



Micro-invasive Glaucoma Surgery (MIGS) was first introduced in 2004 with the approval of Trabectome, but then exploded onto the scene in 2012 with the approval of the iStent (Glaukos, Laguna Hills, CA) and turned the glaucoma world on its head. Since then many new procedures and devices have emerged, each of which provides different risk, benefit, and safety profiles. One of those devices is the Kahook Dual Blade (KDB, New World Medical, Rancho Cucamonga, CA) which was introduced in the United States in 2015 (Figure 1).


Figure 1: The Kahook Dual Blade
Goniotomy with the KDB works by removing the trabecular meshwork (TM) in a minimally invasive manner. Remember that in glaucoma, the TM, specifically the juxtacanalicular TM, is the site of greatest resistance to aqueous outflow. Therefore, removing it should in turn lower intraocular pressure (IOP) by improving aqueous outflow.
KDB clinical outcomes
KDB goniotomy has gained acceptance since its introduction due to its favorable safety profile and excellent clinical results. Unfortunately, given its relative novelty, many studies have limited follow-up to only about one year. In a one-year study by Sieck et al of 197 eyes, success rate (defined as IOP reduction >20% or reduction of at least one medication) was approximately 72% with combination phacoemulsification and KDB goniotomy (phaco+KDB) and 69% with KDB goniotomy as a standalone procedure. In that same study, average IOP in the phaco+KDB group was significantly reduced from16.7mmHg on 1.9 meds pre-operatively (pre-op) down to 13.8mmHg on 1.5 medications post-operatively (post-op). With standalone KDB, the IOP was reduced from 20.4mmHg on 3.1 medications pre-op to 14.1mmHg on 2.3 medications post-op (1). Sieck et al then presented their two-year results on 382 eyes (74 KDB only eyes, 308 phaco+KDB eyes). Average IOP at 2 years was 13.5 mmHg, down from 16.3mmHg for phaco+KDB and 14.5mmHg, down from 21.8mmHg pre-op for KDB only. They also evaluated success rates in different glaucoma subtypes. Pseudoexfoliation glaucoma patients had the highest success rate at 86.1% followed by primary open angle glaucoma at 65.8% (2).
Comparison to other MIGS and goniotomy techniques
Again, because of their relative novelty, there have not been many studies which directly compare different MIGS procedures to one another. This can sometimes make deciding between procedures more difficult for both physicians and patients. Dorairaj et al did complete a 6 month multicenter retrospective trial which compared phaco+KDB to phaco+iStent. Phaco+KDB had significantly more patients with IOP reduction >20% at 6 month follow-up (56.1% with KDB and 43.9% with iStent; p<0.05). Phaco+KDB also lowered IOP and medication usage more than Phaco+iStent in this study (3).
There are several techniques by which surgeons perform trabeculotomy and goniotomy. These have long been used in pediatric glaucoma to lower IOP but the usage of all techniques in adult open angle glaucoma has expanded as well. Other goniotomy or trabeculotomy techniques that you may have heard of include Gonioscopic-Assisted Transluminal Trabeculotomy (GATT), Trabectome (Neomedix Corporation, Tustin, CA), OMNI/Trab 360 (Sight Sciences, Manlo Park, CA), and traditional goniotomy with an MVR blade. GATT and traditional goniotomy are different from a KDB goniotomy in that in the first two procedures, the TM is cut, torn, or incised either with a suture (as in GATT) or an MVR blade or needle (as in traditional goniotomy). These first two procedures, therefore, leave residual TM leaflets that my scar closed later on. Trabectome removes TM with an electrocautery device but has also been shown to leave TM leaflets and can cause thermal injury to the surrounding tissue. In contrast, KDB goniotomy uses a novel dual blade design to more completely remove the TM from the nasal angle without causing significant damage to the surrounding tissues. This has been demonstrated to be true histologically in comparison to Trabectome and MVR blade (4). A study published in 2019 compared 6-month surgical outcomes of 360 trabeculotomy (GATT or Trab 360) to KDB. In their study, at 6 months, surgical success was similar between GATT or Trab360 eyes and KDB eyes. However, significantly more eyes in the KDB group achieved IOP ≤ 18mmHg (80% vs 59.3%; p=0.04) and ≤ 15mmHg (61.4% vs 25.9%; p=0.003). Mean IOP and medication reduction were also similar between the two groups (5). Another study of 73 eyes compared phaco+KDB to phaco+Trabectome at 12 months. At one year, success rates, defined as IOP of ≤ 21 mmHg and IOP reduction of at least 20% from baseline, or reduction of at least 1 glaucoma medication, was similar between the groups at 88.9% and 77.3% for phaco-KDB and phaco-Trabectome groups, respectively (6).
