


Patient case report: geographic atrophy
Mrs. Jones comes into your office. She’s the sweetest 80-year-old woman. She’s 20/150 in the right eye and 20/400 in the left eye. Her youngest daughter Monica recently gave birth to the cutest baby boy ever. When someone asks Mrs. Jones who he looks like, she’s at a bit of a loss.
She reports that the baby’s face is always a blur. Mrs. Jones also mentions that she cannot sign any of her checks or pay her bills anymore and has been unable to read the news scroll that runs along the bottom of the television for quite some time now. She’s extremely saddened by her very poor vision.
You take a look under the slit lamp with a 90 Diopter lens. Even before taking a look, you unfortunately already know the diagnosis just based on her symptoms and age.
Mrs. Jones is 80 years old, but patients with geographic atrophy (GA) from advanced age-related macular degeneration (AMD) can present much earlier. Mrs. Jones, like many of our AMD patients, is otherwise in pretty good health for her age. Her cardiologist thinks she’ll live to 105 years old, like her elder sister Mrs. Murphy.
Patient case report takeaways
You sit back and think to yourself: If only I could prevent this from progressing further. If only I could have prevented progression 30 years ago. As eye doctors, our goal is to preserve our patients’ vision and functionality and allow them to live their best lives. There is nothing more precious than our patients’ eyesight.
Fortunately for our patients, technology and medical breakthroughs are progressing at a faster rate than ever, and it appears that help is around the corner.
The stages of age-related macular degeneration
Our current classifications and our current treatment guidelines arise largely from important studies, namely the AREDS and AREDS2 studies.1,2 These studies allow us to group AMD into different stages ranging from early to intermediate to advanced. Advanced or late-stage AMD can then be further divided into advanced nonexudative or dry AMD (geographic atrophy) and advanced exudative or wet AMD.
Overall, dry AMD is responsible for 90% of diagnosed cases of AMD.3 Whereas at the advanced stages, dry AMD/GA accounts for 45%, and wet AMD accounts for 55%.4 These two forms can often coexist as well, with some eyes having features of each.
Early AMD is characterized by drusen and pigmentary abnormalities. These early changes are usually asymptomatic for the patient and can be detected by the doctor on examination using fundus photography (FP) and optical coherence tomography (OCT) imaging.
Figure 1 shows the role of oxidative stress and blood vessels in the progression of AMD.5

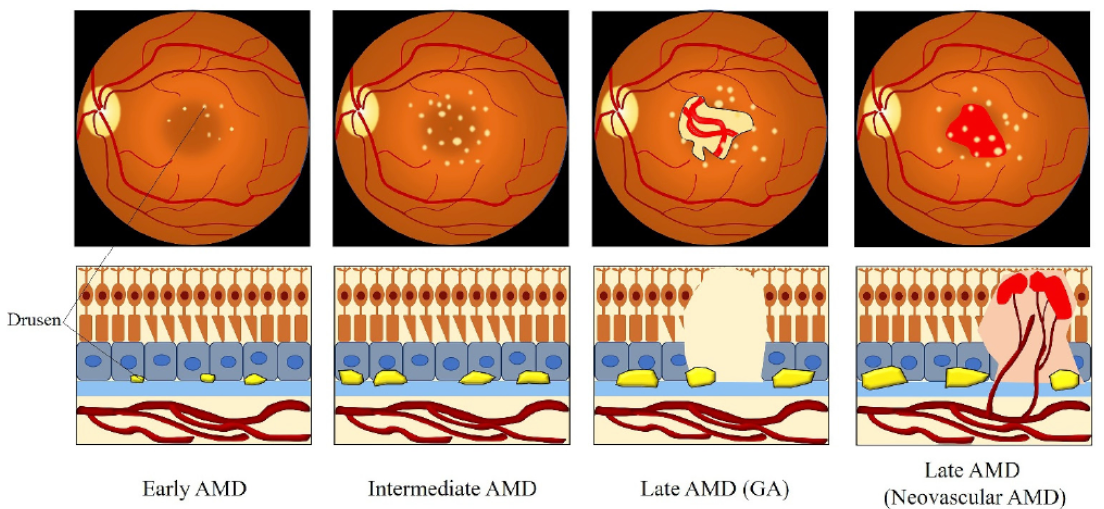
Figure 1: Courtesy of Ruan et al.
