Introduction: What is age-related macular degeneration?
Age-related macular degeneration (AMD) is an acquired, degenerative disease of the retina that causes progressive changes to the macula, resulting in a loss of central vision. It is characterized by distinct clinical stages, including the “dry” or atrophic form and the “wet” or exudative form.
In the dry form, loss of photoreceptors and retinal pigment epithelium (RPE) results in retinal tissue atrophy called
geographic atrophy (GA). In wet AMD, choroidal neovascularization (CNV) develops in the macula, which can also result in GA in the later stages of the disease.
Prevalence of AMD
AMD is a leading cause of severe, irreversible vision loss in adults over age 50, both in the United States and worldwide. Globally, it is estimated that approximately 200 million people have been diagnosed with AMD.1,2
Of the worldwide population, approximately 1 to 3% suffer from some form of
advanced AMD, with 5 million alone having GA. Of those 5 million, 1.5 million are in the United States.
1,2 GA has an estimated new case rate of 0.19% annually in people over the age of 50.
1With advancing age, the chances of getting GA increase, with approximately 1 in 29 patients over age 75 having GA and 1 in 4 patients over age 90 having the disease.3 This translates into an annual incidence of 2.2% in those over 90 years of age.
Classification of AMD
AMD classification by the Beckman Initiative for Macular Research Classification Committee is as follows:
- No disease: No pigmentary abnormalities are observed, and no or only a few drupelets (≤63µm drusen) are detected
- Normal Aging: Only small drusen (<63µm) are present; no AMD pigmentary abnormalities are present
- Early AMD: No pigmentary changes are present; drusen are between 63µm and 125µm in size.
- Intermediate AMD: Large drusen >125µm and/or any AMD pigmentary abnormalities are present
- Advanced: Neovascular AMD (wet) and/or geographic atrophy (dry)
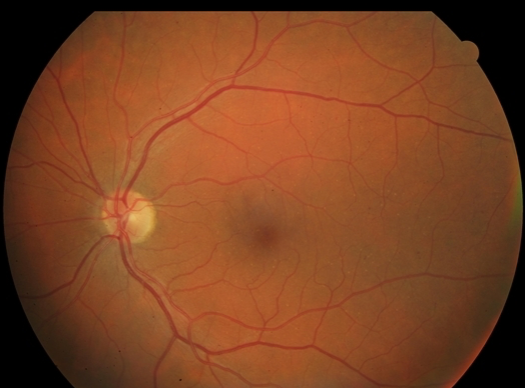
Figure 1 shows fundus photography of a patient with no signs of age-related macular degeneration.
Figure 1: Courtesy of Julie Rodman OD, MSc, FAAO.
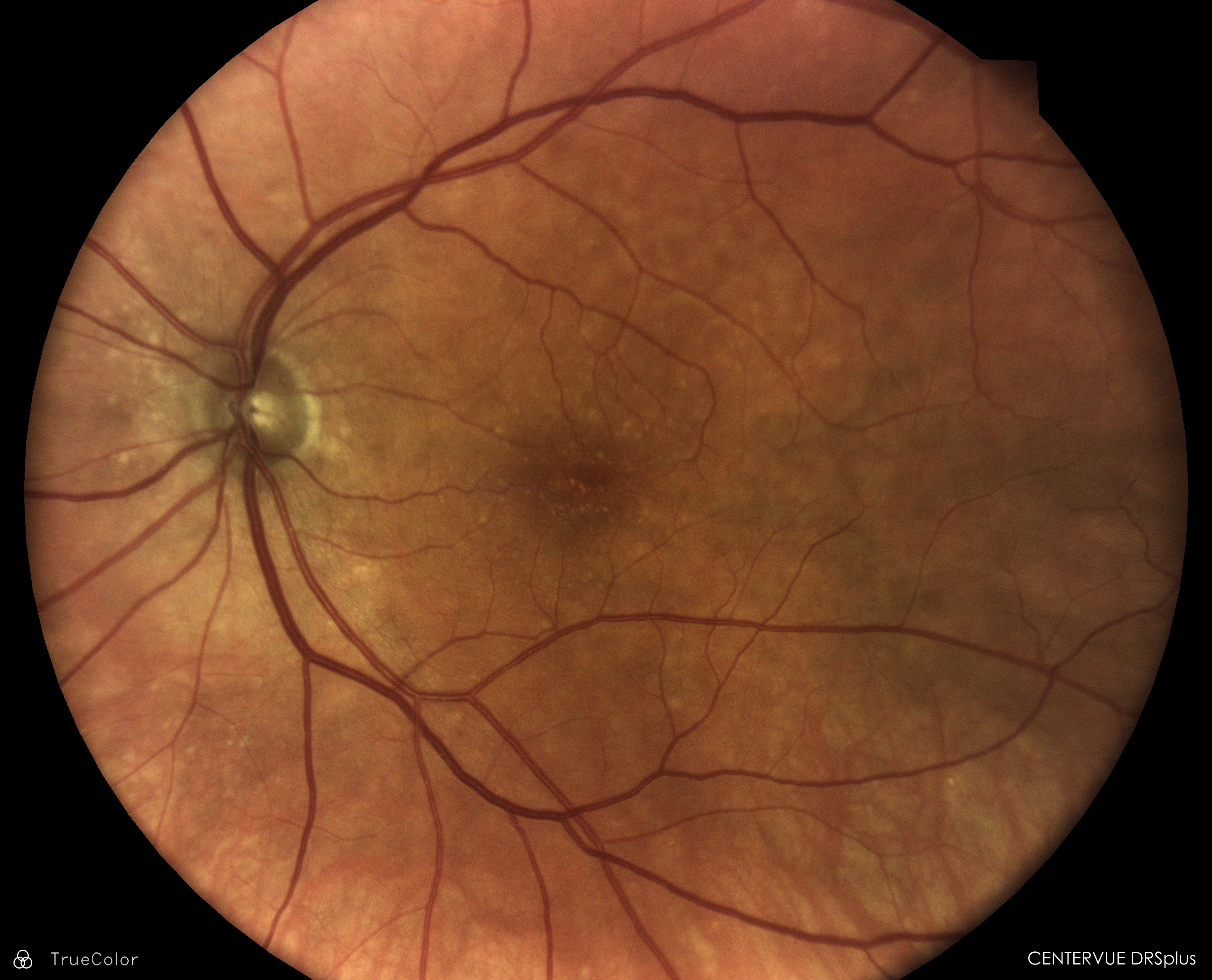
Figure 2 features fundus photography of a patient with early AMD; no pigmentary changes are present, and drusen are between 63µm and 125µm in size.