Good candidates for KDB
So now that we’ve briefly reviewed the data, who should you consider performing KDB goniotomy on? There are multiple things to consider when deciding on a surgical approach for any patient. As a versatile MIGS option, KDB can be performed in combination with cataract surgery, but also in pseudophakic patients or in phakic patients as a stand-alone procedure.
One obvious factor is their type and severity of glaucoma. Additional factors you should consider are their IOP goal or target, their starting IOP and the patient’s personal surgical goal (IOP control, medication independence, halt progression of disease, etc.). KDB is approved for the treatment of open angle glaucoma and ocular hypertension. It can be used in patients with any disease severity as well. Remember though that while angle-based procedures which work on the TM can successfully lower IOP, aqueous outflow still depends on the downstream outflow system and therefore cannot lower IOP below episcleral venous pressure (i.e. 8-10mmHg). Thus, KDB and other goniotomy procedures may not be ideal for patients with a very low IOP goal. Nor are they indicated for use in patients with elevated episcleral venous pressure.
KDB has shown particular success in patients with secondary open angle glaucoma such as pseudoexfoliation, pigment dispersion, and steroid-induced glaucoma (2). In all of these instances, the disease process occurs at the TM, therefore removal of the TM makes sense (2,7). Lastly, while primarily used in patients with open angles, KDB can be used in some, but not all patients with angle closure. In patients with relatively small areas of peripheral anterior synechiae (PAS) or in those with relatively recent angle closure, goniosynechiolysis followed by KDB goniotomy can often be performed safely. Goniosynechiolysis can be performed via your preferred method but can also be performed with the footplate of the KDB.
Details regarding their glaucoma often drive the decision-making process, but with that said, always remember to consider the whole patient. To perform most angle surgery, you need a cooperative patient with a clear cornea. During the KDB procedure specifically, which may take at least a few minutes even for an experienced surgeon, the patient has to rotate their head approximately 30-45° away from you, the surgeon, then look in a specific direction and not move. Therefore, avoid patients with a history of neck injury or those who can’t turn their neck or are unable to stay still. Lastly, remember to choose a patient with a clear cornea. Small scars or opacities outside of the visual axis you can usually work around but you ideally want as clear a view as possible. Can you see their angle easily during in-clinic gonioscopy? If so, then the cornea is probably clear enough for your case.
Remember to review their systemic medications pre-op as well. If a patient is on blood thinners such as aspirin, this does not need to be stopped. For patients on warfarin or other newer anticoagulant medications, consider a temporary cessation a few days prior to surgery with the approval of their cardiologist or primary care physician as they are likely at higher risk for hyphema.
Poor candidates for KDB
KDB is not indicated in patients with elevated episcleral venous pressure, active angle neovascularization, or angle dysgenesis. Any patient with non-identifiable angle structures is also not a good candidate. It may be performed in certain cases of chronic or acute angle closure, although we would not recommend starting out with these cases. Eyes with minimal angle pigmentation can make identification of angle structures difficult. So, avoiding these eyes for your first few cases and choosing those with more dense pigmentation of the TM is certainly helpful. As described above, any angle procedure, including KDB should be avoided in patients with corneal opacities which obscure your view of the nasal angle and in those who cannot turn their head and neck or follow instructions appropriately. Patients on blood thinners are not contraindicated but special consideration should be given in these situations, especially if the patient is monocular.
