


This report will walk you through the fluorescein angiography (FA) procedure, indications, and results. It will also introduce you to FA’s sister procedures: indocyanine green angiography (ICGA) and fundus autofluorescence (FAF). These all serve as valuable tools for identifying and monitoring retinal pathology.
The purpose of fluorescein angiography
The purpose of FA is to evaluate the retinal blood flow and analyze retinal perfusion and choroidal vasculature. This can be a useful tool for an array of conditions, including (but not limited to) hereditary retinal disease, age-related macular degeneration (AMD), diabetic retinopathy, central serous chorioretinopathy (CSR), ischemic optic neuropathy, suspicious choroidal nevi (versus melanoma), and retinal vascular occlusions. It can also be used to investigate cases of unexplained vision loss and used on the anterior segment to outline iris rubeosis.
Performing the procedure
The procedure involves injecting fluorescein dye, a vegetable-based dye, intravenously, most often into the antecubital vein of the arm; then, a retinal camera, equipped with the proper excitation filters and barriers, is used to obtain photographic images.
A white light flash is emitted from the camera and passes through a blue excitation filter. Fluorescein molecules absorb the blue light and fluoresce. This emits light of a longer wavelength in the yellow-green spectrum. The barrier filter allows for only the light of interest from the excited fluorescein to be captured in the images.
After the dye is injected, it travels to the eye approximately 10-15 seconds, first filling the short posterior ciliary arteries and appearing in the optic nerve and choroid. In elderly patients and those with poor cardiovascular health, the dye may have an increased transit time, more like 20 to 30 seconds. Also, if the dye is injected at a slower speed or the injection is performed into a vein in the back of the hand, instead of the antecubital vein in the arm, this will increase transit time.
Images are acquired immediately after injection every 1 to 3 seconds for the first minute, and then every minute (or so) out to about 10 to 12 minutes. The initial choroidal flush appears as a patchy-patterned hypofluorescence and is followed by the appearance of the dye in retinal circulation a few seconds later. First, there is filling of the arteries, arterioles, and capillaries within the early arteriovenous phase.
During the later arteriovenous phase, the veins fill in a laminar pattern with dye coursing along the outside walls first and then then filling centrally. The dye then circulates out of the retina with most of it no longer seen by the 10-minute mark. A few ocular structures may continue to fluoresce after this point, including the optic nerve head, Bruch’s membrane, and the sclera.1,2
Reading the images
When reviewing FA images, the main concept to master is how to interpret hypofluorescence and hyperfluorescence. Hypofluorescence occurs when there is either a blockage or a filling defect.
Examples of a blockage could be a vitreous hemorrhage or congenital hypertrophy of the retinal pigment epithelium (RPE), while a filling defect is usually due to vascular non-perfusion. Filling defects can be caused by cardiovascular disease or vaso-occlusive disease with bilateral findings more likely in the former and unilateral in the latter.
Hyperfluoresence can result from leakage of blood or fluid through compromised blood vessels—from a choroidal neovascular membrane, for example—and appears as an enlarging cloud of dye in the affected area. Pooling and staining of dye within ocular structures also creates hyperfluorescence, but these have more contained patterns. Pooling occurs in spaces that are fluid filled, while staining appears more distinct and outlines the structure or area.
Hyperfluorescent “window defects''occur when dye is viewed through a layer that would normally block it; this is commonly seen with disrupted RPE in dry macular degeneration.1
Irregular optic nerve filling on FA can be indicative of disease. In optic atrophy there is a lack of capillary perfusion so the nerve will appear hypofluorescent. On the contrary, in optic disc edema there is fluid accumulation around the nerve and thus will appear hyperfluorescent, though the edema usually causes a delayed fill.1
Macular findings can pinpoint pathology as well. The macula normally appears dark on FA due to the foveal avascular zone and blockage of fluorescence by the retinal pigment. One of the more common pathologic findings is a petaloid hyperfluorescent pattern in cystoid macular edema (CME), due to fluid leaking and spreading in the outer plexiform layer. RPE detachments cause small areas of pooling within the fluid space.
Choroidal neovascular membranes (CNVM) at the macula produce progressive clouding and hyperfluorescence as leaking occurs. CSR presents as a “smokestack” or “ink blot” of spreading hyperfluorescence.2
Image 1 demonstrates a patient with peripheral retinal nonperfusion, retinal neovascularization, and neovascularization of the disc secondary to proliferative diabetic retinopathy of both eyes. The nonperfusion area is dark due to non-filing and the neo-vascularized regions are viewed as expanding clouds of hyperfluorescence.