Figure 2: Courtesy of Julie Rodman OD, MSc, FAAO.
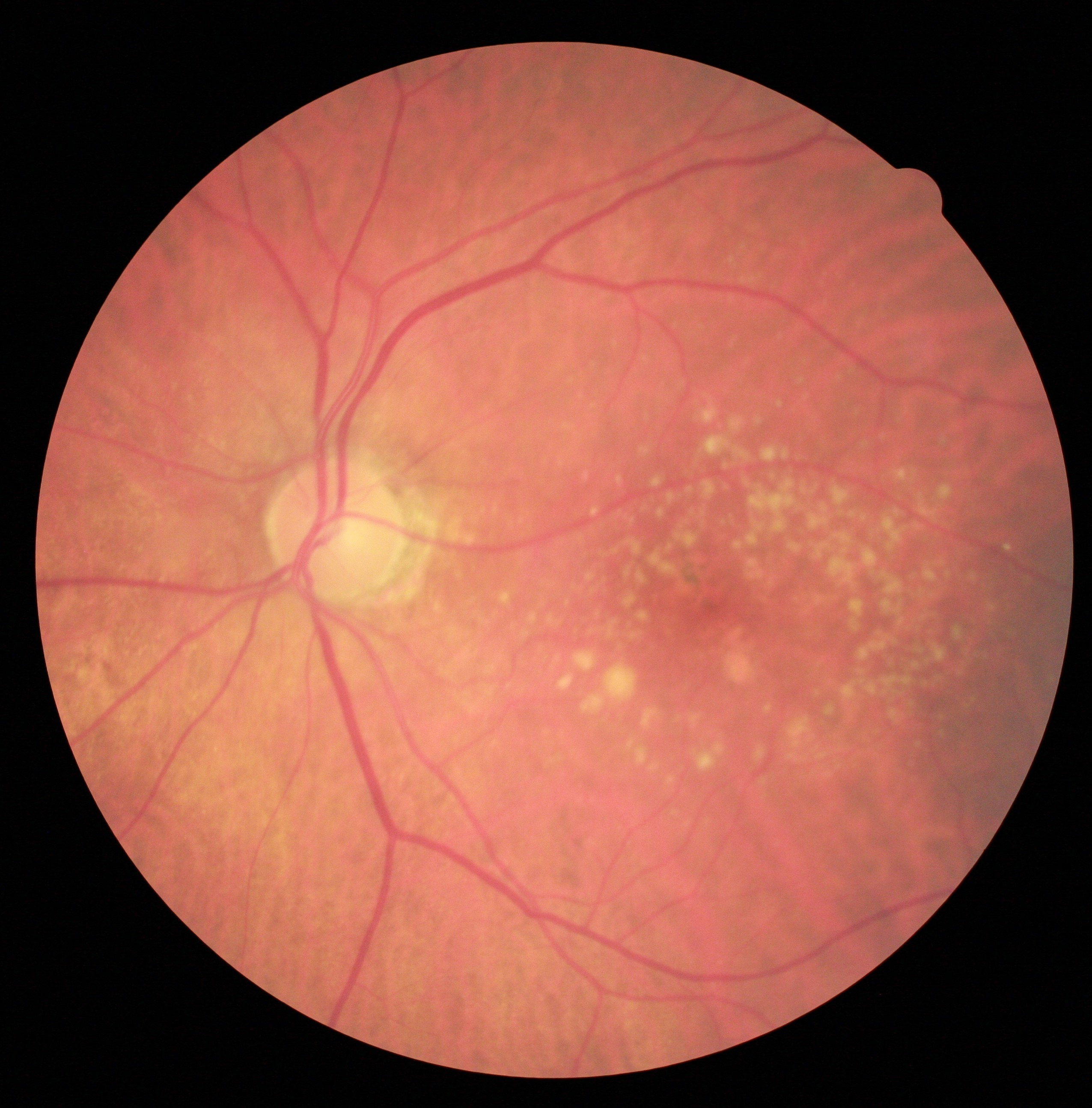
Figure 3 highlights fundus photography of a patient with intermediate AMD; large drusen >125µm and/or any AMD pigmentary abnormalities are present.
Figure 3: Courtesy of Julie Rodman OD, MSc, FAAO.
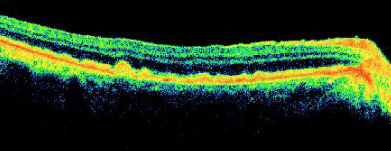
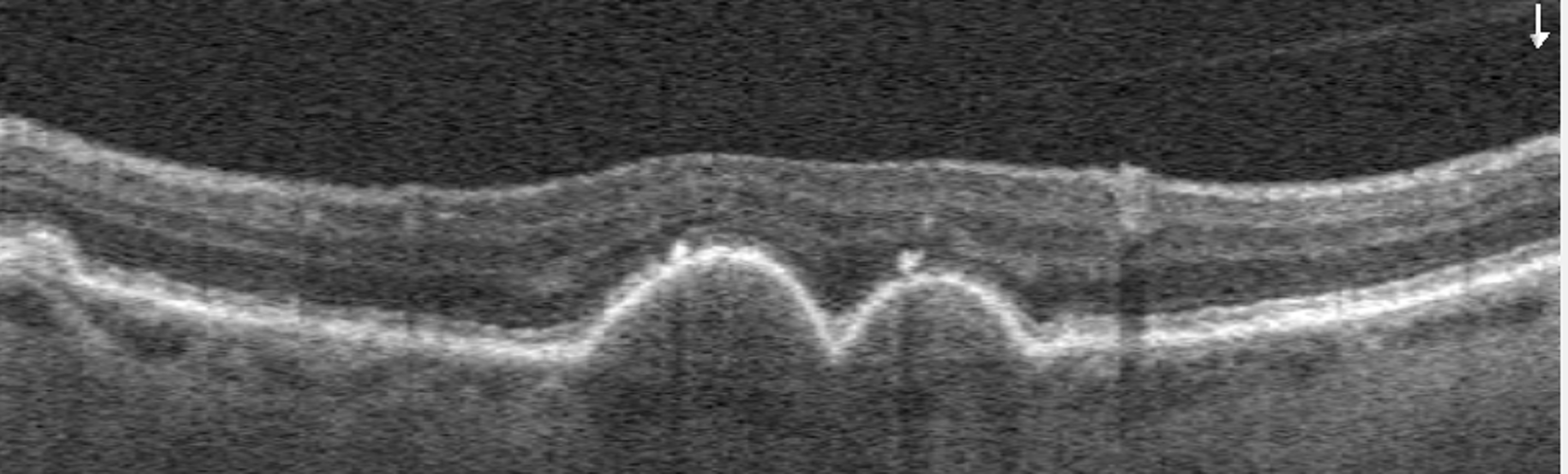
Figure 4 shows spectral domain optical coherence tomography (SD-OCT) illustrating medium-sized soft drusen.
