



In the past few decades, the exponentially rising rate of myopia across the world, especially in the pediatric population, has researchers fighting to understand the root causes of myopia development and ways to help slow progression. In Asian countries, the prevalence of myopia is over 80%.1
Although it is well known that myopic eyes have a higher risk of developing comorbidities, such as retinal detachments and myopic maculopathy,2 there is one disease that has been overlooked in pediatrics with myopia: dry eye disease (DED). There are very few studies reporting on the incidence of dry eye in pediatrics.
It is often overlooked due to underreporting from patients as well as a lack of understanding of what dry eye symptoms entail. However, many children may have DED due to various external factors, such as allergies and systemic medications.
Furthermore, children who are myopic are often treated with soft daily multifocal contact lenses, orthokeratology, and atropine eye drops, which may further exacerbate dry eye. This article will explore various causes of dry eye in the pediatric population, more specifically those who are myopic.
Predisposing factors to dry eye in teens
Ocular allergies
Allergies are the fifth leading chronic condition in industrialized countries among all ages and the third most common chronic disease among children under 18 years old.3 However, there is currently minimal data on allergy epidemiology due to the fact that allergies are considerably underreported and may vary significantly depending on geographic location.
Symptoms of ocular allergies, such as excessive lacrimation, can affect the stability of the tear film and reduce goblet cell density, especially in children wearing contact lenses, leading to DED.4 Therefore, pediatric patients with pre-existing ocular allergies may not be as tolerant to CL wear, which can present a challenge when presenting modern myopia control options.
Eyestrain/screen use
It is well known that increasing eyestrain from digital device use is associated with an increase in myopia and DED. Teenagers today are exhibiting frequent blinking, sensitivity to light, and other dry eye ocular discomfort.5 However, DED is not always reported by the patients, resulting in a discrepancy between dry eye signs and symptoms.
For example, a study by Wang et al., 2022 found that 15.9% of patients reported symptoms of DED; however, MGD was observed in 30% of patients (See Figure 1 below).6 These findings were supported by Wan et al., 2015 who reported that increased use of digital devices led to reduced blink rates, which in turn led to reduced meibum secretion.7
Figure 1 illustrates different meibomian gland morphologies in ametropic children. (A)0-25% area of loss (B) 25-50% area of loss (C) 50-75% area of loss (D) Meibomian glands were twisted and some meibomian glands were twisted more than 90°.

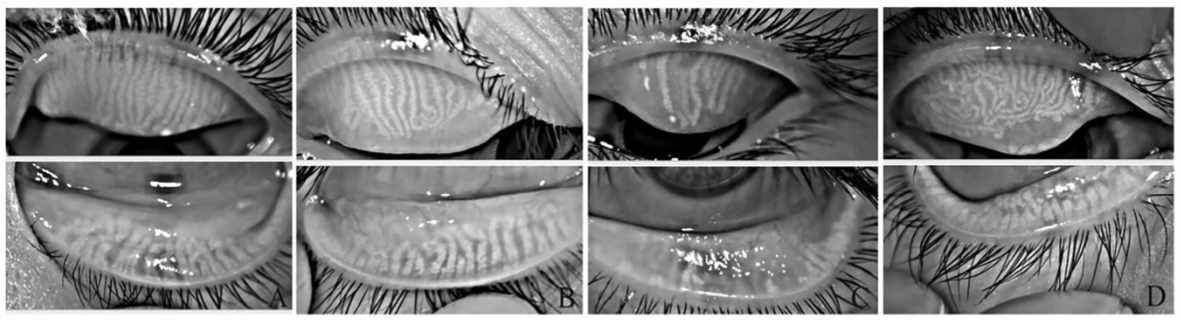
Figure 1: Wang et al., 2022
Medications
Oral antihistamines
As stated earlier a significant proportion of the pediatric population experiences allergies, including ocular allergies. Therefore, they are likely taking oral antihistamines, which have been found to reduce tear volume and exacerbate DED.8 When comparing the effects of oral vs. topical antihistamines, Ousler et al., 2007 found that oral antihistamines exacerbate DED in patients compared to topical options.9 Therefore, it may be worth discussing discontinuing oral antihistamines and switching to a topical alternative with your patients.
When considering myopic patients who are wearing contact lenses, topical antihistamines may disrupt the tear film and cause blurriness upon installation. This can be avoided by recommending a drop that is instilled once a day at bedtime.