Pre-op counseling - What to tell patients before surgery?
As with all surgeries, accurate and thorough pre-operative counseling is key. A good rule to live by when possible is under-promise and over-deliver. We describe the procedure to patients as a way to open the natural drainage system of the eye, like unclogging a sink drain, as we have found that most patients will understand that metaphor. For patients undergoing KDB along with phaco, inform them that it will lengthen their procedure slightly, review the additional risks, and go over what to expect the day of surgery. Always make sure they understand why you are doing this procedure as well, such as “we are doing this to try to get your pressure lower” or “to try to get you off of some of your glaucoma drops.”
Lastly, always review what they can expect after surgery. Hyphemas can be asymptomatic, significantly limiting visually or range anywhere in between. We explain to patients before surgery that they should expect some bleeding during surgery, but that it is an expected event after this type of surgery. The blood may blur their vision post-op for a few days up to a week or more. It is important to remind them this isn’t their friend’s cataract surgery where they were 20/20 day 1, and they should expect blurred and fluctuating vision for at least a few days. If the hyphema is absent or minimal and they’re seeing great, they will think you are wonderful and if they have a significant hyphema, they were prepared for it. Also, review activity restrictions post-op, especially in patients on blood thinners or those at high risk of bleeding. Warn patients of the risk of re-bleeds, which happens around 3-5 days post-op, if at all. Further, many surgeons use carbachol or Miostat at the end of a KDB case. This will usually lead to a miotic pupil, dim vision, and a possible headache post-op day 1. Warn your patients of the expected headache or brow-ache so that you aren’t fielding emergency headache calls the night of surgery and having to explain it to an anxious patient. Lastly, we like to warn patients that IOP may fluctuate post-op due to bleeding, inflammation, possible steroid response, etc. This way if they have an IOP spike post-op week 1 or their IOP is not as low initially as you had hoped, again they were warned and are not surprised by this.
Learning how to perform KDB Goniotomy and tricks of the trade
Before your first case, as with any surgery, it’s important to practice. This includes watching instructional videos, reading up on surgical techniques, and doing wet labs. Your New World Medical surgical representative should have a great wet lab to work with you on before your first few cases and they can usually be present with you in the operating room (OR) when necessary (check with your surgical center regarding COVID regulations and representatives). Contact your local rep for assistance with this.
After teaching this procedure to multiple residents, fellows, and new attendings, we have noted that each struggle or succeed in different areas. One area where surgeons struggle is in properly identifying the TM, especially in lightly pigmented individuals. So, let’s review a few tricks you can use to help you identify the proper landmarks in this instance. The first is simple, practice gonioscopy in clinic and in the OR. Practice identifying all angle structures and have someone confirm your findings. On routine phacos, turn the patient’s head and your microscope just like you would for any angle surgery and practice identifying the structures. You can even take a blunt instrument like a Sinsky hook and touch the TM or practice the gliding movement. Intraoperatively you can find the TM if you’re struggling with two easy tricks, use Trypan blue or look for blood reflux. Trypan blue stains the trabecular meshwork, making it, you guessed it, blue, which in turn makes for easy identification of the TM. If you are performing your KDB prior to phaco, just use Trypan blue intracameral before placing viscoelastic to stain the TM (Figure 2).


Figure 2: Trypan Blue staining of the trabecular meshwork. Photo courtesy of Bac Nguyen and New World Medical.
If you are performing your KDB after phaco though, you may notice the TM is no longer blue, because the irrigation during phaco rinsed it away. In this instance, you can remove viscoelastic, place more Trypan, then refill with viscoelastic. Another way to identify the TM is to look for blood reflux into the Canal of Schlemm (SC) (Figure 3). In some patients this is prominent, but in others, you may need to lower the IOP. Burp or remove some viscoelastic and then look at the TM again and you should notice it has a reddish hue.