Figure 4: Courtesy of Visionix.
Figure 5 depicts fundus photography of a patient with intermediate AMD; large drusen >125 microns and/or any AMD pigmentary abnormalities are present.
Figure 5: Courtesy of Julie Rodman OD, MSc, FAAO.
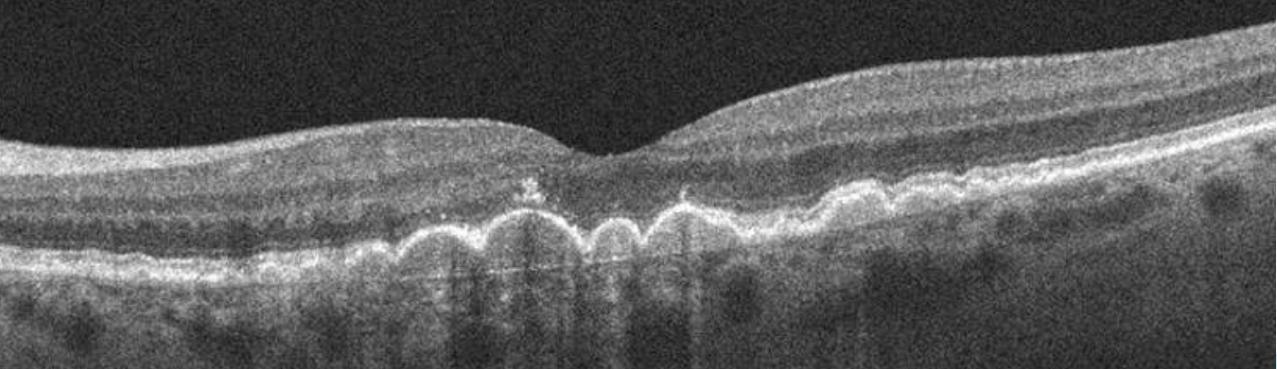
Figure 6 demonstrates SD-OCT imaging illustrating large drusen with small hyper-reflective foci suggestive of RPE pigmentary changes.
Figure 6: Courtesy of Julie Rodman OD, MSc, FAAO.
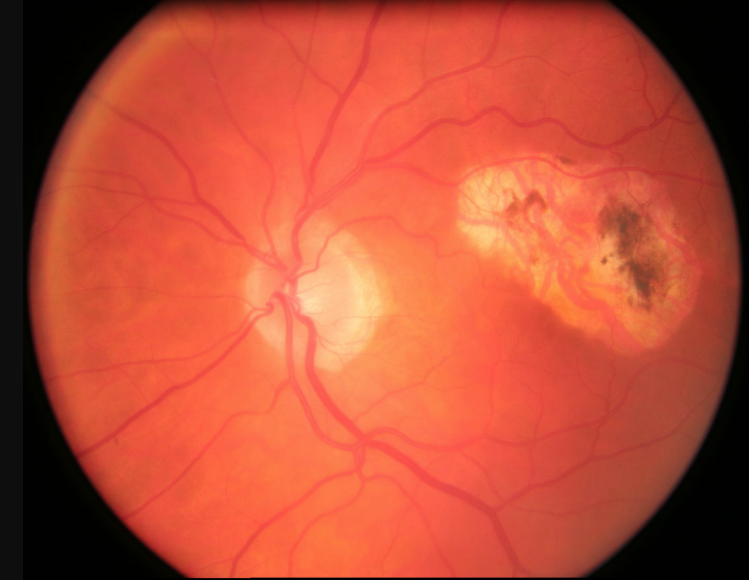
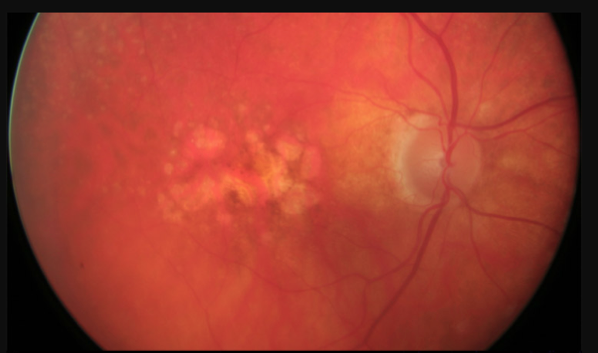
Figure 7 exhibits fundus photography of a patient with advanced AMD, and choroidal neovascular membrane (CNVM) can be observed.
Figure 7: Courtesy of Julie Rodman OD, MSc, FAAO.
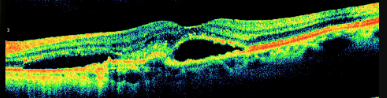
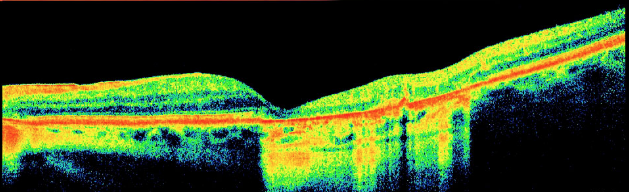
Figure 8 presents SD-OCT imaging illustrating choroidal neovascular membrane with adjacent subretinal fluid.
Figure 8: Courtesy of Visionix.