Antidepressant medications
According to The Pharmaceutical Journal, the rate of prescribing antidepressants to children aged 5-12 years has increased by more than 40% between 2015 and 2021.10 One of the most commonly prescribed medications for the treatment of depression is serotonin reuptake inhibitors (SSRIs), which inhibit serotonin (5-HT) transport. This increase in serotonin concentrations can activate inflammatory cytokines proven to trigger DED.11
Another study by Li et al., 2011 supported these findings when authors found that patients using an SSRI have a 1.5x increased risk of DED compared with that of patients using other types of psychotropic medications or not using these medications at all. Therefore, taking these types of medications may increase dry eye prevalence in adolescents.12
Oral isotretinoin (Accutane)
Isotretinoin, also known as Accutane, is an active form of Vitamin A and is mainly used to treat acne in young adults. However, this medication may have serious side effects, including on the eyes. It was discovered that oral isotretinoin can cause alterations to the function and structure of the meibomian glands and inhibit the production of lipids, leading to increased tear evaporation.13
Oral contraceptives
It has been found in past studies that sex hormones, such as estrogen, can potentially affect the structural and functional aspects of the eye thereby leading to DED.14 Estrogen, which is a hormone found in oral contraceptives, has been linked to a decrease in lipid production and size of the sebaceous gland.15
Atropine
Atropine is a common topical medication used in myopia management that is instilled in the eye once at nighttime. Dryness and light sensitivity symptoms have been found in patients with atropine use; however, Coroi et al., 2015 found that these symptoms are more likely due to the preservatives in the formulations instead of the atropine drop itself.16
Furthermore, in the LAMP study, a major study looking at atropine’s effect on reducing myopia progression, authors found that the occurrence of allergic conjunctivitis and dry eyes was the same across all groups, all of which used a preservative-free form of atropine.17
Binocular vision
Numerous studies have found that binocular vision disorders can lead to asthenopia (visual fatigue), and that both have been linked to DED. In a study by Rouse et al., 2009 researchers investigated the relationship between contact lens induced dry eye symptoms and binocular vision disorders. They found a significant correlation between the severity of symptoms on the Ocular Surface Disease Index (OSDI) and the Convergence Insufficiency Symptoms Survey (CISS).18
This correlation was greater than any correlations between OSDI and signs of dry eye. Therefore, their results indicated that dry eye symptoms were more closely linked to binocular vision disorders than to dry eye clinical signs.
Rueff et al., 2015 evaluated the incidence of binocular vision disorders in non-presbyopic myopic contact lens wearers with self-reported dry eye symptoms. They found more than 48% of myopic subjects had a binocular vision disorder, the most common being an accommodative lag of one diopter or more, and the second being a pseudo-convergence insufficiency.
Therefore, there is likely a strong correlation between dry eye symptoms, contact lenses, binocular vision disorders, and myopia.19
Higher order aberrations (HOA), choroidal thickness, and axial length
Previous studies have reported a correlation between ocular HOAs and myopia. Total ocular HOA were found to be higher in children in whom myopia progressed rapidly (SE > 0.50 D/year).20 Hazra et al., 2022 found a negative correlation between HOA and TBUT in children. In other words, as HOAs increased, TBUT decreased.
Furthermore, choroidal thickness increased resulting in decreased axial length. Therefore, HOA, TBUT, and choroidal thickness are suggested to be highly correlated.
The authors postulated two theories on the relationship between TBUT and choroidal thickness:21
- First, since increased parasympathetic tone enhances both the choroidal thickness and amount of tear secretion from the lacrimal glands, their results suggest a “factor X” that includes the parasympathetic nervous system and might be a common factor between dry eye and myopia.
- Secondly, a simpler explanation would be that those who perform more near work have a greater increased risk of both evaporate DED, which affects the TBUT, and choroidal thickness, which affects the axial length.
Figure 2, below, by Hazra et al., 2022 provides a nice summary of their findings.21 It illustrates the scheme of the relationships among the tear film breakup time (TBUT), higher order aberrations (HOAs), choroidal thickness (CT), and axial length (AL) from the results of the current study. The TBUT is associated significantly with the CT that is related to the AL. The TBUT is correlated with the corneal HOAs but not with the total ocular HOAs, whereas the AL is related to the total ocular HOAs but not to the corneal HOAs. Because the parasympathetic nervous system affects both the lacrimal glands and CT, it might be a common factor upstream in the association between the TBUT and CT.