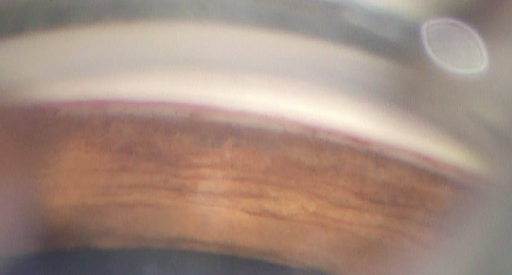
Figure 3: Blood Reflux in the Canal of Schlemm
Another area where new surgeons struggle is balancing the gonioprism on the eye with their non-dominant hand. This is just as it is described, a very delicate balancing act and not an intuitive skill. It takes practice. So as mentioned above: practice, practice, practice, BEFORE your first cases. Too much pressure on the gonioprism and you will get corneal striae which will block your view. Too little pressure and you will get air bubbles in the cornea-gonioprism interface and have no view (Figure 4). You definitely don’t want to lose your view while the blade is in position either. Never advance a blade that you cannot see. Also, if you have blood on your surgical field, either from a wound near conjunctival vessels or from a sub-tenon’s block, for instance, ensure the blood is wiped away from the cornea prior to placing your viscoelastic and gonioprism. Blood in the interface will obscure your view and is difficult to clean off.

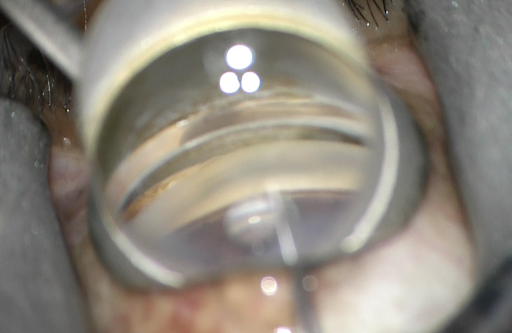
Figure 4: Air bubble in viscoelastic-cornea-gonioprism interface blocking view of blade and TM
Once you pierce the TM with the blade it should slide or glide within SC. You should NOT encounter resistance and neither the eye nor the iris should move. Residents in particular sometimes struggle with the lack of tactile feedback in this step. Several we have worked with have expressed that they feel like they should encounter resistance when in actuality, it’s all visual. You should confirm that you are in the right spot and then advance your blade. If you encounter resistance, usually the blade tip has embedded itself in the outer wall of SC. In which case the eye will rotate and the blade will stop advancing. Do NOT keep pushing if this happens. Instead, gently back the blade up, drop the heel of the blade and pull the tip towards you a bit, then advance/glide again when there is no resistance. Sometimes you may also notice iris moving. It shouldn’t. If the iris is moving, either you hooked it with the blade tip, you are in the wrong spot, or there was either synechiae or a membrane overlying the TM and iris. If this happens immediately stop, back the blade up, and remove it from the canal carefully. Consider placing more viscoelastic to further deepen the AC and push the iris down away from you. If there are visible synechiae, lyse them with the footplate of the blade or perform goniosynechiolysis before proceeding.
Once you have removed the TM from the nasal angle, depending on your chosen technique, you may see a strip of TM in the AC, but still attached to the TM where you stopped. It is tempting to grab this strip and pull it out. Doing so can extend or lengthen the treated area which can be beneficial. But be careful, this strip can also be attached to iris or Descemet’s membrane and you could accidentally pull either of those and cause damage you didn’t intend to.