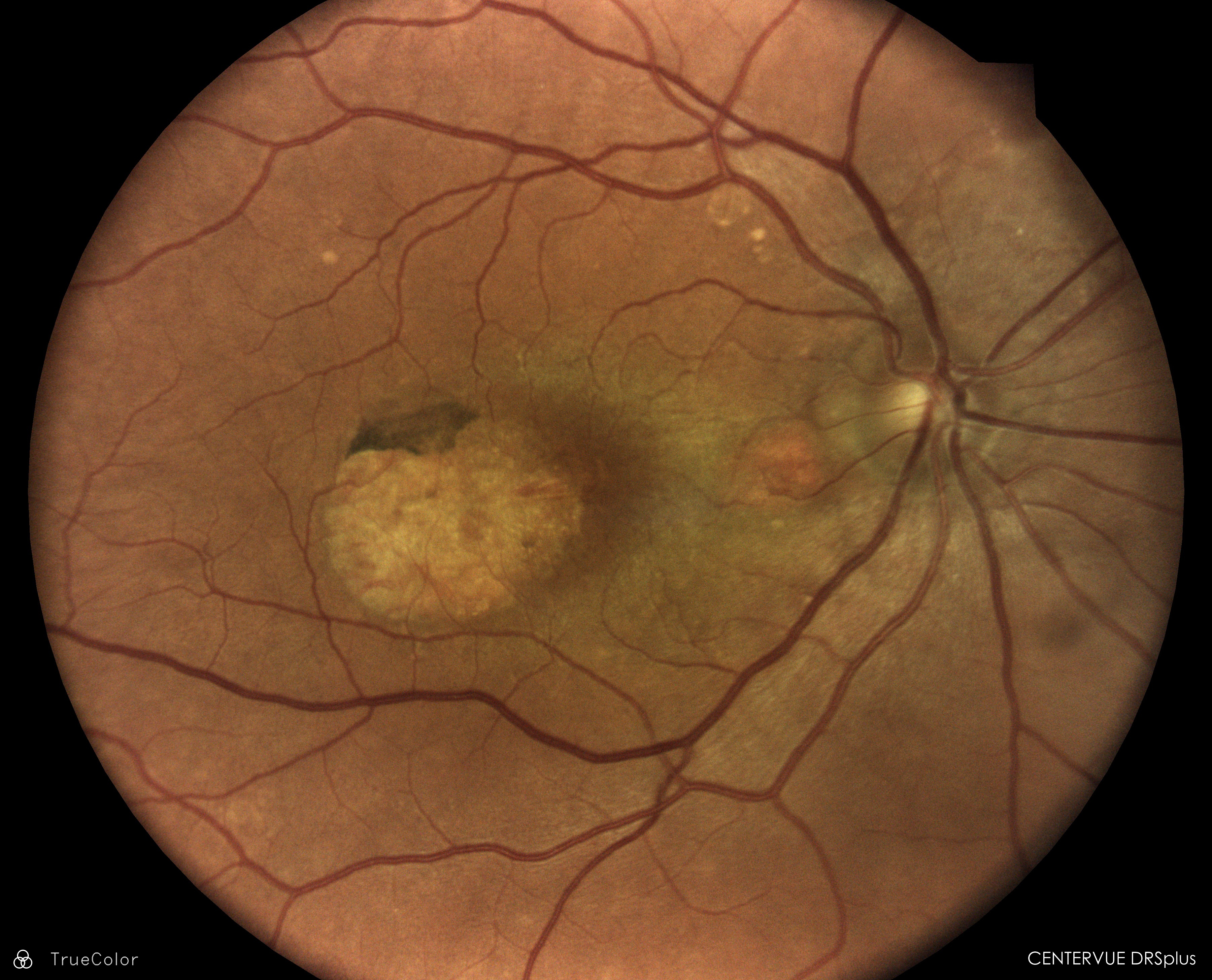
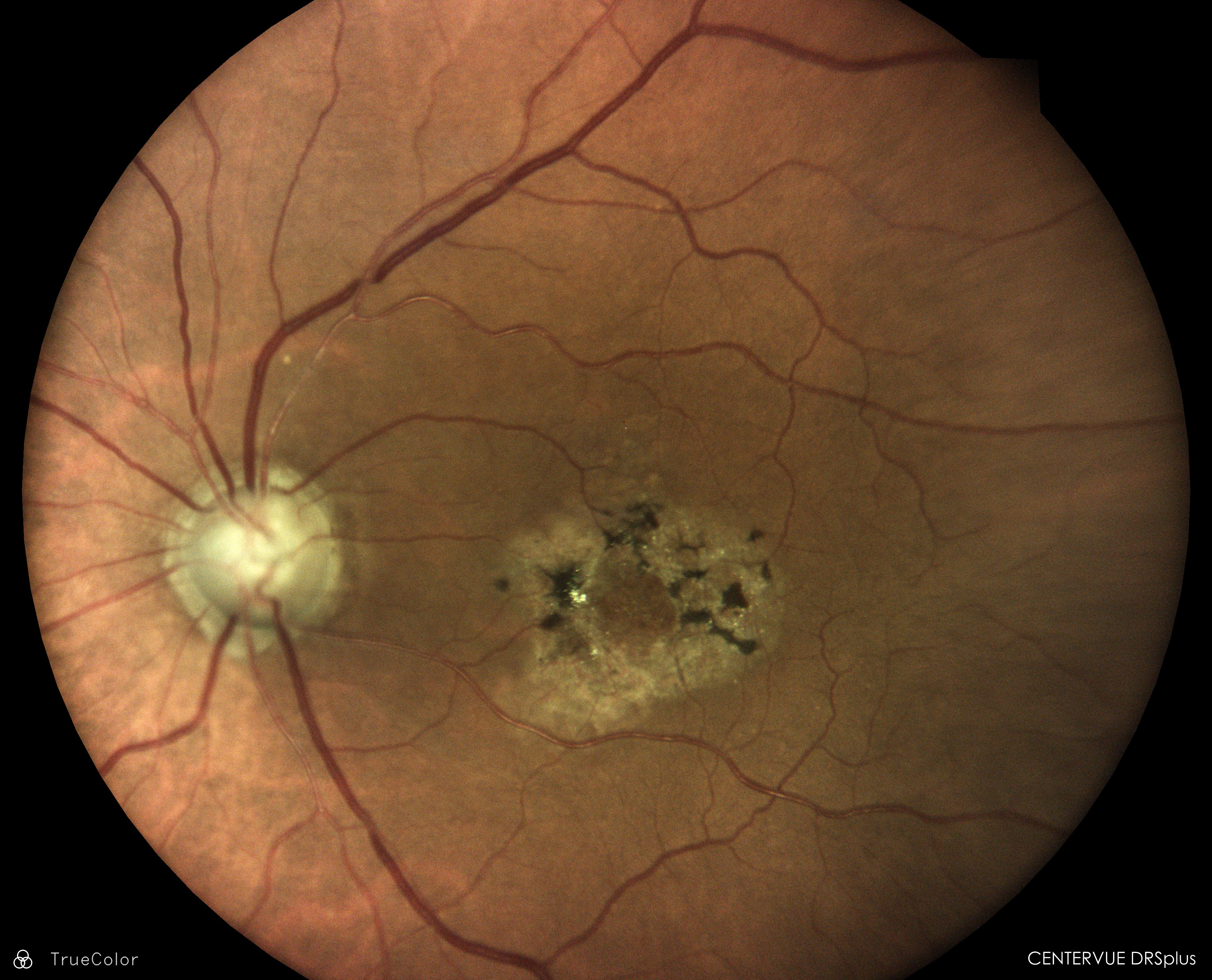
Figure 9 shows fundus photography of a patient with advanced AMD; geographic atrophy bordering the fovea can be observed.
