No matter where or how you practice, I have no doubt that you have come across a patient with
dry eye disease (DED). Nowadays, and especially as a result of increased screen and reading time from the
COVID-19 pandemic,
1 it seems that almost no patient is safe when it comes to the effects of dry eye. Therefore, it is imperative that we familiarize ourselves with both the common and the more unique therapeutic management options for DED.
When artificial tears fail us, what other dry eye management tools can we whip up? One seemingly underutilized tool is a scleral lens.2 Let’s continue the conversation below and perhaps you will be convinced that a scleral lens option might just be the right choice for some of your dry eye patients.
What is dry eye disease (DED)?
Dry eye disease has been identified as a chronic, inflammatory, multifactorial condition of the ocular surface.
3 Let’s define the ocular surface: this is a complex system that is composed of multiple ocular tissues functioning together. These tissues include the eyelid, conjunctiva, cornea, tear film, lacrimal glands and meibomian glands.3
A healthy ocular surface means there is equilibrium or homeostasis between these tissue functions, both physiologically and mechanically. From a physiological standpoint, the meibomian, lacrimal and accessory glands work to produce good quality tears for sufficient ocular surface lubrication. And from the mechanical standpoint, the act of eyelid blinking spreads these tears evenly across the ocular surface, spreading the lubrication as well as serving to protect the ocular surface.