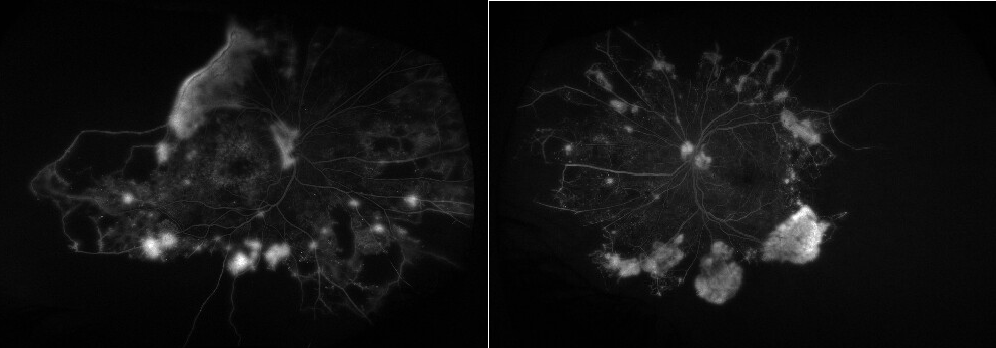
Image 1
In Image 2, a patient with non-exudative AMD on FA, window defects are hyperfluorescent, well-demarcated areas is represented.

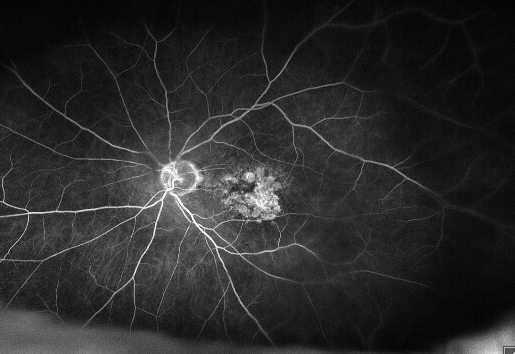
Image 2
Image 3 of a patient with exudative AMD, the hyperfluorescent area expands as a cloud due to leakage.

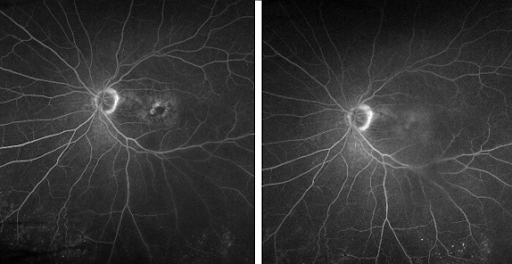
Image 3
Risks and adverse effects
Before the procedure can be performed, a written consent form must be reviewed and signed. The purpose of the test should be clearly stated and the possible adverse effects made known. This may include transient nausea right after the injection.3 This is rare but more often occurs in younger patients and is thought to be the result of faster circulation of the dye through the body. If it does occur, this nausea usually passes quickly as “waves” within the first one to three minutes of the angiogram.
The patient should also be alerted that the dye will pass through the body creating discolored, yellow to orange urine for a few days. It may also cause a temporary, slight yellow tinge to the cheeks or other areas of the skin a few hours after the procedure. A risk of urticaria, syncope, and anaphylaxis also exist. The risk of anaphylaxis is rare (approximately 1 in 200,000).1,3 It is recommended to use a half dose of fluorescein dye in patients who suffer from kidney disease.
Pregnancy is a relative contraindication for the procedure, since the effects are not known; unless it was a true ocular emergency, the test is not recommended.1,2
Indocyanine green angiography
ICGA is like FA but is more useful in conditions involving choroidal blood flow and associated retinal pathology. ICG is a water-soluble cyanine and iodine-based dye that fluoresces in the near-infrared range. Due to its protein-binding properties, ICG leaks less from the choriocapillaris and remains in the choroidal vasculature for a longer time than fluorescein dye. Some examples of conditions that may benefit from ICG are CNVM, polypoidal choroidal vasculopathy, choroidal melanoma, choroiditis, and CSR.
Due to the iodine-base chemistry, an iodine or shellfish allergy is a contraindication. Patients with liver disease should also not have ICGA. Like FA, pregnancy is a relative contraindication since the effects are not known; it is not performed unless an ocular emergency. The timeline for ICGA runs longer than FA with the early phase occurring in the first 60 seconds, the mid-phase at 5-15 minutes, and the late phase around 18-30 minutes.4
Image 4, below, represents CSR in the left eye with view on macular optical coherence tomography (OCT) and ICGA. The serous retinal detachment can be observed on the OCT study and the diffuse clouding of dye at and above the macula on ICGA is due to increased choroidal vascular permeability in this condition.

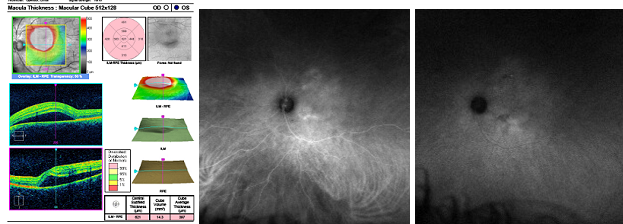
Image 4
Fundus autofluorescence
Fundus autofluorescence(AF) is another helpful tool in the diagnosis and monitoring of retinal disease. FAF provides us with functional information about retinal cells by mapping lipofuscin within the RPE. Areas of increased lipofuscin concentration will appear hyperfluorescent, while hypofluorescence will be present in areas where RPE cells have atrophied or are absent.
The latter is exhibited in cases of geographic atrophy. At the border of geographic atrophy, there is often a hyperfluorescent “halo.” This region represents “sick” RPE cells that are facing imminent atrophy.
Retinal dystrophies can also exhibit their own patterns of abnormal autofluorescence representing the atrophic regions and the “sick” regions of the retina.5
In Image 5, dry AMD can be observed as a hypofluorescence in areas of atrophy with a hyperfluorescent halo on FAF.