Figure 9: Courtesy of Visionix.
Figure 10 features SD-OCT imaging of geographic atrophy.
Figure 10: Courtesy of Julie Rodman OD, MSc, FAAO.
Figure 11 highlights fundus photography of a patient with advanced AMD; geographic atrophy involving the fovea can be observed.
Figure 11: Courtesy of Julie Rodman OD, MSc, FAAO.
Pathophysiology of dry AMD
Dry age-related macular degeneration arises from structural abnormalities in the RPE, resulting in drusen formation in and around the macula.
5 Intermediate and large drusen play a large role in the pathogenesis of AMD. Aging and environmental stress lead to progressive damage to the retina triggering inflammation via multiple pathways, including the complement cascade.
The complement cascade is the body’s immune response to recognize and remove pathogens. Compromise of these pathways results in chronic inflammation and retinal cell death leading to GA.6 There are three pathways involved in the complement cascade, including classical, lectin, and alternative, which form a protein complex, C3 Convertase.
These different pathways converge with the cleavage of complement factor C3 into C3a and C3b, which cause inflammation and label cells for phagocytosis. In a pathogenic environment, the complement cascade thrives, leading to the cleavage of complement factor C5 resulting in cell death.6
What is geographic atrophy?
Geographic atrophy is the advanced form of dry AMD and is characterized by the presence of retinal atrophy that arises as a result of progressive and irreversible loss of the photoreceptors, retinal pigment epithelium, and choriocapillaris.
7,8 Clinically,
geographic atrophy is seen as well-delineated round or oval areas of hypopigmentation, allowing for increased visibility of the choroidal vessels.
9,10 Atrophic lesions typically appear perifoveally with eventual center foveal involvement.
Typically, foci of GA manifest initially in the parafoveal region, sparing the fovea.7 With time, these foci coalesce and expand into the fovea. It is hypothesized that foveal involvement occurs later in the disease due to unique features of the fovea, including increased macular pigment, increased choroidal blood flow, and higher concentration of cone density.11
Risk factors for age-related macular degeneration
AMD is a chronic multifactorial eye disease, and numerous risk factors have been identified in association with AMD. These risk factors can be delineated as “modifiable,” or those that we can control, and “non-modifiable,” or those that we cannot control.
Non-modifiable risk factors for AMD:
- Age: AMD becomes increasingly prevalent with advancing age. Individuals 75 years of age and older have a threefold increased risk of developing AMD.12 With GA specifically, 3.5% of people aged >75 years and 22% of people aged >90 years are afflicted.12
- Race and ethnicity: Those of European ancestry have the highest risk of AMD, followed by Chinese and Hispanic/Latino people, with the least at risk being those of African descent. Similarly, the population more likely to go blind from AMD would be those of European descent compared to those of African ancestry.2
- Family history: Studies have shown a link between late AMD and family history.13
- Genetics: Certain genetic loci have been linked to the development and progression of AMD and include Complement Factor H (CFH) and the ARMS2 gene. ABCA1 has been shown to be associated with a decreased risk of progression from normal to intermediate drusen and from intermediate to large drusen.
- Female gender
- Hyperopia
Modifiable risk factors for AMD:
- Cigarette smoking: Current smokers have a four-fold higher risk of late AMD when compared to those that have never smoked, with past smokers having a 3-fold higher risk of GA.14 Cigarettes contain toxins that contribute to cellular oxidative stress reducing the number of antioxidants.2
- Poor nutritional intake
- High blood pressure and hypercholesterolemia
- Cardiovascular Disease
- Obesity
Busting AMD myths
FALSE
Although a family history of AMD increases the risk of developing AMD, other lifestyle and systemic factors play a large role. All patients (regardless of family history) should be advised to exercise, avoid smoking, maintain healthy blood pressure and cholesterol levels, and eat a well-balanced diet.
2. “If I am diagnosed with AMD, I will go blind!”
FALSE
Early detection can play a large role in the trajectory of the disease. Yearly dilated eye examinations can identify “age-related” changes, which will allow for proper education and management. Patients may experience blurry vision or other functional vision loss without ever going blind.
Early detection of GA
AMD is a disease spectrum ranging from early to late stages.
8,9 Fortunately, the early signs of the disease can be identified through dilated fundus examinations alongside ancillary testing such as OCT, color fundus photography (CFP), near-IR reflectance (NIR), and
fundus autofluorescence (FAF).
The clinical hallmark of the disease is the presence of drusen, which leads to progressive degeneration of photoreceptors and RPE and results in loss of central vision.9 Identifying drusen and/or pigmentary changes as early as possible can ultimately change the course of the disease.
In fact, early AMD and signs of retinal changes are seen in individuals aged <45 years old.15,16 Eye examinations should be performed before patients exhibit loss of vision or large atrophic retinal involvement. Early detection and prompt attention improve the visual outcome.
Management options for early age-related findings include observation,
antioxidant, vitamin, and mineral supplements, encouragement of smoking cessation, maximizing cardiovascular health, and education on other risk factors when applicable. All patients should be educated about the prognosis of the disease and how proper behaviors can alter their visual and functional status.