Tear film instability and hyperosmolarity, damage to the ocular surface epithelium, ocular surface and lacrimal gland inflammation, as well as neurosensory abnormalities disturb this homeostasis resulting in dry eye.3 Clear and comfortable vision requires a healthy ocular surface and any imbalance in the homeostasis of the tear film can ultimately affect patient symptoms and vision.
DED can be classified into evaporative, aqueous deficient, or a combination of both.
4 Meibomian gland dysfunction (MGD) is considered to be the major cause of evaporative dry eye and approximately 70% of patients with DED have some form of MGD.
4 Blink abnormalities also play a role in evaporative dry eye. The most common causes of aqueous deficient dry eye stem from autoimmune systemic conditions, such as
Sjogren’s disease or chronic Graft versus Host Disease (cGVHD).
Although it can happen, the prevalence of aqueous deficient dry eye in isolation (without any component of evaporative dry eye) is rare.4 A mixed form or combination of both evaporative and aqueous deficient dry eye is present in 50-70% of DED patients.5
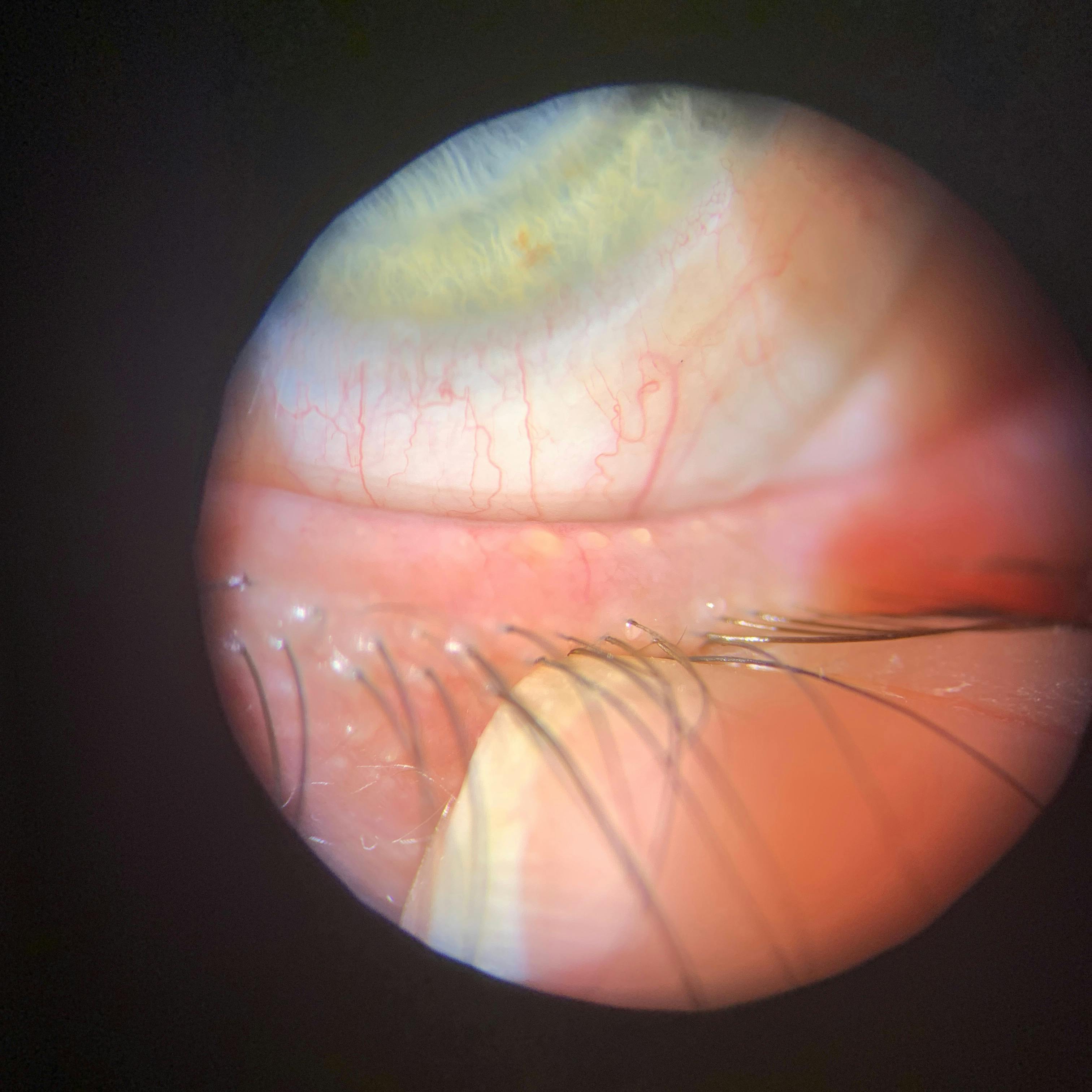
In Figure 1 and Figure 2, dry eye disease can be classified as meibomian gland dysfunction (MGD). This is a condition characterized by erythematous, thickened and scalloped eyelid margins, telangiectasias on the eyelid margins, and inspissated and blocked meibomian gland orifices as well.
Figure 1
Figure 2
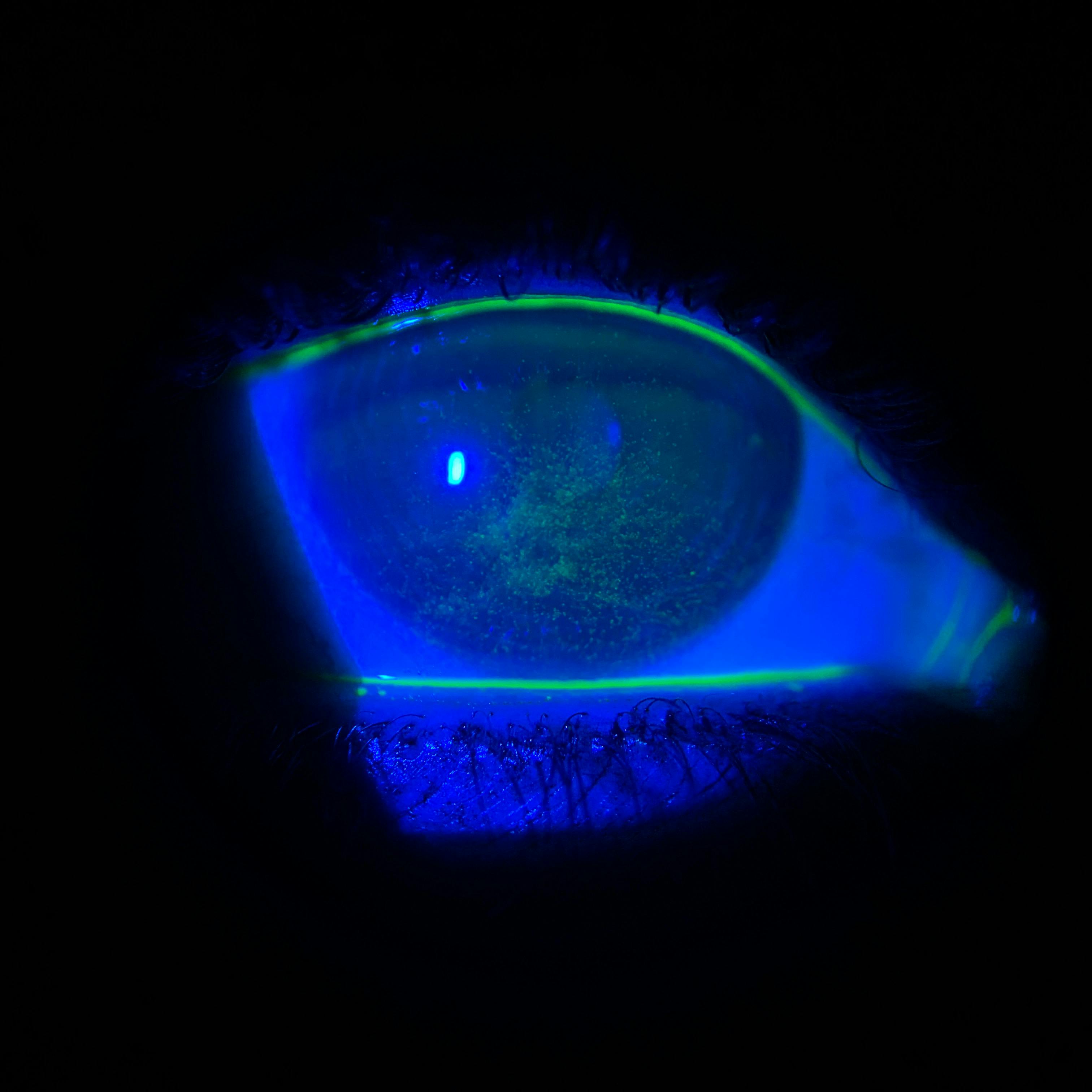
As seen in Figure 3, manifestations of dry eye disease include superficial punctate keratitis.