Surgical steps
First, let’s talk anesthetic options. Most of these cases are performed under topical or intracameral anesthesia only. Subtenon and retrobulbar blocks can be used as well but can make the procedure somewhat more difficult due to bleeding and the akinesia they produce. For ideal visualization of the angle, some patient cooperation with eye movement is often required and patients may not be able to do this if the aforementioned blocks are used. A similar difficulty can be encountered with general anesthesia. However, this can sometimes be overcome by tilting the patient’s head or rotating the microscope further. In cases where general anesthesia will be employed, it is important to discuss this with your anesthesia provider ahead of time as they will need to ensure the tube is secure during head and neck rotation. Further, you can suggest that they bend the tube so that it is directed away from the operative eye.
Moving onto the surgery itself. First, a paracentesis is created and intracameral lidocaine is instilled. Next, the AC is deepened with a cohesive viscoelastic and a temporal clear corneal incision of at least 1.5mm is created. In cases where goniotomy is combined with phaco, make your standard clear corneal incision. Try to avoid nicking limbal blood vessels during the formation of your corneal incisions, as this often leads to blood on the corneal surface which can make visualization of the angle very difficult. In combined cases, perform your phaco as you normally would. After the intraocular lens is placed and centered in the bag, more viscoelastic is then added if necessary to deepen the nasal angle and push the iris posteriorly. Ensure the eye is well formed but be careful not to overinflate the eye as this can cause the collapse of SC and difficulty with the procedure. Next, the patient’s head is tilted 30-45 degrees away from you and the microscope is tilted 45 degrees towards you. Viscoelastic should then be placed on the corneal surface or the underside of the gonioprism. Using your non-dominant hand, float the gonioprism on the corneal surface and visualize the nasal angle and all appropriate landmarks. Ensure that your view is optimal – if it is not, figure out why and fix it. If there is heme under the lens, rinse off the corneal surface and lens and reapply viscoelastic. If there are corneal striae, fill the anterior chamber with more viscoelastic as you are likely underfilled. It is also important to ensure an “en face” view of the angle, where your viewing angle is perpendicular to the TM. If it seems like you are looking in a downward or upward angle at the TM you should adjust the patient's head and/or scope so that you achieve the correct view. Focus and zoom in with the microscope during this time as well. Do not open the blade until all landmarks are verified. Next, with your dominant hand, insert the blade sideways through the corneal wound. Usually, the gonioprism is lifted during this time to allow visualization of the corneal wound. Be careful during wound entry and ensure the blade is held sideways so as not to scratch the corneal endothelium or engage the iris. Under direct visualization, advance the blade across the eye. The sharp tip of the blade should be used to pierce the TM, then flatten the heel of the blade so that it is lying flush with the posterior wall of SC. It can be useful to tilt the blade tip slightly anteriorly towards the cornea before piercing the TM to ensure iris is not engaged and then flatten the blade horizontally again once the TM is pierced. Once the heel of the device is seated within SC, advance the blade in whichever direction you intended for 3-5 clock-hours. This will produce a trabecular strip ahead of your advancing tip. You will also notice a white cleft posterior to the heel of the blade if done properly (Figure 5).

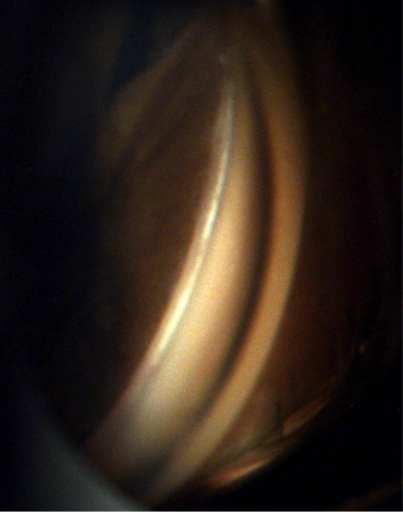
Figure 5: White appearing cleft noted after trabecular meshwork removal
While advancing the device, it is important to ensure that you are pivoting in your wound with the handle. Do not let the handle push against either edge of the wound as this will produce corneal striae or move the eye, both of which will impede your visualization. Depending on which technique you decide to employ (more discussed later), the device may then be flipped and these same steps done in the opposite direction. You may notice a small hyphema or blood reflux; however, bleeding should not be significant. If blood impedes your view, stop advancing the device, carefully remove it from the eye and use viscoelastic to displace the blood and visualize the area treated. Never treat an area that you cannot see clearly.