Status of the fellow eye for AMD
The presence of GA in one eye is a strong prognostic indicator of the development of GA in the other eye, with an estimated involvement time of 7 years.11 GA also progresses at a faster rate when the fellow eye has GA.
Eyes with
bilateral GA or an eye with GA in one eye and CNV in the fellow eye have a significant risk of developing CNV alongside the GA.
13,17 Progression to advanced AMD in eyes with early or intermediate AMD is increased when there is GA or CNV in the fellow eye.
Figure 12 features fundus photography of a patient with geographic atrophy with CNVM.
Figure 12: Courtesy of Julie Rodman OD, MSc, FAAO.
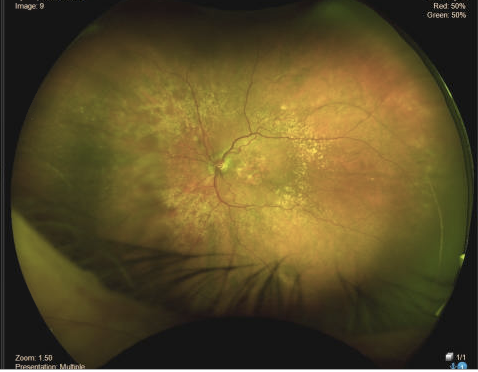
Figure 13 highlights geographic atrophy with diffuse retinal drusen.
Figure 13: Courtesy of Julie Rodman OD, MSc, FAAO.
Geographic atrophy: What we know about progression
Not all GA is created equal! Identifying which lesions are more susceptible to rapid growth is critical in proper management of this disease. The rate of lesion progression in GA patients ranges from 0.53mm2 to 2.6mm2 per year (median 1.78mm2).9 Specific characteristics have been shown to directly correlate with disease progression.
- GA lesion size: GA lesions that are large at baseline have a higher rate of progression.9,18
- Number of GA lesions: Multifocal lesions have increased rates of GA growth.9,18
- Shape: Irregularly shaped lesions grow more rapidly than circular lesions.18
- Location of the atrophy (foveal versus extrafoveal): GA can present with or without foveal involvement. Foveal involvement is believed to be a strong predictor of growth rate and progression. Extrafoveal lesions progress more rapidly than foveal lesions.9
- OCT and FAF findings
- Outer retinal tubulation (ORT): ORT is a distinct finding identified on OCT. ORT correlates with an area of damaged photoreceptors that take on a circular or tubular pattern. They have a characteristic outer ring of hyper-reflectivity with a central core of hypo-reflectivity on OCT. The presence of ORT is correlated with a more rapid rate of GA progression.19 Patients that have ORT and neovascular AMD are at higher risk of developing atrophy as well.
- Type of drusen: Reticular pseudodrusen or subretinal drusenoid deposits (SDD) reside in the subretinal space (versus regular drusen that exist between the RPE and Bruch’s membrane). These drusen have a “saw-tooth” appearance and resemble small triangular projections on OCT. Reticular pseudodrusen are highly linked to GA progression.
- Hyper-reflective foci: Hyper-reflective dots or round lesions within retinal layers on OCT. These foci are biomarkers for disease progression and prognosis, including macular atrophy.
Figure 14 exhibits OCT imaging of medium to large drusen with hyper-reflective foci.
Figure 14: Courtesy of Julie Rodman OD, MSc, FAAO.
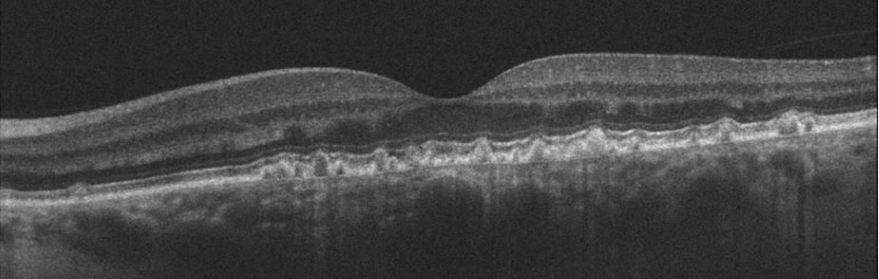
Figure 15 depicts OCT imaging of reticular pseudodrusen.
Figure 15: Courtesy of Julie Rodman OD, MSc, FAAO.
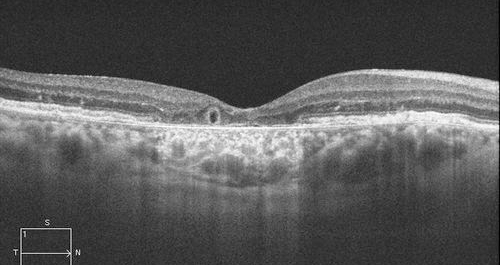
Figure 16 shows OCT imaging of outer retinal tubulation.
Figure 16: Courtesy of Julie Rodman OD, MSc, FAAO.
Features of geographic atrophy
There is a multitude of imaging modalities that optimize both the visualization of GA and assist in monitoring the disease state. The most commonly used imaging modalities in clinical practice include OCT, FAF, near-IR reflectance imaging, and color fundus photography. The role of other imaging modalities, such as
optical coherence tomography angiography (OCTA), is being investigated.
9Color fundus photography
GA lesions will appear as sharply demarcated hypopigmented unifocal or multifocal areas on clinical examination and on
fundus photography. Increased visualization of the underlying choroidal blood vessels due to the absence of RPE and choriocapillaris will be apparent.
CFP often highlights subtle pathology seen in the early stages of the disease that may be easily overlooked on fundus examination. Despite the excellent resolution of fundus photography, CFP often cannot capture some of the findings associated with GA progression.
Near-IR reflectance imaging
NIR is a non-invasive imaging modality used to visualize changes in the subretinal space, including the photoreceptors, RPE, and choroid. Most images are obtained simultaneously with
SD-OCT.
20 Long excitation wavelength (~820nm diode laser) penetrates the optic media allowing for excellent visualization of the RPE and choroid.
Abnormalities on NIR imaging can be classified as hyper-reflective or hypo-reflective. Drusen can range in reflectivity; small to medium are more likely to be hyper-reflective, while large may be hyper or hypo. Reticular pseudodrusen may exhibit a hyper-reflective central appearance, surrounded by a hypo-reflective shell. Geographic atrophy will appear hyper-reflective on NIR imaging.21 NIR is useful in identifying the boundaries of the lesion, where image contrast appears lower on FAF.22
Optical coherence tomography (OCT)
B-scan OCT imaging is commonly used by clinicians to assess GA. OCT will show loss of outer retinal layers corresponding to damage of the RPE and photoreceptors. However, there is a wide range and variability of anatomical changes findings on OCT.