Figure 3
How can we treat DED?
The
Tear Film and Ocular Surface Society’s Dry Eye Workshop II (TFOS DEWS II) provides a framework for the management of DED based on the patient’s disease severity.
6 This is a stepwise approach designed to provide a level of structure for dry eye management. The first line of therapy, or step 1 of the algorithm, includes patient education on prognosis and lifestyle modification as well as other
dry eye therapy fundamentals, such as warm compresses, lid scrubs, and ocular lubricants/artificial tears.
As we move higher along the disease severity list, we come across a treatment modality that might seem a bit counterintuitive:
contact lenses. You might be thinking, I’ve learned that contact lenses exacerbate dryness, how can they be a treatment for dry eye? It is true that both contact lenses and ocular surface disease (OSD) are risk factors for microbial
keratitis, therefore it does seem ironic that contact lenses would be a treatment for ocular surface disease.
However, when selected for the right patient, contact lenses can serve to not only visually correct, but can also play a major therapeutic role in ocular surface rehabilitation. This is especially true for scleral lenses.
What is a scleral lens?
A
scleral lens is a large diameter rigid gas permeable (RGP) lens designed to vault over the cornea and limbus, and land evenly on the bulbar conjunctiva that overlies the sclera.
7 Scleral lenses can be manufactured in varying diameters, ranging from 14 to greater than 20 millimeters.
7The selection of a scleral lens diameter depends on various factors including the patient's:
- Horizontal visible iris diameter (HVID)
- Palpebral aperture
- Indication for scleral lens wear (we may go larger in diameter to protect more of the ocular surface)
Prior to application, the lens bowl of a scleral lens is filled with non-preserved saline solution. This allows the cornea to bathe in fluid, providing continuous hydration. With its rigid material property, a scleral lens is a mechanical barrier for surface protection and, via its fluid reservoir, this device serves to reduce corneal desiccation.8
Who is a candidate for scleral lenses for dry eye?
A stepwise approach to DED management will help in identifying the most appropriate
scleral lens candidates for dry eye. Scleral lenses should not be the first line of therapy for patients with dry eye signs and symptoms. According to the TFOS DEWS II management report, scleral lenses have been identified as step 3 in the management scale.
6 Scleral lenses therefore are best suited for those individuals who have failed conventional dry eye therapy, such as topical lubricants and
topical prescription immunomodulator drops (such as topical cyclosporine or lifitegrast), and moisture goggles.
