



As both a contact lens and dry eye specialist at the Miami Contact Lens Institute, I have seen firsthand the impact contact lenses have on the ocular surface—and their ability to significantly aid in surface health.
But before examining the benefits of scleral contact lenses, let’s look at dry eye as a disease.
How is dry eye defined?
The Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop (DEWS) II study revolutionized the definition of dry eye by identifying the following characteristics.
Based on the TFOS DEWS II study, dry eye:
- Is a multifactorial disease of the ocular surface, causing ocular symptoms.
- Is characterized by a loss of homeostasis of the tear film.
- Has key components of tear film instability, hyperosmolarity, ocular surface inflammation, and neurosensory abnormalities, which play etiological roles.
Aqueous deficient versus evaporative dry eye
In addition, dry eye disease (DED) falls into three categories: aqueous deficient, evaporative, and a mixture of the two.
In a nutshell, with aqueous deficient dry eye, not enough tears are produced. This could result from Sjögren’s syndrome, refractive surgery, a reflex block, systemic drugs, lacrimal obstruction, autoimmune diseases, and many other causes. With OU 4 severe superficial punctate keratitis (SPK) from an aqueous deficient dry eye, a patient would experience increased blink rate, overall discomfort, pain, grittiness, and redness.
With the evaporative variety of DED, a sufficient amount of tears are being produced but are prone to excessive evaporation. Contributing culprits are meibomian gland dysfunction, anterior blepharitis, deficient unstable lipid layer, and vitamin A deficiency, among others.
To find the right treatment, with the ultimate goal of restoring homeostasis, it's important to isolate the underlying cause and determine whether aqueous deficient, evaporative, or a combination of both is at the root. However, all types lead to inflammation, which, if not interrupted, will perpetuate and worsen.
The role of biofilm
Another component that must be addressed is biofilm. In anterior blepharitis, biofilm refers to the layer of bacteria living on the lids and lashes that can exacerbate evaporation, creating dryness, redness, grittiness, and overall inflammation and leading to contact lens intolerance.
Diagnostic testing for dry eye disease
As other ocular surface diseases (OSD) can mimic dry eye, utilizing appropriate diagnostic testing to differentiate is crucial. First, I utilize the OSDI questionnaire to get a thorough understanding of how dry eye affects the patient’s everyday life and grade the dry eye based on their subjective answers. After initiating treatment, I find it useful to readminister the questionnaire and reassess for improved quality of life.
Staining is also very useful in dry eye diagnosis. Lissamine Green shows dead and devitalized cells on the conjunctiva as well as lid wiper epitheliopathy (LWE). Fluorescein reveals dead and devitalized cells on the cornea. Other helpful diagnostic tools are InflammaDry, which shows hyperosmolarity, the phenol red thread test, the Schirmer test to help determine basal tear, and the Sjö diagnostic test.
Once diagnosed, the next step is to educate the patient on the disease itself and what preliminary treatments are available to incorporate into their daily routine to alleviate symptoms.
Treatment options for evaporative dry eye include:
- Hot compresses to liquefy the meibum from the meibomian glands and restore function
- Artificial tears to lubricate the ocular surface and aid in tear film instability
- Eyelid hygiene, which should entail cleaning the lids and lashes twice a day to reduce/remove biofilm
- Omega-3 supplements
However, the TFOS DEWS II study reports that rigid scleral lenses are also considered a viable treatment for moderate to severe dry eye.
Scleral lenses for dry eye disease
In total, there are 62 indications for scleral lenses. A broad range of ocular surface diseases and conditions can be addressed, including Sjögren's syndrome, neurotrophic keratopathy, rosacea, chemical burns, Stevens-Johnson syndrome, corneal dystrophies, nerve palsies, atopic keratoconjunctivitis, limbal stem cell deficiency, vernal keratopathy, and persistent epithelial defects, just to name a few.
Scleral lenses have the ability to improve anterior ocular surface health by providing a hydrating dome that protects the surface from aggravating factors in the outside environment. Essentially, the scleral lens creates a forcefield around the cornea and conjunctiva that keeps bacteria, debris, deposits, and anything that can be causing dry eye (such as exposure keratopathy) at bay.
In addition, hydration and medication can be added to this corneal vault in the form of preservative-free artificial tears, antibiotics (i.e., moxifloxacin), autologous serum tears, amniotic membrane drops, etc.
For the length of time that the patient is wearing the lens—up to 16 hours—they are reaping the benefits of hydration, restoration, and protection from the oasis within the lens.
Figure 1 is a side-by-side comparison of before and after scleral lens wear in a patient with severe ocular surface disease.