Conversely, patients with intermediate AMD are usually more symptomatic and start to have some distortion in the central vision. This stage is characterized by many medium-sized drusen, one large drusen, or GA not extending into the foveal center.1,6
Patients with early AMD, and especially those at later stages of AMD, may start to show compromised reading ability, require brighter lighting, and have difficulty with contrast sensitivity and dark adaptation.4 I routinely ask patients about these symptoms and use these as subtle symptoms of progression in my advanced dry AMD patients.
Current treatments for wet AMD
For wet AMD, anti-vascular endothelial growth factor (VEGF) injections, such as Avastin (bevacizumab), Lucentis (ranibizumab), Eylea (aflibercept), and, more recently, combined anti-VEGF and anti-ang2 injection Vabysmo (faricimab), were groundbreaking therapies. Since their arrival, these treatments have since become the standard of care, with the ability to not only preserve vision in wet AMD but even reverse vision loss in many cases.
While the same revolution in treatment appears on the horizon for geographic atrophy, the current treatments involve mostly decreasing modifiable risk factors, such as smoking cessation, reduction of UV exposure through the use of sunglasses, weight loss, incorporating a diet high in dark green leafy vegetables, and supplements containing certain vitamins and antioxidants identified by the AREDS and AREDS2 studies.1,2
A closer look at the AREDS and AREDS2 studies
The AREDS study, published in 2001, studied over 4,000 patients and found that the estimated 5-year probability of progression from intermediate to advanced AMD was 28% for the placebo group and 20% for patients who took antioxidants plus zinc, resulting in a 25% risk reduction in progression.1,7
Figure 2 is a graphical representation of the results from the AREDS study.7

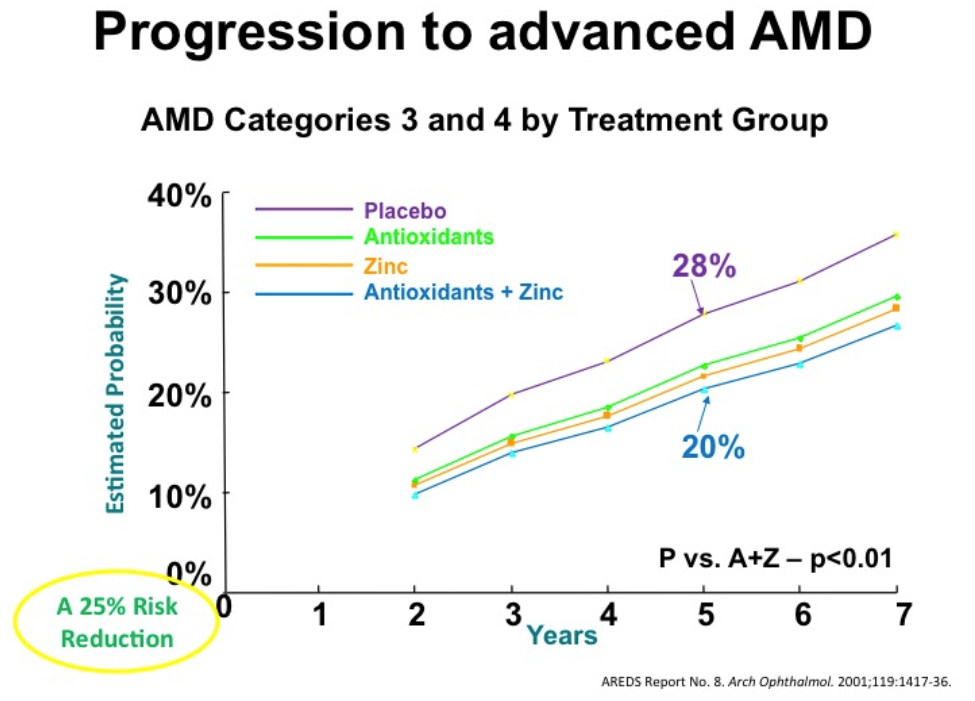
Figure 2: Courtesy of Dennis Ruskin, OD
The AREDS2 study, published in 2013, showed that replacing beta-carotene with lutein and zeaxanthin maintained the risk reduction in the progression of AMD.8 This revised formula included a combination of vitamin C 500mg, vitamin E 400 IU, copper 2mg, zinc 80mg, lutein 10mg, and zeaxanthin 2mg.2,7,8,9,10
As a side note, the original AREDS formula, which had included beta-carotene, was found to have an increased risk of lung cancer in smokers. This was not found to be the case in the newer formula without beta-carotene.8
While the data are significant, nonetheless, we know that this 25% risk reduction is not adequate enough to preserve all of our patients’ vision. Despite our best current efforts, the majority of patients continue to progress as they get older.