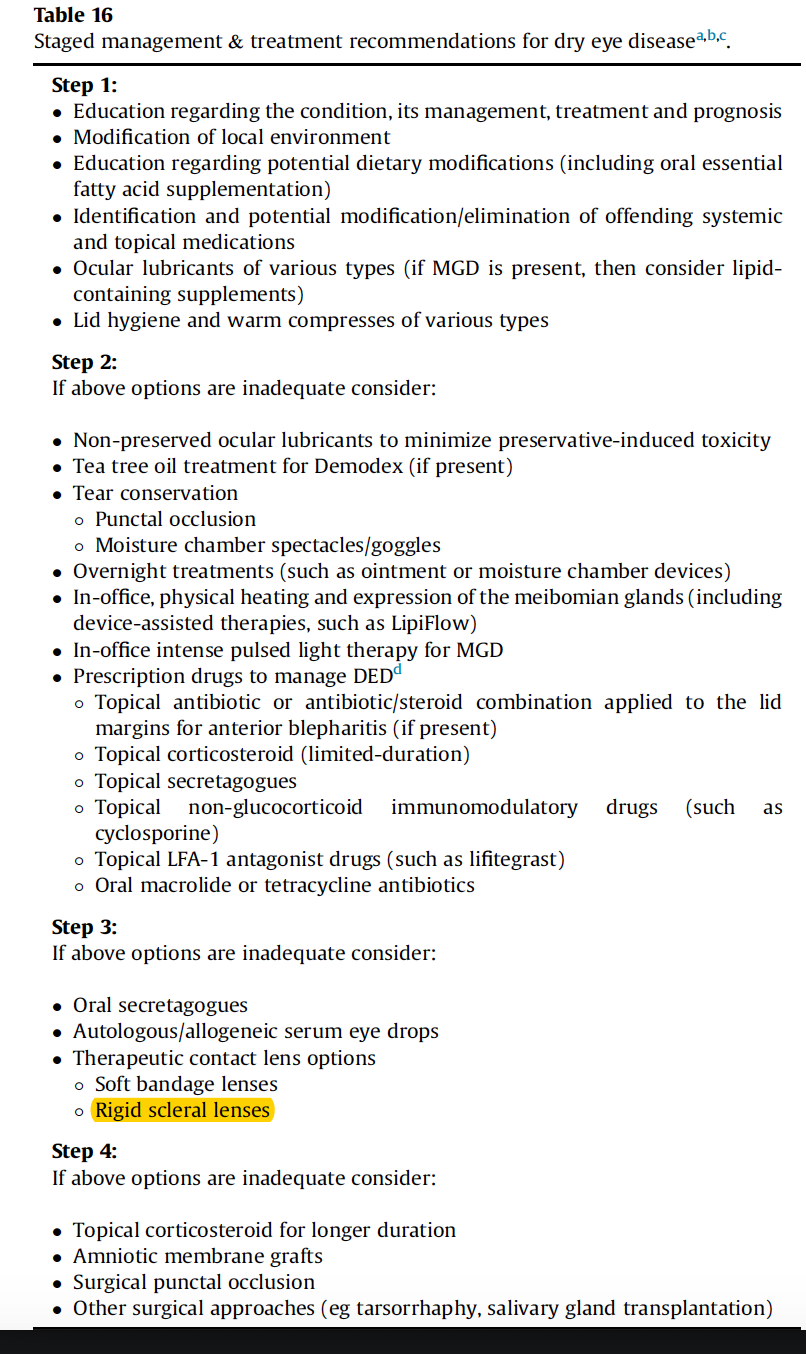
6Figure 4 is taken from the TFOS DEWS II Management and Therapy Report.6 It summarizes treatment types based on the 4 steps for staged management of dry eye disease. Rigid scleral lens (highlighted) falls in step 3 of the therapy stages, after dry eye foundational treatments, such as warm compresses and lid scrubs.
Individuals with exposure keratopathy, non-healing persistent epithelial defects, chronic graft versus host disease (cGVHD), Sjögren’s syndrome, Stevens-Johnson syndrome, ocular cicatricial pemphigoid (OCP), and