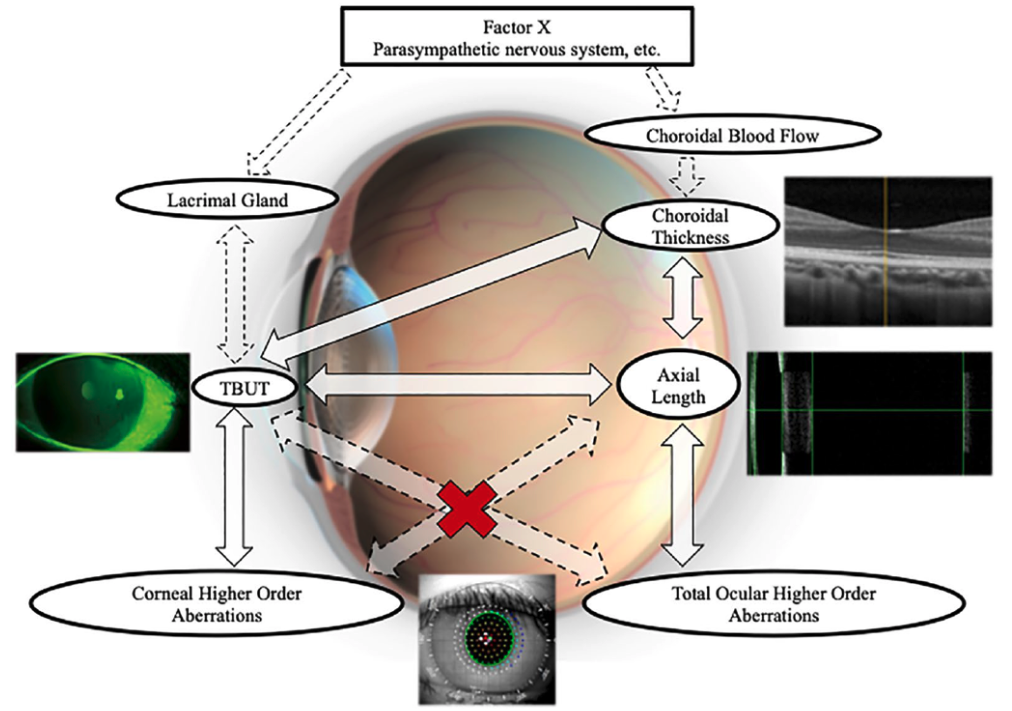
Figure 2: Hazra et al., 2022
Contact lens
Very few studies have been performed which evaluate dry eye complaints in pediatric contact lenses; therefore, we have limited data. Using a contact lens dry eye questionnaire (CLDEQ), one study by Greiner et al., 2010 looked at the percentage of reported dry eye in children versus adults who wear soft contact lenses. They found that only 4.3% of children were categorized with dry eye compared to 56.2% of adults. This difference may be due to differences in tear chemistry, but children may also be less likely to report symptoms due to a lack of understanding of dry eye.22
Although not much has been reported in terms of soft contact lenses and dryness in pediatrics, there have been a few studies that looked at orthokeratology in children and dry eyes. Zeng et al., 2020 found that a greater percentage of patients demonstrated increased partial blinks after they were fitted for orthokeratology.23
Furthermore, Cho et al., 2020 reported tear film instability ascribed to orthokeratology-induced irregular corneal surface changes.24 Luckily, many of these findings seem to be short-term interruptions in the first few months of starting orthokeratology that are reduced in the long-term.25
Treatment of dry eye in myopic patients
Ocular allergies
As Ousler et al., 2007 showed in their study, topical allergy drops have minimal to no effect on tear volume, tear flow, or fluorescein staining.9 Therefore, if a patient is having mostly ocular allergies, it is strongly recommended to switch from oral to topical antihistamines. Newer-generation antihistamines (e.g., olopatadine, alcaftadine, azelastine, epinastine, and ketotifen) are much more convenient. They are instilled twice daily, at least 15 minutes prior to lens insertion and after its removal.
If the patient is unable to take topical medication or has to take oral antihistamines for other allergies, try changing to newer more site-specific (H1 selective) antihistamines, such as Zyrtec or Clarinex, as they are less likely to cause ocular dryness although they may still affect the tear film.