Table 1 represents findings from the AREDS and AREDS2 studies on the benefits of micronutrient supplementation for reducing the risk of wet age-related macular degeneration.11
| Nutrient | AREDS formula | AREDS2 formula |
|---|---|---|
| Vitamin C | 500mg | 500mg |
| Vitamin E | 400 IU | 400 IU |
| Beta-carotene | 15mg | - |
| Copper (cupric oxide) | 2mg | 2mg |
| Lutein | - | 10mg |
| Zeaxanthin | - | 2mg |
| Zinc | 80mg | 80mg |
Table 1: Courtesy of National Eye Institute
An overview of geographic atrophy
Geographic atrophy is considered to be the advanced form of dry macular degeneration, but GA can be seen at intermediate stages as well when the geographic atrophy has not yet involved the fovea.4,12
Clinically, on examination and with color fundus photography, GA can be seen as a hypopigmented area in the macula due to an absence of retinal pigment epithelium (RPE) cells and with clearly visible underlying choroidal vessels.12
How to identify geographic atrophy
Spectral-domain optical coherence tomography (SD-OCT) confirms that GA results from atrophy of the photoreceptors, RPE, and choriocapillaris. Additionally, light hyper-transmission through the retinal layers on OCT results from a lack of RPE results in an increase in choroidal reflectivity below Bruch’s membrane and can help identify areas of GA.12
On fundus autofluorescence (FAF), areas of GA appear hypo-autofluorescent. This is due to the loss of RPE cells and lipofuscin. FAF is an invaluable diagnostic tool that, in addition to SD-OCT and clinical examination, helps to monitor the subtle progression of geographic atrophy. Using a short wavelength, specifically a blue excitation wavelength of 488nm, is the modality accepted by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for clinical trials.4,12
On fluorescein angiography (FA), GA is identified by areas of early hyper-fluorescence and late staining. This is due to the fluorescein dye being taken up first by the choroidal vessels, which are clearly visible due to the lack of RPE cells, creating what is termed “a window defect.” The later phases of the FA show staining of the area, making the margins of GA hard to visualize.12