other systemic autoimmune diseases that may cause ocular surface dryness will be excellent candidates for scleral lenses.
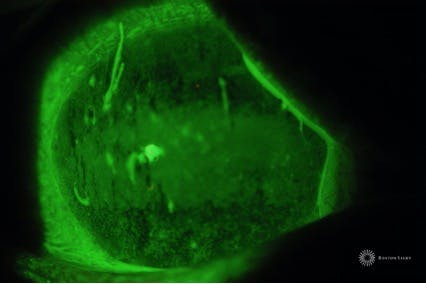
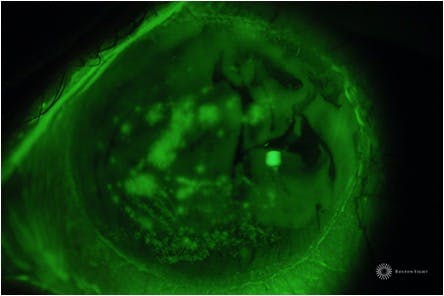
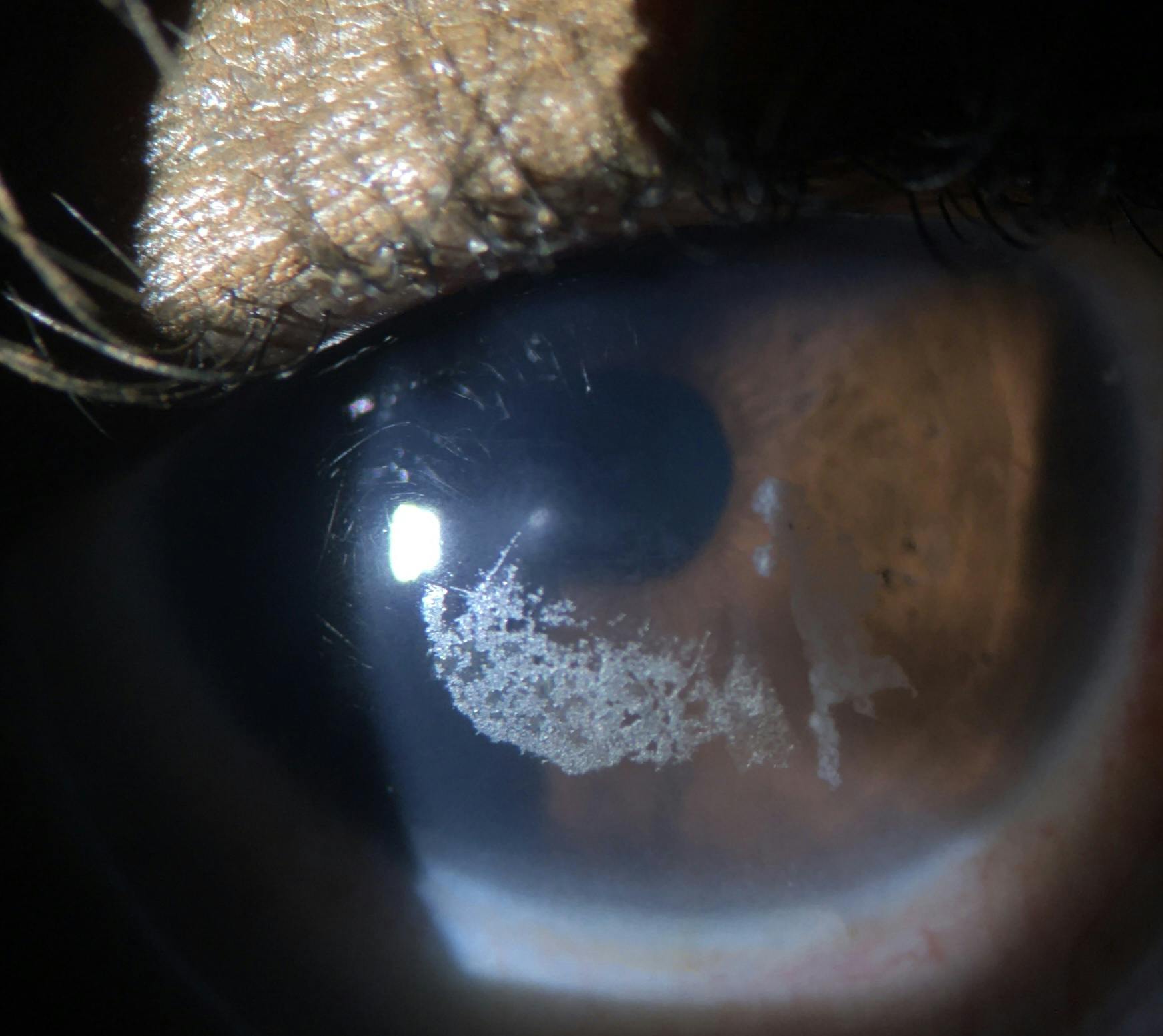
Figures 5-8 illustrate the effects of scleral lenses for a patient with cGVHD.
Figures 5 and 6 are the eyes pre-scleral lens wear. Coalesced punctate keratitis with mucous filaments and strands can be appreciated.
Figure 5: Photo courtesy of Dr. Alan Kwok, Boston Sight.
Figure 6: Photo courtesy of Dr. Alan Kwok, Boston Sight.