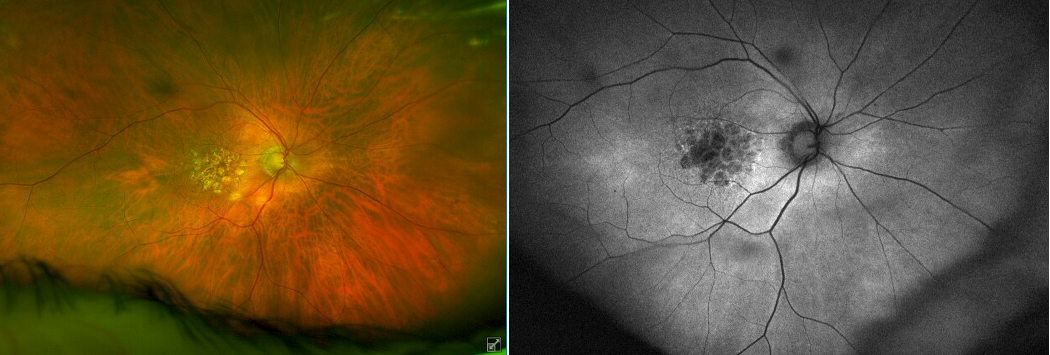
Image 5
In Image 6, we see a diabetic patient with an “hourglass retinal hemorrhage” (partial subretinal and partial preretinal) of the left eye. The hemorrhage blocks autofluorescence.

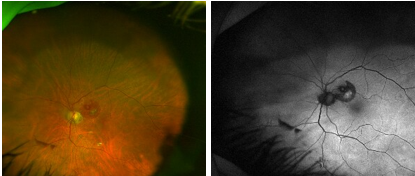
Image 6
Conditions of Note
While FA is a great tool for diagnosing a plethora of retinal pathologies, there are certain conditions that warrant timelier and or more frequent procedures. The top three are:
- Diabetic retinopathy.
- Age-related macular degeneration.
- Hypertensive/ischemic retinal pathology.
Diabetic retinopathy
When a patient has severe, non-proliferative diabetic retinopathy or proliferative diabetic retinopathy, FA may be performed on a regular basis such as annually, biannually, or even quarterly depending on the case. Additionally, in some diabetic retinopathy cases it may be difficult to distinguish factors such as intraretinal microvascular abnormalities (IRMA) on regular fundus exams. FA can make these findings more prominent and thus more precisely pinpoint the patient’s stage of retinopathy.
FA findings are also used to determine efficacy of treatment for the condition. Because diabetic retinopathy has a propensity to impact the peripheral retina, wide-field fluorescein angiography is the preferred modality. This enhances the appreciation of capillary nonperfusion of the peripheral retina and can most accurately map the extent.6
Age-related macular degeneration
FA is also a mainstay for monitoring exudative age-related macular degeneration(AMD) and, often, advanced stages of non-exudative AMD. According to experts, FA offers more than information to determine whether AMD is exudative or not; it also offers insight about the potential progression and can identify discreetly involved areas not detected on typical fundus exam.
In exudative AMD with classic CNVM, FA classically exhibits a subtle cloudy choroidal flush which progresses to a “lacy” appearance of leakage and later a “cloud” leakage throughout the remaining procedure. Occult CNVM is less defined and tends to manifest later in the FA. Sub-retinal hemorrhages from exudative AMD present as dense hypofluorescence over which retinal blood vessels filled with fluorescein can still be observed.
The FA findings play a large role in determining prognosis for AMD patients and in choosing an appropriate treatment plan with a retina specialist.7
Hypertensive/ischemic retinal pathology
Ischemic and hypertensive retinal conditions, such as vascular occlusions, also require FA information to aid in diagnosis and treatment. FA of a branch retinal vein occlusion (BRVO) or hemiretinal vein occlusion (HRVO) would outline the involved area and could be used to monitor the condition and any resulting macular edema.
In a patient with central retinal vein occlusion (CRVO), FA results are used to determine the extent of damage and if it is of the ischemic or nonischemic variety; greater than 10-disc diameters of capillary non-perfusion is considered ischemic and associated with a worse prognosis.
There is often a delay in transit time of the fluorescein dye on eyes with CRVO. Similarly, to diabetic retinopathy, wide-angle imaging with FA is the preferred modality, since it is better able to better map the extent of perfusion, or lack thereof.8
Coding:
The procedure code for FA is 92235, for ICGA 92240 and for concurrent FA/ICGA (also referred to as “interweaved”) it is 92242. For FAF the fundus photography code can be used 92250. The “bilateral” modifier should be selected if both eyes are tested (or the respective eye’s modifier if it is being performed unilaterally).
As an optometrist, you may or may not be injecting the dye yourself, based on the scope of your license. A retina specialist is usually responsible for the final interpretation of the angiogram, but understanding the procedure and interpretation will immensely improve your capability to provide collaborative care.