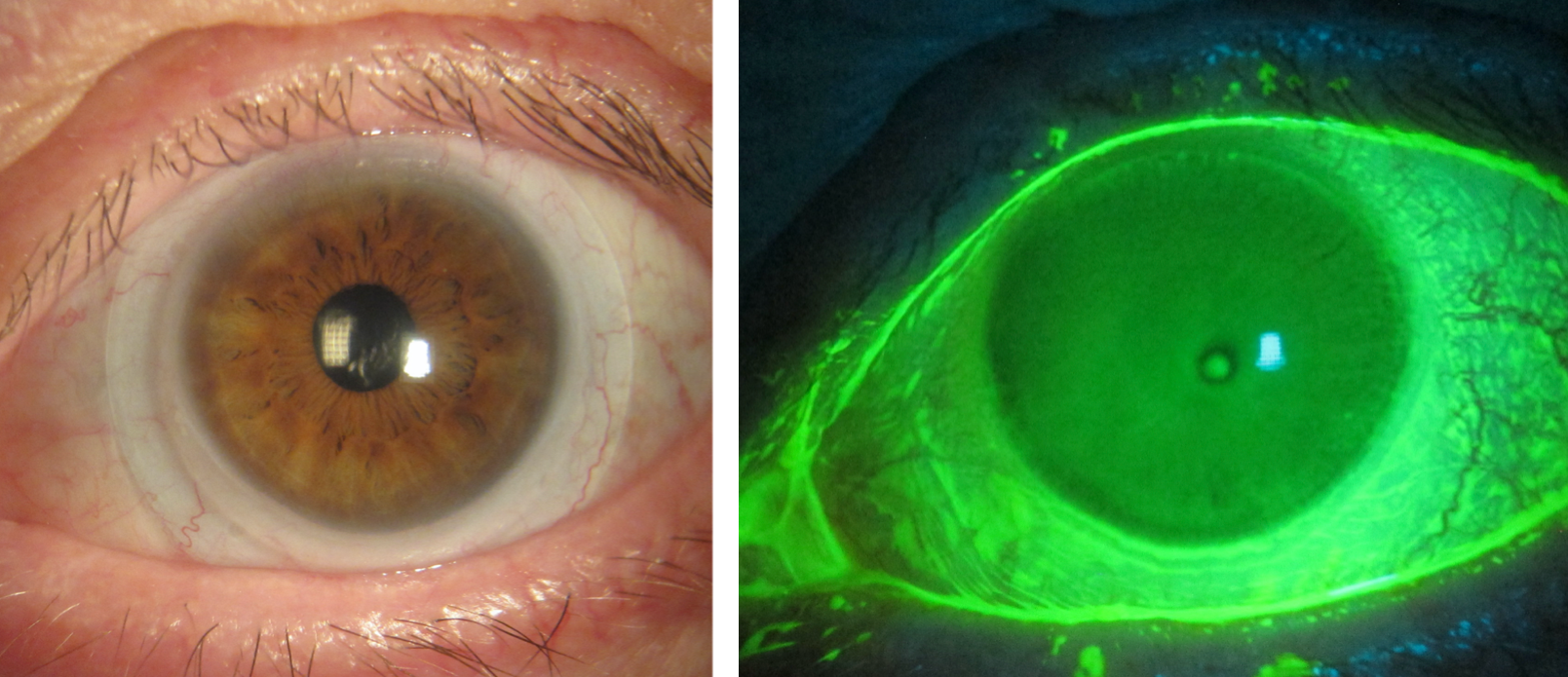
Figure 1: Visionary Optics
For the reasons noted thus far, when dry eye is at play, scleral lenses are often a better choice than rigid gas-permeable lenses. A 2020 study by Levit et al. comparing the comfort of corneal rigid gas permeable lenses versus large diameter scleral lenses found that subjective comfort scores were significantly superior for scleral lenses.
Addressing the pre-lens tear film
For best vision, the contact lens must have an even and continuous pre-lens tear film. Poor lens surface wettability can involve mucoid, lipid, or protein coatings on the lens surface.
An inadequate pre-lens tear film can mean the difference between a comfortable, clear lens and a painful, cloudy lens. As it is the first refractive index that light touches prior to hitting the lens, it has a distinct impact on vision. Despite advances in materials and surface coatings of scleral lenses, it can still be challenging to achieve a good pre-lens tear film for patients who have dry eye disease.
However, there are ways to mitigate this.
Troubleshooting a pre-lens tear film insufficiency:
- Treat all lenses with plasma and consider the addition of Hydra-PEG coating, a polyethylene glycol (PEG)-based polymer mixture designed to maintain tear film.