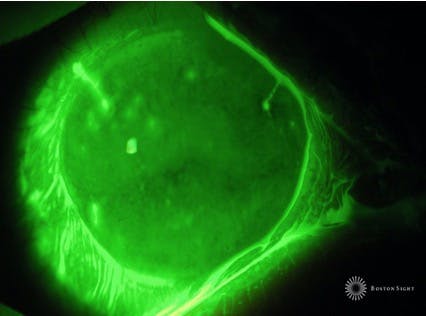
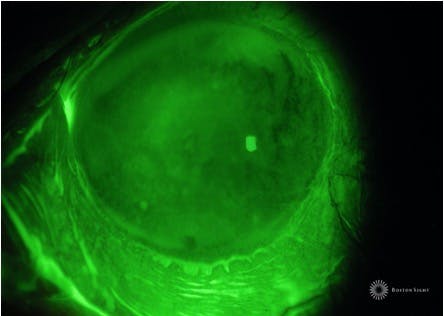
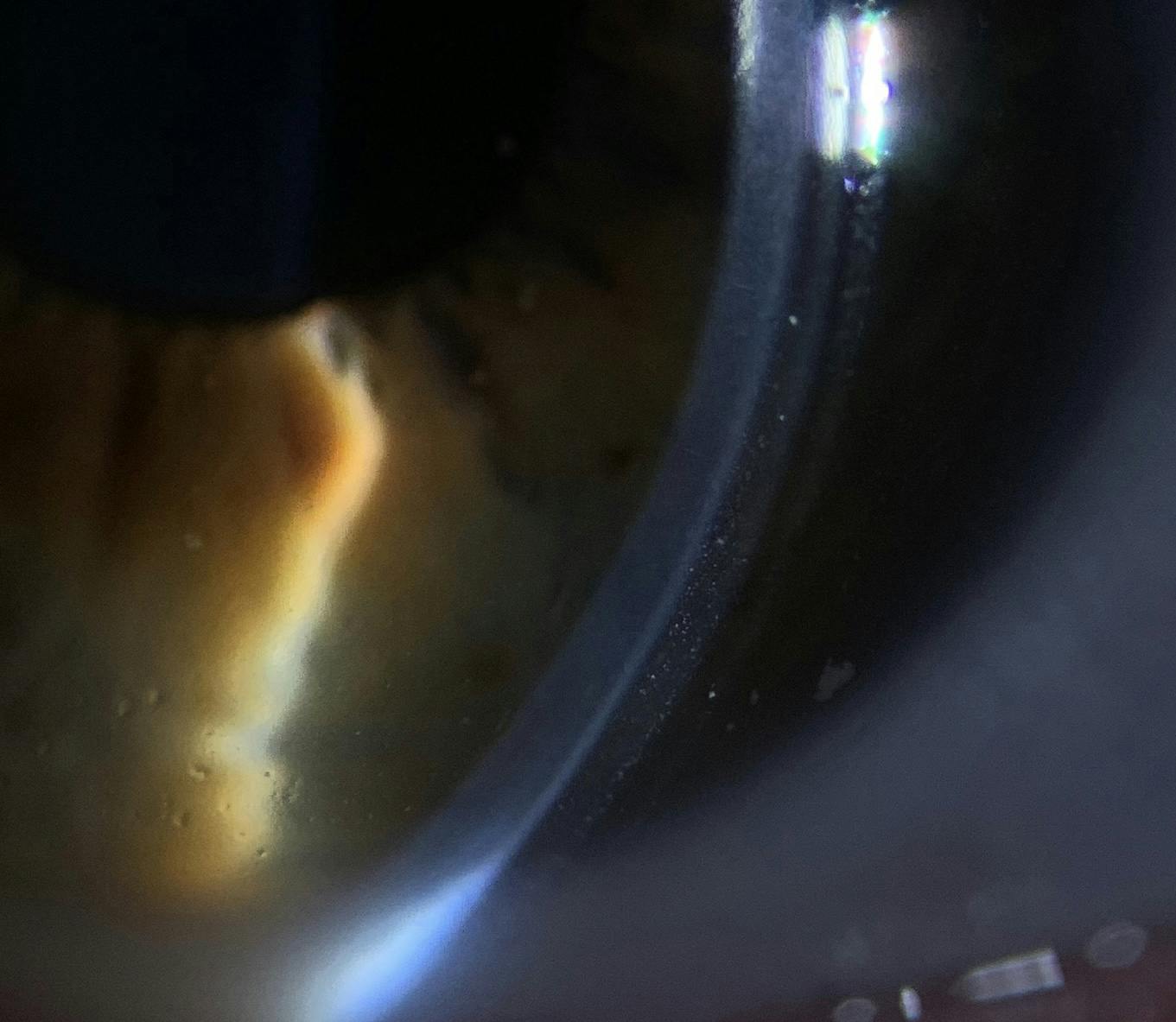
Figures 7 and 8 depict the cornea just 3 hours post-scleral lens wear. Here, we see ocular surface rehabilitation and marked improvement in the keratitis.
Figure 7: Photo courtesy of Dr. Alan Kwok, Boston Sight.
Figure 8: Photo courtesy of Dr. Alan Kwok, Boston Sight.
Another group of patients that do well with scleral lenses are patients with ocular neuropathy. Patients with chronic neuropathic pain will show up in your chair complaining of persistent foreign body sensation, extreme pain and photophobia without many corneal signs supporting their symptoms. This situation may leave you puzzled, especially if multiple attempts using conventional dry eye therapy have failed this patient. In individuals with
neurotrophic keratopathy, nerve disruption causes a hypersensitivity of the cornea and conjunctival somatosensory nerves.