Figure 3 highlights different imaging technology showing features of geographic atrophy.12

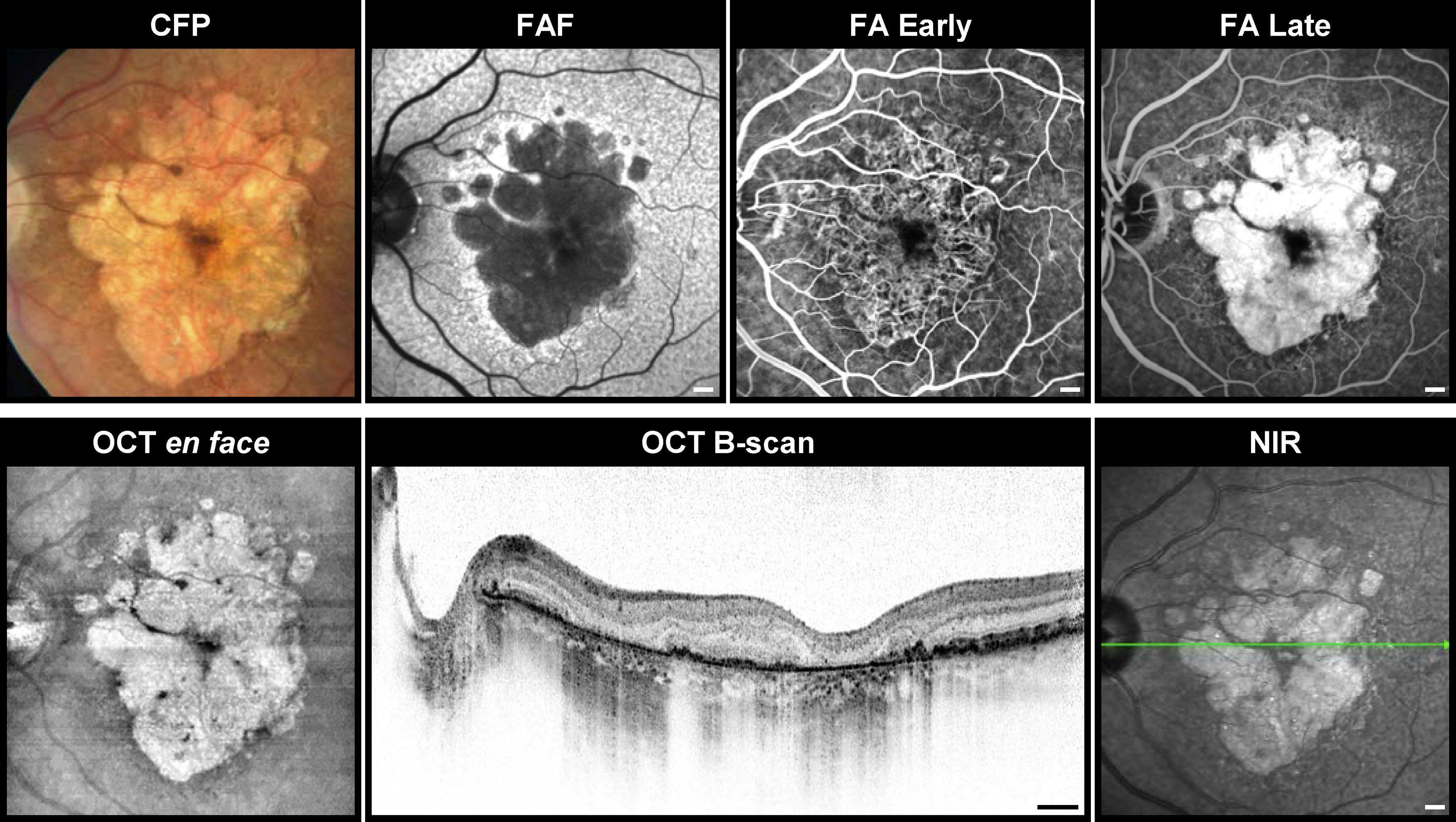
Figure 3: Courtesy of Fleckenstein et al.
Rates and risk factors for the progression of geographic atrophy
Geographic atrophy usually begins in the parafoveal region (non-central GA) and, over time, progresses to central GA. Rates of progression are highly variable in various studies. Most studies have reported overall GA lesion growth rates ranging from 0.53 to 2.6mm2/year.13
GA formation in one eye is highly suggestive that the patient will develop GA in the fellow eye, usually within 7 years.13 Contralateral eye status helps determine rates of progression in the other eye. For example, GA progresses fastest when the contralateral eye has GA, at an intermediate rate when the contralateral eye has choroidal neovascularization, and rates of progression of GA are slower when the contralateral eye has early or intermediate AMD.12,13
Of note, extra-foveal lesions progress faster than foveal lesions at a rate of 2.05 vs. 1.28 mm2/year, respectively. Extra-foveal GA also progresses 2.8-fold faster towards the periphery than it does towards the fovea.12
An eye may have one (unifocal) or multiple (multifocal, two or more) atrophic lesions, which, when summed, determine the total lesion area. It appears that multifocal GA progresses faster than unifocal GA, likely due to the greater total perimeter size of multifocal GA. The greater the perimeter or border, the greater the number of RPE cells exposed at the border, and thus the greater number of RPE cells at risk for progression to GA.14,15
Some studies have found that the rates of annual progression of GA are about 0.29 mm2/year overall. Rates were found to be faster in non-central or extra-foveal GA (0.31 mm2/year) compared to central GA (0.22 mm2/year), multifocal GA (0.36 mm2/year), and for current smokers (0.33 mm2/year) when compared to non-smokers (0.27 mm2/year).14 These findings support that multifocal GA, non-central or extra-foveal GA, and smoking are associated risk factors for progression.14