Thus, the
Classification of Atrophy Meeting Group (CAM Group) created a rubric to provide uniformity when defining GA using OCT. OCT may play a role in the early identification of disease by highlighting structural markers associated with disease progression.
19 OCT is highly effective at identifying early signs of disease but may not be as useful as NIR or FAF in monitoring disease progression.
The CAM group created 4 terms to encompass the various OCT findings seen in GA, as seen below with example OCT images.
1. Complete RPE and outer retinal atrophy (cRORA)
- Loss of outer retinal layers
- RPE loss
- Choroidal hypertransmission of at least 250μm
- Choroidal hypertransmission (increased signal penetration into the choroid) occurs as a result of the atrophy or attenuation of the overlying sensory retina and RPE19
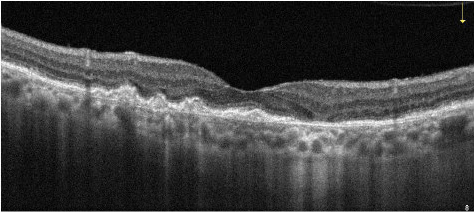
Figure 17 is OCT imaging of cRORA with loss of outer retinal layers, RPE loss, and choroidal hypertransmission of at least 250μm.
Figure 17: Courtesy of Julie Rodman OD, MSc, FAAO.
2. Incomplete RPE and outer retinal atrophy (iRORA)
- Earlier stage of atrophy
- Patchy loss of the RPE (less than 250μm)
- Choroidal hypertransmission (less than 250μm)23,24
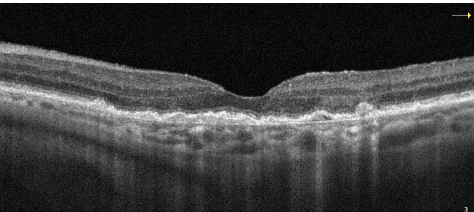
Figure 18 is OCT imaging of iRORA with patchy loss of the RPE and choroidal hypertransmission less than 250μm.
Figure 18: Courtesy of Julie Rodman OD, MSc, FAAO.
3. Complete outer retinal atrophy (cORA)
- Continuous non-visibility of the ellipsoid zone and interdigitation zone
- Severe thinning of the outer retina
- Intact RPE band
- Choroidal hypertransmission is intermittent18
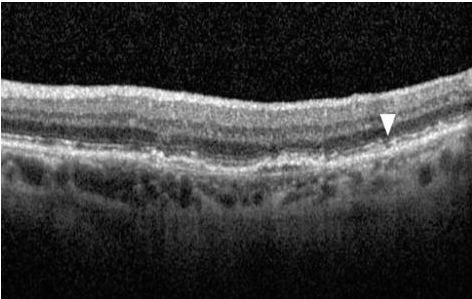
Figure 19 is OCT imaging of cORA, with loss of ellipsoid zone, intact RPE, and patchy hypertransmission.
Figure 19: Courtesy of Julie Rodman OD, MSc, FAAO.
4. Incomplete outer retinal atrophy (iORA)
- Continuous external limiting membrane (ELM)
- Detectable ellipsoid zone disruption
- Thinning of outer retina
- Intact RPE band
- No hypertransmission defects
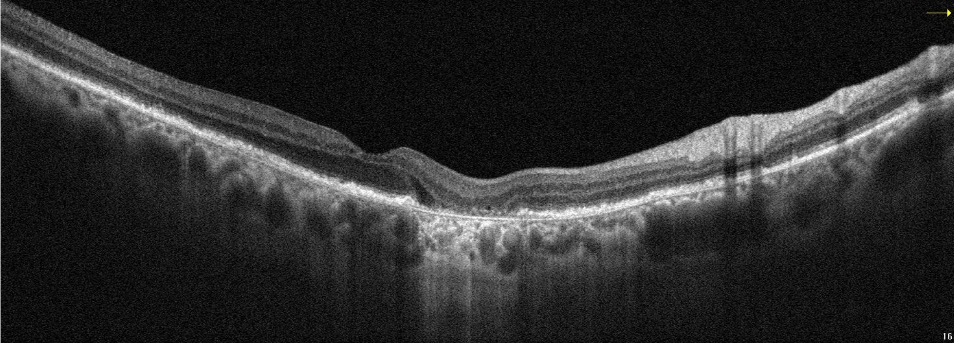
Figure 20 is OCT imaging of iORA with incomplete RPE and outer retinal atrophy.
Figure 20: Courtesy of Julie Rodman OD, MSc, FAAO.
Fundus autofluorescence
FAF is a non-invasive tool that uses the naturally occurring fluorescence of the retina to assess the health and integrity of the RPE. It may often detect abnormalities not seen on fundus examination. On short-wavelength FAF, GA lesions will manifest as sharply demarcated areas of hypoautofluorescence due to a smaller concentration of fluorophores as a result of RPE cell death.
The variability in intensity and presentation of the lesion (assessing the borders or junctional zones around the lesions) provides information about the progression of the GA. FAF is optimal at identifying lesion borders and assessing for progression. The
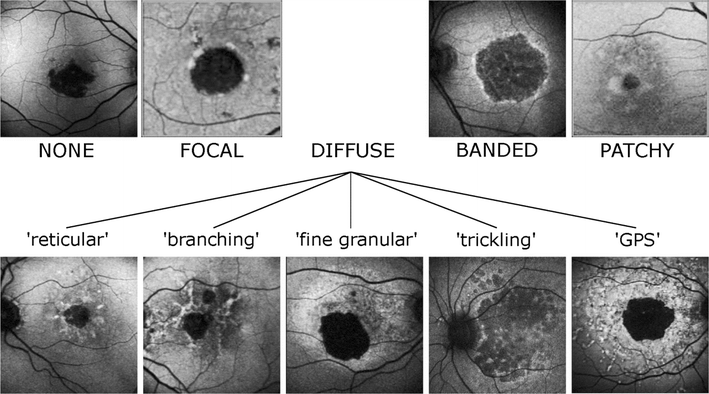
Fundus Autofluorescence in Age-Related Macular Degeneration (FAM) study group identified five different patterns of hyperfluorescence surrounding the GA.
