Understanding unique outflow pathway morphologies
Not every MIGS procedure will work on every patient, the success of the treatment depends on where the resistance to outflow is and the mechanism of action. Surgeons can expect to see patients with varying thicknesses of the outflow pathways, different locations of the collector channels, and an uneven distribution of these collector channels. Often, collector channels are concentrated in the nasal quadrants, so if you can access two or three of those nasal quadrant channels, there’s a good chance that you’ll have significant efficacy.
Figure 3 features a 360-degree reconstruction of live human outflow pathways.

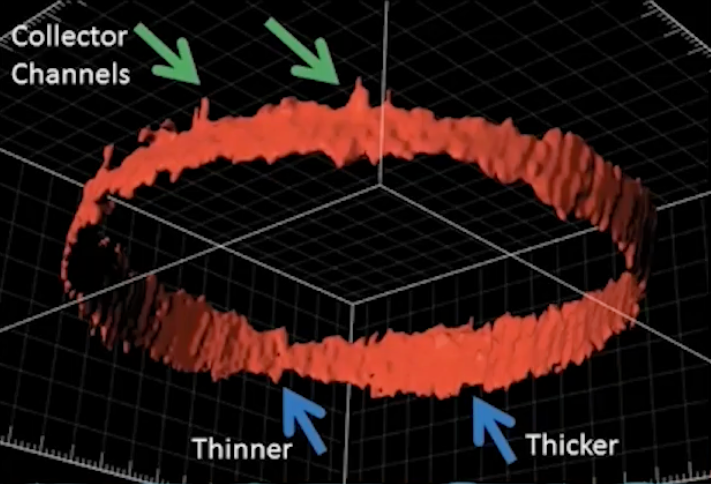
Figure 3: Image courtesy of I. Paul Singh, MD.
MIGS: outflow stents
The iStent inject
In a paper by the author about data from the phase 3 trial for the iStent inject, it was found that the iStent inject effectively reduced IOP across different ranges of baseline IOP. The study also showed that a greater reduction was recorded in eyes with higher baseline IOP. Recently the FDA approved the iStent Infinite for a refractory population of patients, which will help these patients avoid requiring a second trabeculectomy or tube.
The Hydrus
Data from the 5-year results of the HORIZON trial showed that patients who received a Hydrus procedure had a 61% reduction in risk of secondary surgical interventions and ⅔ of the patients who had an invasive glaucoma surgery were mild at baseline.
It’s important to remember that with glaucoma, mild symptoms do not always equate to conservative management, as even mild cases can have rapid progression and visual field decrease.
MIGS: canaloplasty and goniotomy
This resurgence in the development of glaucoma treatments has led to technological innovations in the field, such as the iTrack catheter, OMNI surgical system, iPrime, Streamline, and the Kahook dual blade that help with viscodilation to perform canaloplasties and goniotomies.
Currently used MIGS devices:
- iTrack catheter: A viscodelivery device that helps to break the herniations within the canal and viscal channels and gives control to the surgeon to release as much viscoelasticity in the canal as desired.
- The iTrack Advanced is approved in Europe and offers a new loading mechanism to the iTrack system, allowing for increased efficiency and comfort during surgery.
- OMNI surgical system: A catheter device that automatically releases viscoelastic into the canal as you retract it, which the iTrack can not do.
- iPrime viscodelivery system: Designed to deliver consistent and controlled amounts of viscoelastic during ophthalmic surgery.
- It allows surgeons to administer up to 2.7μl of viscoelastic with each forward activation of the dispense trigger button, independent of microcatheter movement.
- Streamline device: Releases 7μl of viscoelastic with significant force to create a microgoniotomy.
- KDB incisional goniotomy: The KDB works well for pseudophakic patients after a laser peripheral iridotomy, patients with unique anatomies, and patients with TM-based diseases.
- Sight Sciences recently released Sion, a similar device that creates an incisional goniotomy.
New MIGS devices:
- Excimer laser trabeculostomy (ELT): Performed in combination with cataract surgery, ELT creates 10 microchannels in the TM, each with 210μm, which creates an overall 2100μm of new outflow.
- ELT uses a photo ablative decomposition process to disrupt chemical bonds in the TM without causing any thermal damage to surrounding tissue. This allows aqueous to flow through microchannels into the Schlemms canal, lowering IOP and preserving the TM integrity, structure, and function.
- iAccess trabecular trephine: Created by Glaukos, it has a microgoniotomy 30-gauge, precision-lathed titanium nitride tip that creates ~220μm diameter outflow channels.
- There is a 300μm deep built-in safety backstop and an ergonomic, custom-tapered handle designed for comfort and control. During surgery, you can augment your stenting or viscodillation with a few of these micro-otomies to access more collector channels.
Combining MIGS procedures
With these innovations, there is the opportunity to mix different MIGS technologies, such as procedures that dilate, remove/cut TM, and stent and procedures with canal dilation and stenting. Combining these technologies allows surgeons to decrease inflow and increase outflow with other canal-based surgeries.
Overall, using MIGS, you can bring down IOP to the mid-teens and see a reduction in the long-term medication burden to glaucoma patients. Meaning that patients on multiple glaucoma medications would likely have great success with a MIGS.