If the patient is also wearing soft contact lenses to treat myopia, patients should try to wear daily disposables, since it has been shown to reduce ocular allergies compared to extended wear. Wolffsohn et al., 2011 took it one step further and compared allergy symptoms in patients wearing two types of daily disposable lenses, one with enhanced lubrication and one without. The authors found that daily lenses with enhanced lubricating agents provided an additional barrier against allergen penetration in comparison to the other group.26
Eye strain/screen use time
The best solution to combat dryness from screen use is to reduce screen time to less than 1 hour a day. This may not be possible considering many schools have now switched from paper to tablets; however, it is still important for the patient to follow the 20/20/20 rule.
The 20/20/20 rule
Take a 20 second break every 20 minutes to look at something further than 20 feet away.
It is important to reiterate this to both the patient and parent when they are in the exam chair as many are unaware of the harmful effects of excessive screen time.
Medications
In regard to certain oral medications, such as isotretinoin, birth-control, and antidepressants, discontinuation may not be an option. However, there are other options including changing to another drug class or reducing the dosage of the medication. For topical medications, such as atropine, consider switching to a preservative-free solution.
Binocular vision
In adolescent patients, it is important to assess for binocular vision disorders, especially those that have dry eye symptoms and are myopic. As stated earlier nearly 50% of myopes have an underlying binocular vision disorder. If a binocular vision disorder is discovered, it is important to treat that first before starting with dry eye therapy.
Contact lenses
When considering orthokeratology for adolescents, we must assess the ocular surface condition. It is important that the patient does not show any signs of significant DED, because as stated before, orthokeratology can reduce blink rate and therefore increase dry eye signs and symptoms. We must continue to assess for dry eye throughout treatment and treat with preservative-free lubricants when needed.
Furthermore, high myopes can be more prone to increased corneal staining, discomfort, and dryness. Therefore, clinicians should consider partial reduction if that patient is experiencing these symptoms.27
In regard to soft contact lenses, studies have shown that switching patients from extended wear to daily disposables can help reduce tear film disruption.28 Furthermore, multiple studies have shown that switching patients from hydrogel to silicone hydrogel lenses has shown an improvement in the symptoms of dryness.29,30
Patient/parent education
As mentioned earlier, Greiner et al., 2010 found that children may be less likely to report dry eye symptoms because they are too timid to speak up or are unsure of what is to be considered dry eye symptoms.22 Thorough education on signs and symptoms of dry eye to the patient and parents are crucial in preventing DED from worsening in our myopic population.
In conclusion
It is believed DED is often overlooked in children, even in those who wear contact lenses, because they rarely report any ocular discomfort. However, dry eye can affect their vision, tear film stability, and success with myopia control treatments. Therefore, it is still important to use objective measurements when diagnosing dry eyes. These include using a slit lamp to look for fluorescein staining, and, if available, a topography/meibographer to observe tear break up time and meibomian gland function.
As clinicians, it is up to us to diagnose and manage DED early, so we can improve the quality of life for our patients.
References
- Lin LL, Shih Y F, Hsiao CK and Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33: 27–33
- Pierro L, Camesasca FI, Mischi M, Brancato R. Peripheral retinal changes and axial myopia. Retina. 1992;12:12–17.
- American College of Allergy, Asthma, and Immunology. (2018). Allergy Facts. https://acaai.org/news/facts-statistics/allergies
- TodaI, ShimazakiJ, TsubotaK. Dry eye with only decreased tear-up time is sometimes associated with allergic conjunctivitis. Ophthalmology. 1995; 102:302–309.
- J. H. Moon, M. Y. Lee, and N. J. Moon, “Association between video display terminal use and dry eye disease in school children,” Journal of Pediatric Ophthalmology and Strabismus, vol. 51, no. 2, pp. 87–92, 2014.
- Wang N, Zhuang X, Zhong X, Zhang J, Li G, Li S. Questionnaire Analysis on Incidence and Risk Factors of Dry Eye in Children From a Myopia Outpatient Clinic. Front Med (Lausanne). 2022 Feb 14;9:846709.
- Wan T, Jin X, Lin L, Xu Y, Zhao Y. Incomplete blinking may attribute to the development of meibomian gland dysfunction. Curr Eye Res. (2016) 41:179–85. Doi. 10.3109/02713683.2015.1007211
- Hom M. Is it the medication? Optom Mgmt. 2000;35(2):92-6.