Once complete, carefully remove the blade from the eye under direct visualization again. A gentle side to side motion can be used to ensure no intraocular contents are stuck on the tip. If a large trabecular strip remains, it can be removed with intraocular forceps; however, it does not have to be. Be aware that the strip may be attached to the iris or Descemet’s membrane which, if pulled, can accidentally be removed or damaged along with the strip. The patient’s head and microscope are then returned to their original positions and viscoelastic is washed from the corneal surface. Irrigation and aspiration should be used to remove viscoelastic from the AC and carbachol (Miostat) intraocular solution can be placed intracamerally to produce pupillary miosis after completion of the case. Lastly, hydrate your wounds and refill the eye with a balanced salt solution. Ideally, the IOP should be kept slightly high immediately post-operatively, around 20-25mmHg to prevent significant blood reflux.
KDB techniques
There are three widely accepted techniques for performing goniotomy with the KDB:
- Inside-Out
- Outside-In
- The “Mark and Meet”.
The Inside-Out technique is where the surgeon enters the TM and SC directly across from the main wound and advances the blade to the extent of their view in one direction. The blade is then flipped in the opposite direction and enters SC at the same starting point, then advances this time in the opposite direction. This generally leaves two TM strips attached at the superior and inferior extent of the cleft created. The Outside-In technique is just the opposite. The device is advanced across the AC but starts either at the superior or inferior extent of the visualized nasal angle where it pierces TM and moves centrally towards the nasal angle directly across from the corneal wound. Again, the blade is flipped and this same process is completed from the opposite side. This technique generally produces a free-floating trabecular strip with no leaflets remaining attached. The Mark and Meet is a slight variation to those noted above and is designed to avoid a backhand pass. In this technique, the blade enters the TM/SC off-center and is advanced just slightly either superiorly or inferiorly depending on the surgeon's preference. It is then moved to the opposite end of the nasal angle and advanced until it meets the initial area treated or “marked”. For more details and video examples of each technique, visit https://www.newworldmedical.com/kdb-surgical-techniques-animation/. There is no “best” technique. In reality, the best technique is whichever is safest and most comfortable in your hands.
Post-operative care
Patients are generally seen post-op day 1, week 1, and month 1 just like a standard phaco post-op. However, if IOP is high or there is significant blood reflux and hyphema, they should be seen more often. For patients who underwent KDB goniotomy along with phaco, the standard post-op drop regimen can be followed which may include topical steroid, antibiotic and NSAID. For stand-alone cases, most surgeons use only a topical steroid and antibiotic. Pilocarpine 1% is also used by some surgeons to produce pupillary miosis and place tension on the scleral spur to ensure patency of the cleft in the early postop period. While anecdotally, and in theory, this may help improve outcomes, there remains little evidence demonstrating a benefit postoperatively. If you chose to use this, it can be tapered along with the topical steroid. Surgeons who decide to use pilocarpine should warn patients of the effects this will have on their vision post-op (tunnel vision, dim vision, blurred vision) and the possible headache/brow-ache associated with pilocarpine use.
The use of ocular anti-hypertensive agents post-op depends on the patient, particularly on their glaucoma severity. In patients with severe disease, it is safest to continue most, if not all, of their pre-op glaucoma regimen to prevent optic nerve damage from potential IOP spikes or failure of the procedure. These can then be tapered off later. However, if their disease is mild or moderate you may decide to stop some or all of their glaucoma drops initially and restart as indicated. It is important to remember though that these patients can still experience IOP fluctuation and spikes in the postoperative period. They can also experience a steroid response. We warn all patients about the risk of fluctuations within the first month so that when there are changes they are not alarmed. In cases of IOP spike due to steroid use, the steroid can be tapered faster or switched to an alternate agent such as loteprednol or fluorometholone. Keeping a patient on at least one ocular anti-hypertensive during the post-op period—ideally a prostaglandin analogue—can help blunt this response if it occurs.