Figure 4 is a procedure algorithm to use when deciding which MIGS procedure is the best fit for a patient.

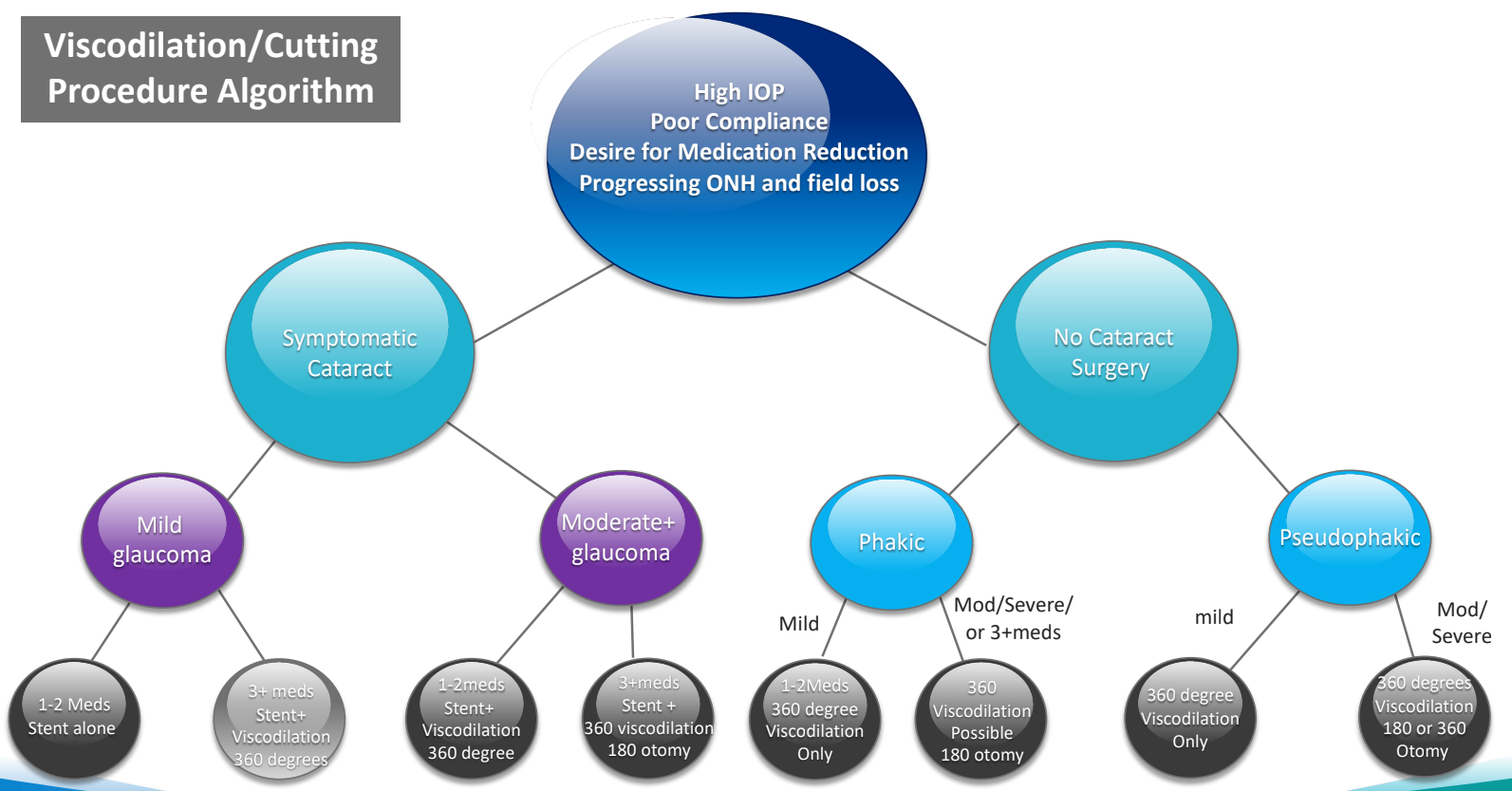
Figure 4: Image courtesy of I. Paul Singh, MD.
MIGS postoperative management
Postoperative management for MIGS procedures is similar to cataract surgery, but ophthalmologists should watch for steroid spikes around 2 to 3 weeks after treatment. If a patient presents with postoperative hyphema, consider reducing activities that increase episcleral venous pressure. Additionally, if a patient is on multiple drops, consider keeping them on aqueous suppressants for the first few weeks after the procedure.
Conclusion
As an eyecare practitioner, reducing a patient’s medication load, even by one medication, provides significant value and is immensely helpful to patients. MIGS technologies allow for earlier intervention, which increases the chance we have of achieving the target IOP. As a cherry on top, conventional MIGS procedures allow for predictable postoperative follow-up, which, in turn, helps with minimizing poor compliance.
By offering more safe and accessible treatments to patients, noncompliance-based glaucoma progression can be nipped in the bud. At the end of the day, the take-home for treating glaucoma patients with MIGS is to always listen to the patient. They give us clues along the way for identifying the best approach to treatment.