For these patients, a scleral lens may just be the answer. Scleral lenses can disrupt this pain cycle and mitigate their symptoms.7-9
The main goal of scleral lenses for the treatment of dry eye is two fold: to provide ocular surface rehabilitation and hydration as well as symptom control. Depending on your patient’s dry eye severity, it will be necessary to couple scleral lenses with other dry eye therapies, such as topical lubricants, topical cyclosporine, topical autologous serum, punctal occlusion, and amniotic membranes.
Age should not be considered a limiting factor when it comes to
scleral lens fitting. Both pediatric and geriatic scleral lens fittings may be done with success, though application and removal training may need to be customized to meet your patients’ needs. A study by the Boston Sight group using the Prosthetic Replacement of the Ocular Surface Ecosystem (PROSE) device underscored the timing of the application and removal process. The study found that application and removal can be successfully taught in age diverse patients with no difference in time between younger and older age groups.
All patients could apply devices in less than 5 minutes by week 5, and remove devices in less than 3 minutes by week 3.10
How do I get started with fitting a scleral lens for my dry eye patient?
In general, scleral lenses are selected large enough to completely vault over the corneal and limbal surface with the intent to land evenly on the bulbar conjunctiva. The patient’s horizontal visible iris diameter is an important measure that can help in selecting a scleral lens large enough to clear the entirety of the cornea.
When it comes to dry eye and scleral lenses, we’ve discussed that an important objective is hydration and protection. Depending on the surface area that needs rehabilitation, it may be necessary to select a lens that is overall larger, so as to cover and protect a larger surface area. Special consideration should be given to patients with a history of tarsorrhaphy or symblepharon, or microcornea—in which case a smaller scleral lens may be necessary.8
Most modern scleral lenses are still fit using a diagnostic fitting process where an initial trial lens is applied on the eye and assessed for proper fitting characteristics. Recently, however, technological innovations in scleral profilometry (scleral topography) and impression-based scleral lens designs have produced precise measurements to allow empirical fitting of scleral lenses. These advancements in technology can offer several advantages for the fitting practitioner, such as optimized scleral lens fitting, improved patient satisfaction, and high rate of first lens success, and ultimately reduced chair time.11
I will argue, though, there is value in applying a scleral lens for your patient during the dry eye scleral consultation visit. Applying the lens in office first allows the patient to experience the therapeutic benefit of the scleral lens immediately.
Practically speaking, this initial positive outcome can be a beacon of hope for the patient throughout the fitting process and can be especially helpful in overcoming barriers when the going gets tough like dealing with potential fitting complications and lens handling concerns
There are a wide number of scleral lens designs and scleral lens manufacturing labs available to the practitioner. When starting out with fitting scleral lenses, it is prudent to select one or two scleral lens designs and labs that will provide solid consultation support. Begin with these designs and become comfortable with those specific lens designs (my advice is no more than three scleral lens designs to keep it simple) before offering multiple options to your patients. For fitting dry eye patients, ensure the manufacturer offers a larger diameter scleral lens.
During the diagnostic scleral lens fitting, a trial lens is selected from a fitting set and careful consideration is placed on selecting lens diameter and sagittal height parameters of the initial scleral lens. For the most part, a scleral lens design can be divided into three zones: the optic zone, the transition zone, and the landing zone. Each zone can be independently assessed to ensure a proper fit is achieved. As mentioned above, the scleral lens should not be touching any area of the corneal or limbal surface.
This is especially important for patients with dry eye, as any mechanical contact will disrupt the corneal epithelial integrity and further exacerbate dry eye signs and symptoms.
Ideal initial central vault, tear fluid reservoir (in microns) between the central cornea and the scleral lens, varies between 300 to 500 microns.11
Scleral lenses will settle into the bulbar conjunctiva with time, which will cause a decrease in central vault of about 80 to 100 microns.11-12 Larger lenses tend to settle more and may cause a shallower fluid reservoir overtime when compared to smaller scleral lenses.13 After settling, the target central vault should ideally be between 100 to 300 microns.11
When it comes to targeting fluid vaults for your dry eye patients, it may be worthwhile to consider fitting in the higher end of the target vault to ensure ample fluid thickness as the lens settles and to serve the goal of abundant corneal hydration.