Using imaging technology to detect geographic atrophy
Certain OCT findings are also associated with a high risk for progression. The presence of reticular pseudodrusen or subretinal drusenoid deposits anterior to the RPE on OCT is strongly associated with progression to GA.12 OCT findings of nascent GA were shown to result in an 80-fold increased risk of developing GA.16 Nascent geographic atrophy can be identified by the subsidence of both the outer plexiform layer and inner nuclear layer and a wedge-shaped band within the outer plexiform layer.12,16
FAF remains the gold standard for detecting the growth of GA.13 The hypo-autofluorescent patches in areas of GA are surrounded by varying degrees of hyper-autofluorescence, particularly at junctional regions of atrophy.17 Overall, the greater the hyper-autofluorescence surrounding the area of atrophy, the worse the prognosis.12,17
Different patterns at the junctional zone in FAF have been identified, which can help identify which patients are at increased risk of progression. Patients with banded or diffuse patterns show greater progression of GA than patients with focal patterns or no pattern.12,17
Figure 4 features hallmark patterns in fundus autofluorescence and OCT for patients with geographic atrophy.12

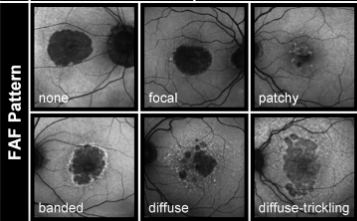
Figure 4: Courtesy of Fleckenstein et al.
Pathophysiology: The role of the complement system and genetics
The main phenotypic pathway which results in GA is drusen, followed by hyperpigmentation, regression of drusen, hypopigmentation, and ultimately RPE cell death, with the development of atrophic retina and choriocapillaris. This process can take 5 to 6 years, from large drusen (>125 microns) and hyperpigmentation to the development of geographic atrophy. Large confluent drusen are a risk factor for progression to atrophy.4
Geographic atrophy can also follow after drusenoid RPE detachment, regression of choroidal neovascular membrane, or RPE rupture.4
Figure 5 demonstrates the increased effects over time in geographic atrophy from pegcetacoplan treatment.18

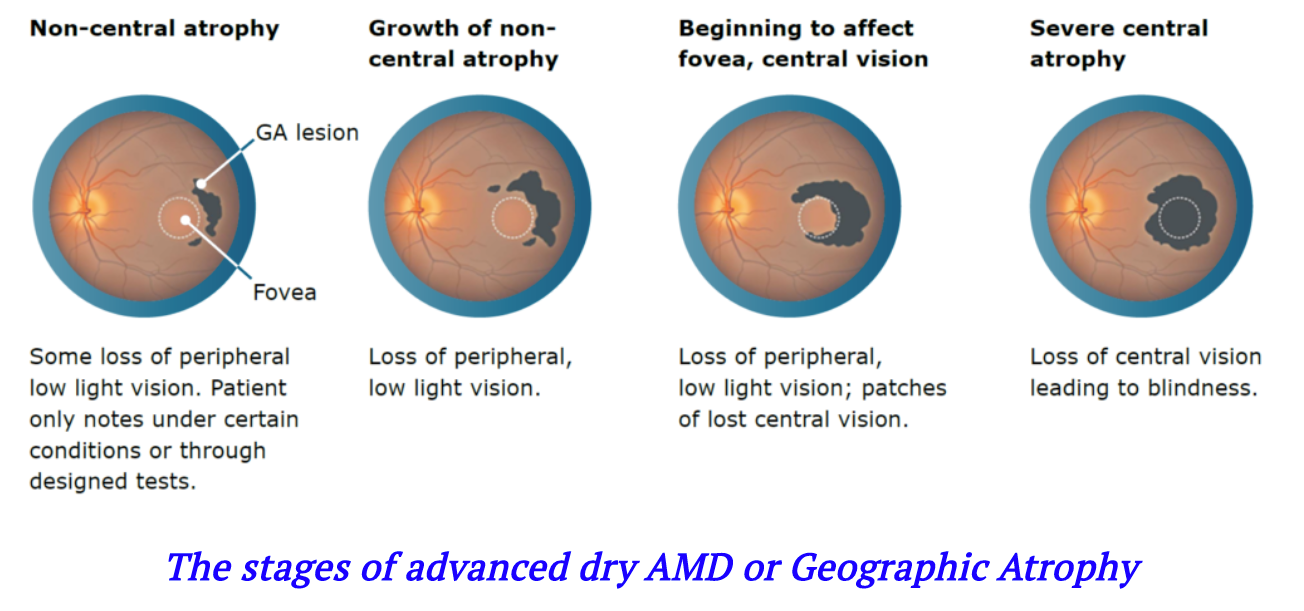
Figure 5: Courtesy of BioPharm Analyses.