- Ousler GW 3rd, Workman DA, Torkildsen GL. An open-label, investigator-masked, crossover study of the ocular drying effects of two antihistamines, topical epinastine and systemic loratadine, in adult volunteers with seasonal allergic conjunctivitis. Clin Ther. 2007 Apr;29(4):611-6.
- The Pharmaceutical Journal, PJ, September 2021, Vol 307, No7953;307(7953): DOI:10.1211 /PJ.2021.1.104115.
- Simmons KT, Xiao Y, Pflugfeldera SC, de Paiva CS. Inflammatory response to lipopolysaccharide on the ocular surface in a murine dry eye model. Invest Ophthalmol Vis Sci. 2016;57: 2443–2451.
- Li M, Gong L, Sun X, Chapin WJ. Anxiety and depression in patients with dry eye syndrome. Curr Eye Res. 2011;36:1–7.
- Moy A, McNamara NA, Lin MC. Effects of isotretinoin on meibomian glands. Optom Vis Sci. (2015) 92:925–30.
- Sullivan DA. Tearful relationships? Sex, hormones, the lacrimal gland, and aqueous-deficient dry eye. Ocul Surf. 2004; 2(2):92–123.
- Sullivan DA, Yamagami H, Lui M, et al. Sex steroids, the meibomian gland and evaporative dry eye. Adv Exp Med Biol. 2002; 506(Pt A):389–399.
- Coroi MC, Bungau S, Tit M. Preservatives from the eye drops and the ocular surface. Rom J Ophthalmol. 2015 Jan-Mar;59(1):2-5
- Yam JC, Jiang Y, Tang SM et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study. Ophthalmol.126:113-24 (2019).
- Rouse M, Borsting E, Mitchell GL, Cotter SA, Kulp M, Scheiman M, Barnhardt C, Bade A, Yamada T. Validity of the convergence insufficiency symptom survey: a confirmatory study. Optom Vis Sci. 2009;86:357-363.
- Rueff EM, King-Smith PE, Bailey MD. Can Binocular Vision Disorders Contribute to Contact Lens Discomfort? Optom Vis Sci. 2015;92:e214-221.
- Zhang, N. et al. Relationship between higher-order aberrations and myopia progression in schoolchildren: A retrospective study. Int. J. Ophthalmol. 6, 295–299 (2013).
- Hazra, D., Yotsukura, E., Torii, H. et al. Relation between dry eye and myopia based on tear film breakup time, higher order aberration, choroidal thickness, and axial length. Sci Rep 12, 10891 (2022).
- Greiner KL, Walline JJ. Dry eye in pediatric contact lens wearers. Eye Contact Lens. 2010 Nov;36(6):352-5.
- Zeng, L., et al., Tear Lipid Layer Thickness in Children after Short-Term Overnight Orthokeratology Contact Lens Wear. Journal of Ophthalmology, 2020. 2020.
- Cho, W.-H., et al., Analysis of tear film spatial instability for pediatric myopia under treatment. Scientific Reports, 2020. 10(1): p. 1-9.
- Na K. S., Yoo Y. S., Hwang H. S., Mok J. W., Kim H. S., Joo C. K. The influence of overnight orthokeratology on ocular surface and meibomian glands in children and adolescents. Eye & Contact Lens: Science & Clinical Practice. 2016;42(1):68–73.
- Wolffsohn J, Emberlin JC. Role of contact lenses in relieving ocular allergy. Contact Lens Anterior Eye 2011; 34: 169-72.
- Hu, P., et al., The safety of orthokeratology in myopic children and analysis of related factors. Contact Lens and Anterior Eye, 2021. 44(1): p. 89-93.
- Nichols, J.J., Mitchell, G.L., Nichols, K.K., et al. The performance of the contact lens dry eye questionnaire as a screening survey for contact lens-related dry eye. Cornea. 2002;21(5):469-75.
- Chalmers, R., Long, B., Dillehay, S., et al. Improving contact lens related dryness symptoms with silicone hydrogel lenses.Optom Vis Sci. 2008;85(8):778–84.
- Fonn, D., Situ, P., Simpson, T. Hydrogel lens dehydration and subjective comfort and dryness ratings in symptomatic and asymptomatic contact lens wearers. Optom Vis Sci. 1999;76: 700–704.