22,25FAF Patterns (seen in the junctional zone of GA)
- None
- Focal: Evidence of one or more small spots of elevated FAF at the edge of the lesion
- Patchy: Lesions show some FAF spots outside the GA lesion area with spread toward the posterior pole
- Banded*: Increased autofluorescence is characterized by a continuous stippled band of increased FAF surrounding the entire atrophic area.
- *Banded and diffuse trickling has been associated with a high risk for disease progression.
- Diffuse*†: Reticular, branching, fine-granular with peripheral punctate spots, or diffuse trickling
- *Banded and diffuse trickling has been associated with a high risk for disease progression.
- †Diffuse trickling—lesions demonstrate gray (rather than black) hypoautofluorescence and lobular atrophic patches with high intensity at the margins.
Assessing the pattern of fluorescence and
lesion boundaries may be more challenging in certain patterns (such as diffuse trickling); these scenarios would be optimally visualized using both FAF and NIR imaging. NIR is not as affected by macular pigment, thus enhancing the image contrast.
22,25Figure 21 features images of perilesional phenotypic FAF patterns that can be used to classify geographic atrophy.
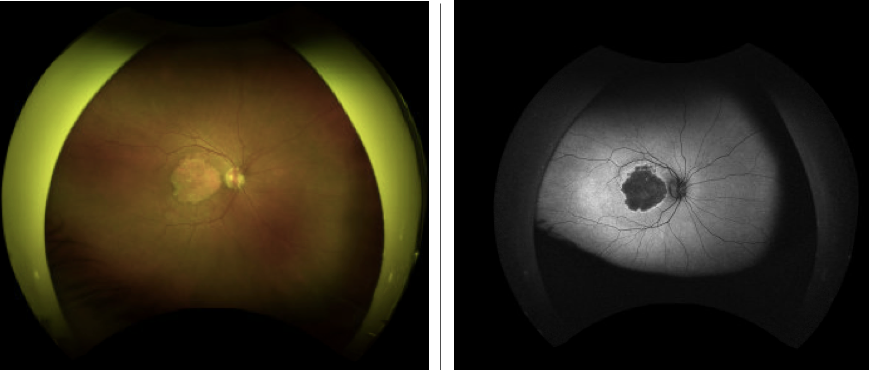
Figure 22 shows color fundus photography of geographic atrophy on the left and fundus autofluorescence illustrating a banded pattern on the right.
Figure 22: Courtesy of Julie Rodman OD, MSc, FAAO.
Busting geographic atrophy myths
1. “Multimodal imaging can not detect early changes.”
FALSE
OCT, FAF, CFP, and NIR are our best friends when it comes to diagnosis and early detection. These modalities provide outstanding visualization of findings that may be very subtle on fundoscopy and are oftentimes overlooked on exams. It is crucial that optometrists are familiar with these modalities and how to interpret the findings to identify those at risk for progression.
2. “All GA patients will experience visual loss; no one is spared from progression.”
FALSE
Early detection via yearly eye examinations and multi-modal imaging will help identify early clinical signs of the disease. This will change the dialogue between physician and patient with the goal of modifying behaviors/environmental factors to alter the course of the disease. Not all patients with AMD will progress.
3. “There are no treatments available or on the horizon for GA.”
FALSE
Pegcetacoplan injection (Syfovre) is the first FDA-approved intravitreal injection indicated for the treatment of GA secondary to AMD. Additionally, avacincaptad pegol is an intravitreal injection therapy that is currently under investigation for the treatment of GA. With these promising new agents coupled with proactive earlier detection, these novel treatments may stop or slow progression and give hope to patients who might be suffering from this disease.
What is the link between GA and visual function?
GA can lead to a significant decline in visual function and a negative effect on one’s quality of life. Although best-corrected visual acuity may be preserved in patients with “foveal sparing” GA, patients typically experience visual impairments such as difficulty with everyday tasks.
GA affects a patient’s ability to perform social activities such as recognizing a friend’s face, driving, and reading. Patients will have decreased mobility and driving ability and often report a feeling of social isolation.
Tests such as Snellen visual acuity may not provide an accurate assessment of a patient’s visual function, particularly in patients with foveal sparing. Other tests are more efficacious in identifying functional
vision loss.
Evaluating visual function in patients with geographic atrophy
Microperimetry measures threshold light sensitivity at various points across the macula. This is achieved by modifying the stimulus intensity. Looking at the microperimetry map in tandem with CFP can provide a means of assessing structure and function simultaneously.
Additionally, the
low luminance visual acuity (LLVA) test is another effective functional vision assessment. This test requires a patient to read an ETDRS chart under normal lighting through a 2.0-log unit neutral density filter. Baseline low luminance deficits are directly correlated with subsequent vision loss for all levels of VA in geographic atrophy.
12 Low luminance testing is also useful in identifying patients at the highest risk for VA loss.
Evaluating a patient’s reading speed is another effective measure of functional vision in GA patients. Patients with extrafoveal lesions may experience difficulty with continuous text and thus display a reduction in reading speed. This is often missed by testing a single letter on the ETDRS chart.
Figure 23 depicts fundus photography of a patient with geographic atrophy sparing the fovea.
Figure 23: Courtesy of Julie Rodman OD, MSc, FAAO.
Treatments for geographic atrophy
In 2023, two treatments to slow the progression of geographic atrophy were approved by the FDA and are now commercially available in the United States after multiple studies investigating the drugs' efficacy and safety. Both medications were well-tolerated with favorable safety profiles.27,29
Syfovre (pegcetacoplan injection, Apellis Pharmaceuticals, Waltham, MA) 15mg/0.1 mL, a complement C3 inhibitor, was approved in February 2023. Syfovre is an intravitreal injection that is administered every 25 to 60 days and indicated for the treatment of GA secondary to AMD.
27,28,29 Izervay (avacincaptad pegol intravitreal injection, An Astellas Company, Northbrook, IL) 2mg, a complement C5 inhibitor, was approved in August 2023. Izervay is an intravitreal injection that is administered monthly and indicated for the treatment of GA secondary to AMD.
30 Note: This article was originally published June 7, 2023. It has been updated as of February 9, 2024 to reflect the FDA approval status of both avacincaptad pegol and pegcetacoplan.