Using the complement system to treat geographic atrophy
This is what happens on the phenotypic level. Recent advances aim to detect changes in the cellular, genetic, and even metabolomic levels, and novel treatments target these various pathways.19
GA is a complex disease and different treatments currently advancing towards commercialization or under clinical program development with several targets, including complement inhibition, neuroprotection, inflammation reduction, cell therapy, and visual cycle modulation.19
Of all the proposed treatments, inhibition of parts of the complement system has garnered the most attention from researchers and clinicians alike. There are two treatments looking, specifically at the complement system, currently undergoing Phase 3 trials.
What exactly is the complement system, and how is it relevant?
The complement system is a non-cellular part of the innate immune system, composed of three different pathways, including the classical, lectin, and alternative pathways.19
The classical pathway of the complement system is pathogen-mediated and activated by immune complex deposition (IgG or IgM), whereby the antigen-antibody complex forms and the Fc portion containing the complement binding site is exposed, initiating the complement cascade.13
The other arm of the complement system is the lectin pathway which is activated by non-self-recognition. Protein recognition receptors, such as mannose-binding lectin, identify non-self molecules, especially select highly conserved pathogen-associated molecular patterns, leading to the initiation of the complement cascade.13
The alternative pathway is different from the other two pathways and is activated by spontaneous hydrolysis of C3 in plasma. This is antibody independent.13,20 Genetic evidence suggests that this pathway may be dysregulated in AMD patients.20
Figure 6 highlights the complement cascade inhibition pathway.13

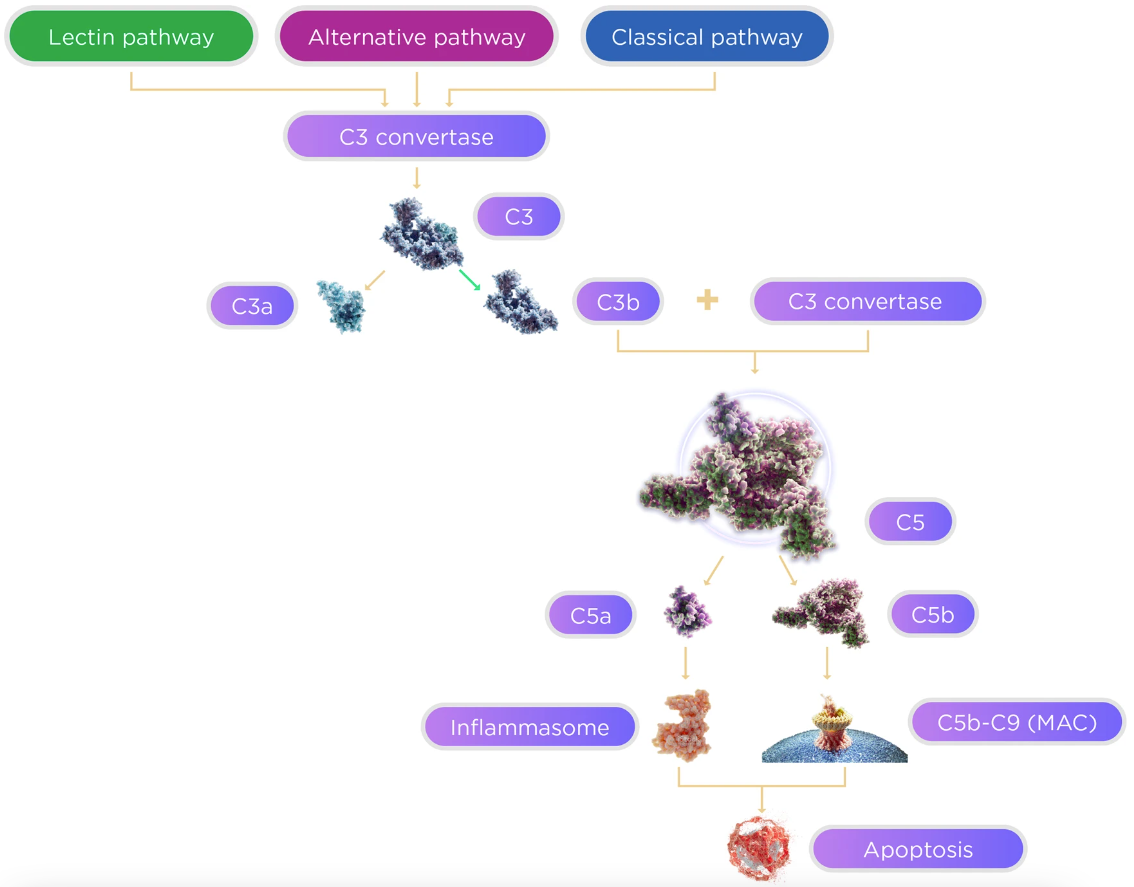
Figure 6: Courtesy of Desai et al.