Ideally, a shield should be worn over the operative eye at night for one week post-op and activity restrictions should be reviewed. Strict activity restrictions may be warranted for those with significant hyphema or those at risk of re-bleeds. It is a good idea to warn patients with hyphema or a clot that their vision will fluctuate as the hyphema resolves. It is usually worse in the morning upon awakening and clears throughout the day but may vary or worsen after strenuous activity, bending, etc. They can sleep with the head of the bed elevated if desired but it is not required.
Understanding how your front-line colleagues approach glaucoma is more important than ever. Download Eyes On Eyecare's free 2023 Glaucoma Report to see how your peers diagnose, treat, and manage this condition!
Billing and Financial considerations
It is always a smart idea to start learning about billing considerations in ophthalmology residency and fellowship, because once you are in practice, you will have to face the financial impacts of procedures. KDB goniotomy is convenient from a billing standpoint for a number of reasons. First, it has an established billing CPT code (65820) that is generally approved for the treatment of open angle glaucoma of any severity or ocular hypertension and is approved both in combination with phaco and as a stand-alone procedure. Costs to start performing this procedure are usually minimal because the device is a single-use, disposable handpiece. However, you may need to purchase several gonioprisms if your surgical center does not already have them. Additional costs that you have to consider are possible use of intracameral carbachol and the additional viscoelastic when compared to a phaco-only procedure.
Conclusions
Goniotomy with KDB is a highly versatile, safe and effective procedure for treating glaucoma and ocular hypertension. As with most glaucoma procedures, success hinges on proper patient selection. Appropriate patient education and counseling about the details of the surgery, its risks and benefits, and the post-operative experience should always be discussed with patients prior to the day of surgery. Any surgeon has the ability to perform KDB goniotomy safely and effectively but as with any new procedures, it requires careful and deliberate practice and preparation to optimize outcomes. Soon after getting underway, clinicians will realize the meaningful IOP and medication reductions that KDB goniotomy can provide to patients, making the KDB a welcome addition to the MIGS toolkit.
References
- Sieck ES, Epstein RS, Kennedy JB, et al. Outcomes of Kahook Dual Blade Goniotomy. Ophthalmology Glaucoma. 2018;1(1):75-81.
- Sieck ES, Epstein RS, Kennedy JB, et al. Two Year Outcomes of Kahook Dual Blade Goniotomy with and without Phacoemulsification Cataract Extraction. American Glaucoma Society. March 14, 2019, San Francisco, CA
- Doreiraj SK, et al. A multicenter retrospective comparison of goniotomy versus trabecular bypass device implantation in glaucoma patients undergoing cataract extraction. Clinical Ophthalmology; April 2018;12:791-797
- Seibold L. K., SooHoo J. R., Ammar D. A., Kahook M. Y. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. American Journal of Ophthalmology. 2013;155(3):524–529.e2.
- Hirabayashi MT, Lee D, King JT, Thomsen S, An JA. Comparison of Surgical Outcomes Of 360° Circumferential Trabeculotomy Versus Sectoral Excisional Goniotomy with the Kahook Dual Blade At 6 Months. Clin Ophthalmol. 2019;13:2017-2024.
- Dirghangi AJ, Netland PA, Roa TM, Comparison of two glaucoma surgical techniques, Kahook Dual Blade goniotomy versus Trabectome ab-interno trabeculotomy, in combination with cataract surgery. Investigative Ophthalmology and Visual Science; July 2019;60(9).
- Miller VJ, Young CEC, SooHoo JR, et al. Efficacy of Goniotomy With Kahook Dual Blade in Patients with Uveitis-associated Ocular Hypertension. J Glaucoma. 2019;28(8):744-748.