- Adhere to standard treatment protocol: preservative-free artificial tears, hot compresses, eyelid hygiene, Omega-3, and in-office treatments, like LipiFlow.
- Address any allergies by eliminating the allergen or treating them with an appropriate pharmaceutical agent.
- Ensure the patient uses all skincare and cosmetics products after applying the lenses to avoid the accumulation of deposits on the lens and causing a hydrophobic surface.
- Improve the cleaning regimen by using an extra-strength, alcohol-based, or peroxide cleaner.
- Have the patient use a wet Q-tip or their application plunger to wipe away the deposits without removing the lens.
Reducing debris in the tear film reservoir
Debris in the tear film reservoir can exacerbate dry eye symptoms, as the fluid dynamics attract deposits, especially if the limbal clearance is excessive. Conversely, a lack of tear exchange can lead to accumulation over time. Patients will notice midday fogging and consequent blurred vision.
The key is to avoid the removal and reinsertion of the lens, which in itself can increase debris accumulation.
Troubleshooting tear film reservoir debris:
- Treat any ocular surface disease and eyelid deposits using preservative-free artificial tears, hot compresses, eyelid hygiene, Omega-3, and in-office treatments, like LipiFlow.
- Modify the peripheral curves or reduce the lens diameter to improve tear film exchange.
- Modify the curves to reduce limbal clearance; excessive limbal clearance will cause negative pressure and attract debris into the tear film.
- Mix viscous artificial tears inside the bowl of the lens, which will maintain clarity and prevent fogging.
- Have the patient tilt their head and flush their tear film with saline without removing the lens.
- As a last resort, remove the lens, replenish with fresh saline, and reinsert.
Case report 1
A 51-year-old female with a history of Sjögren's syndrome and keratoconus presented for a scleral lens evaluation. The patient had also attempted to receive LASIK in the right eye, resulting in a flap, but no actual treatment was completed. For dry eye management, she had been previously treated with cyclosporine, lifitegrast, and punctal plugs.
At the time of her initial visit, she was wearing frequent-replacement soft lenses and had complaints of very poor vision. She had also attempted to wear hybrid lenses but stopped due to discomfort. With spectacles, vision was 20/40 in her right eye and 20/20 in her left.
After evaluation, the patient was fitted with a 16.5-millimeter, freeform, customized scleral lens with Hydra-PEG coating to improve her chance of successful wetting. Though she was able to achieve 20/20 vision in both eyes, during her first follow-up visit, she reported insufficient wetting in the right lens and symptomatic midday fogging of the left lens, which was also reported to be loose. We reordered and dispensed a left lens with a steeper landing zone.
At the 9-month follow-up, the patient reported the midday fogging resolved, but neither lens was wetting well, despite the Hydra-PEG coating. We noted significant deposits of lipid and protein on the left lens, which is not surprising as poor wetting often increases lens deposition. To improve wettability and decrease deposits, we prescribed a Tangible Boost solution, which worked to the patient’s satisfaction.
Case Report 2
In this case, a 4-year-old girl was referred for a scleral lens evaluation. The child was born with Manitoba-oculo-tricho-anal (MOTA) syndrome and had undergone multiple reconstructive surgeries, including tarsorrhaphy. Significant findings from her first visit showed bilateral upper eyelids with scalloped margins, severe amblyopia, symblepharon, and acquired corneal opacification secondary to exposure keratopathy with OS>OD.
Her visual acuity was 20/150 in her right eye and 20/400 in her left. Corneal scleral topography with a sMap3D showed substantial bilateral corneal and scleral irregularity.
At her initial visit, she was only being treated with preservative-free artificial tears. We ordered 14.9-millimeter scleral lenses, which required a single remake due to insufficient central clearance in both eyes. Beyond the fitting process, one of the biggest challenges with a child of such a young age is teaching the parents the application and removal techniques while ensuring the child's cooperation; we were successful in doing so.
With the prescribed scleral lenses, we significantly improved the patient’s vision, neutralized the irregular astigmatism, prevented further symblepharon formation, and promoted ocular surface restoration by preventing further amblyopia. We also expect the corneal scarring to improve to a degree.
In closing
When it comes to ocular surface disease, scleral lenses offer patients improvements not only in vision but in ocular surface health, resulting in an increased quality of life.
With multiple indications, many ways to troubleshoot potential complications, and the ability to customize, scleral lenses can prove invaluable. I encourage you to explore scleral lenses as a powerful tool in the treatment of dry eye disease.