The pathophysiology of the complement system pathway
The three pathways all converge at C3 and cascade down to C5, ultimately leading to inflammasome and membrane attack complex (MAC or C5b-9) formation and eventually causing apoptosis or cellular death.13
Various complement components, including C3, C5b-9 (MAC), CFB, and CFH, have been found in drusen and GA. Increased plasma levels of C3a, C3d, Bb, and C5a have been found in AMD patients. These studies suggest involvement of the complement system at a localized level as well as potentially systemic level in AMD patients.13,20
Additionally, studies have shown that polymorphisms in a number of complement genes, including CFH, CFB, C2, C3, and SERPING1, increase the risk of AMD, again suggesting involvement of different parts of the complement system.13,20
Within the complement cascade, C3a and C5a are potent inflammatory mediators known as anaphylatoxins which cause vasodilation and increased permeability of small blood vessels; are chemotactic to neutrophils, mast cells and leukocytes; trigger oxidative burst in macrophages and eosinophils; release histamine from basophils and mast cells; and result in further proinflammatory cytokine production, as well as tissue regeneration and fibrosis.13,20 It is here that current treatments are being focused on.
Treatments for AMD and geographic atrophy
The following section highlights some of the most recent advances in AMD, including an emphasis on pegcetacoplan and avacincaptad pegol, each of which inhibits a different part of the complement system and are both currently undergoing FDA evaluation.
AMD treatments targeting the complement system: Pegcetacoplan
Pegcetacoplan (APL-2, Apellis Pharmaceuticals, Waltham, MA, USA) selectively inhibits complement factor C3. In the Phase 2 trial (FILLY), patients who received APL-2 monthly for 12 months had a 29% lower rate of GA progression. Patients who received APL-2 every other month had a 20% lower rate of GA progression. Of note, there was an increase in the incidence of conversion to wet AMD in APL-2 treated eyes, with a 20.9% increase in the monthly treated group and an 8.9% increase in the every other month group.
The Phase 3 DERBY and OAKS trials are ongoing. The 24-month results from these trials were recently announced and showed a 19 to 22% reduction in GA lesion growth with monthly treatment and a 16 to 18% reduction in GA lesion growth with every-other-month treatment.
Most notably, between months 18 and 24, the treatment effect accelerated compared to prior 6-month treatment intervals, with a 24 to 36% reduction in GA growth with monthly treatment and a 25 to 29% reduction in GA growth with every other month treatment.21
The FDA evaluated the new drug application (NDA) submitted by Apellis and has approved intravitreal pegcetacoplan (Syfovre) as of late February 2023, making it the first FDA-approved treatment for geographic atrophy.19,22,23
AMD treatments targeting the complement system: Avacincaptad pegol
Avacincaptad pegol (Zimura; Iveric Bio, Cranbury, NJ, USA) selectively inhibits C5. In the phase 2/3 Trial (GATHER1), patients who received Zimura 2mg for 1 year had a 27.4% reduction in the rate of GA growth. Patients who received Zimura 4mg for 1 year had a 27.8% reduction in the rate of GA growth.
Rates of choroidal neovascular membrane (CNVM) formation were higher for patients undergoing treatment with Zimura, with 9% in the 2mg dose and 9.6% in the 4mg dose, compared to only 2.7% in the sham cohort.
Iveric Bio has submitted an NDA to the FDA and has received Breakthrough Therapy designation.19,22
Gene therapies targeting the complement system
HMR59 or AAVCAGsCD59 (Hemera Biosciences, Waltham, MA, USA) is a gene therapy that inhibits the complement system. An adeno-associated virus serotype 2 (AAV2) vector is delivered by intravitreal injection, which leads to the production of a form of CD59 that prevents the binding of C9 proteins in the complement cascade and therefore inhibits the formation of the membrane attack complex (MAC). A Phase 1/2 trial is underway.19,22,24
GT005 (Novartis AG, Basel, CH–formerly Gyroscope Therapeutics, London, UK) is a gene therapy that inhibits the complement system by supplementation of CFI. This also uses an AAV2 vector but is delivered by subretinal injection. The Phase 1/2 trials FOCUS and HORIZON are currently underway.19
GA treatments targeting neuro-protection
Elamipretide (Stealth Biotherapeutics, Newton, MA, USA) reduces mitochondrial dysfunction, which is thought to play a role along with oxidative stress in GA. Subcutaneous elamipretide 40mg daily is currently being evaluated in a Phase 2 trial (ReCLAIM-2).19
Intravitreal delivery of brimonidine tartrate (Allergan, Dublin, Ireland) by a delayed delivery system (DDS) which is released over 6 months, is currently being evaluated. Brimonidine is thought to have neuro-protective effects and has been used by glaucoma specialists in the past for this reason.25
A Phase 2a clinical trial showed decreased rates of GA progression, but this was not statistically significant. Phase 2b trial (BEACON) using a higher dose showed further decreased rates of GA progression. There are two Phase 3 trials (IMAGINE and ENVISION) currently underway.19,22
GA treatments with anti-inflammatory agents
Tetracyclines are antibiotics that also have anti-inflammatory properties via decreasing reactive oxygen species, inhibiting apoptosis, preventing complement activation, and inhibiting matrix metalloproteinases, which are responsible for breaking down the barrier between RPE and Bruch's membrane.26 Doxycycline (Oracea; Galderma Laboratories, Fort Worth, TX, USA) 40mg by mouth daily versus placebo is currently being evaluated in a Phase 3 trial.19
RG6147 (Genentech, San Francisco, CA, USA) is an antibody that inhibits HTRA1, a serine protease gene involved in the pathogenesis of GA. A Phase 2 trial (GALLEGO) is currently underway comparing an intravitreal injection of RG6147 to sham control.19
Visual cycle modulators to treat geographic atrophy
ALK-001 (Alkeus Pharmaceuticals, Cambridge, MA, USA) is a synthetic vitamin A product that looks to potentially reduce the accumulation of toxic vitamin A dimers that lead to GA. A Phase 3 trial is underway examining patients that receive oral ALK-001 versus sham.19,22
Other therapies for geographic atrophy
GEM103 (Gemini Therapeutics, Cambridge, MA, USA) is a recombinant human form of complement factor H (CFH) given by intravitreal injection. This is being studied to improve complement modulation in patients with CFH mutations. A Phase 2 trial is underway.19
Risuteganib (Allegro Ophthalmics, San Juan Capistrano, CA, USA) is an integrin peptide given by intravitreal injection with positive results in a Phase 2a trial.
There are numerous other trials currently ongoing, including trials studying oral minocycline, metformin, and carbidopa-levodopa.19
Concluding remarks
While Mrs. Jones’ situation is rather unfortunate, she will benefit from a low vision referral and evaluation for low vision aids, which will help her with her daily activities. This upcoming year and the remainder of the 2020s look very promising for pharmacologic advances that stand to help millions of patients around the world like Mrs. Jones who suffer from geographic atrophy.
As eyecare professionals, it is our job and the commitment we make to our patients to stay up-to-date with the advances as they come so that we may offer and provide the latest treatments to preserve vision. I hope this guide helps in that regard.