Prior to lens application, the scleral lens is filled with preservative-free saline. Sodium fluorescein dye may be placed into the scleral lens bowl prior to lens application to better highlight the fluid reservoir during lens assessment. The amount of fluid vault under a scleral lens should be assessed using an optic section with white light via slit lamp observation. In addition, a diffuse cobalt blue filter can be used to identify any areas of corneal and scleral lens contact. Anterior segment optical coherence tomography (OCT) can also be helpful in quantifying the fluid reservoir at different points under the scleral lens.
If excessive or inadequate corneal or limbal clearance are identified, the sagittal depth or equivalent is adjusted and another trial lens is applied. This trial process continues until the closest sagittal height is matched to the desired central vault.
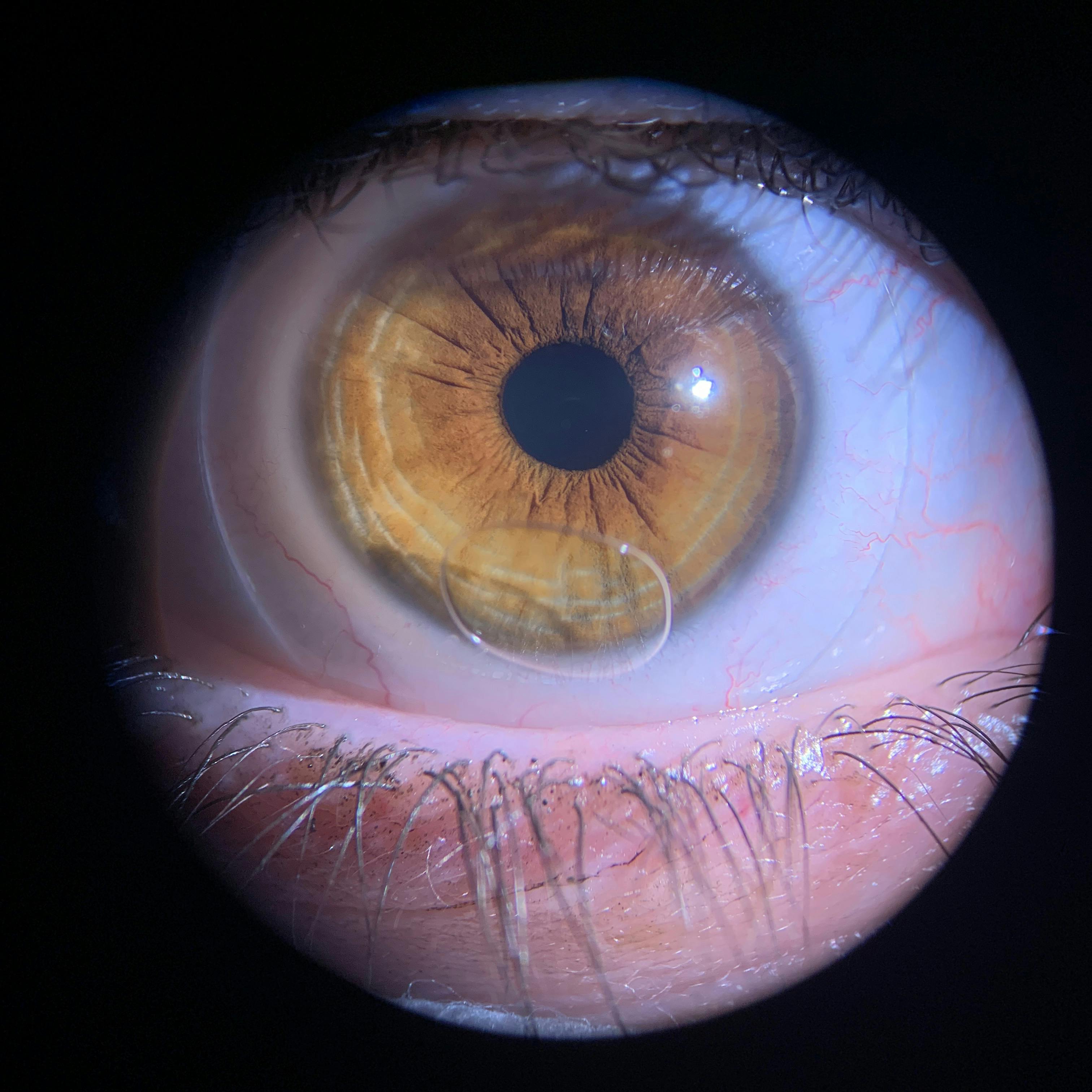
As seen in Figure 9, a scleral lens is typically applied using an application plunger. There are alternatives to using a plunger for lens application, such as placing the lens on a ring inserter or using the patients' own fingers for balance prior to application. The scleral lens is filled with non preserved sterile saline prior to lens application.
Figure 9
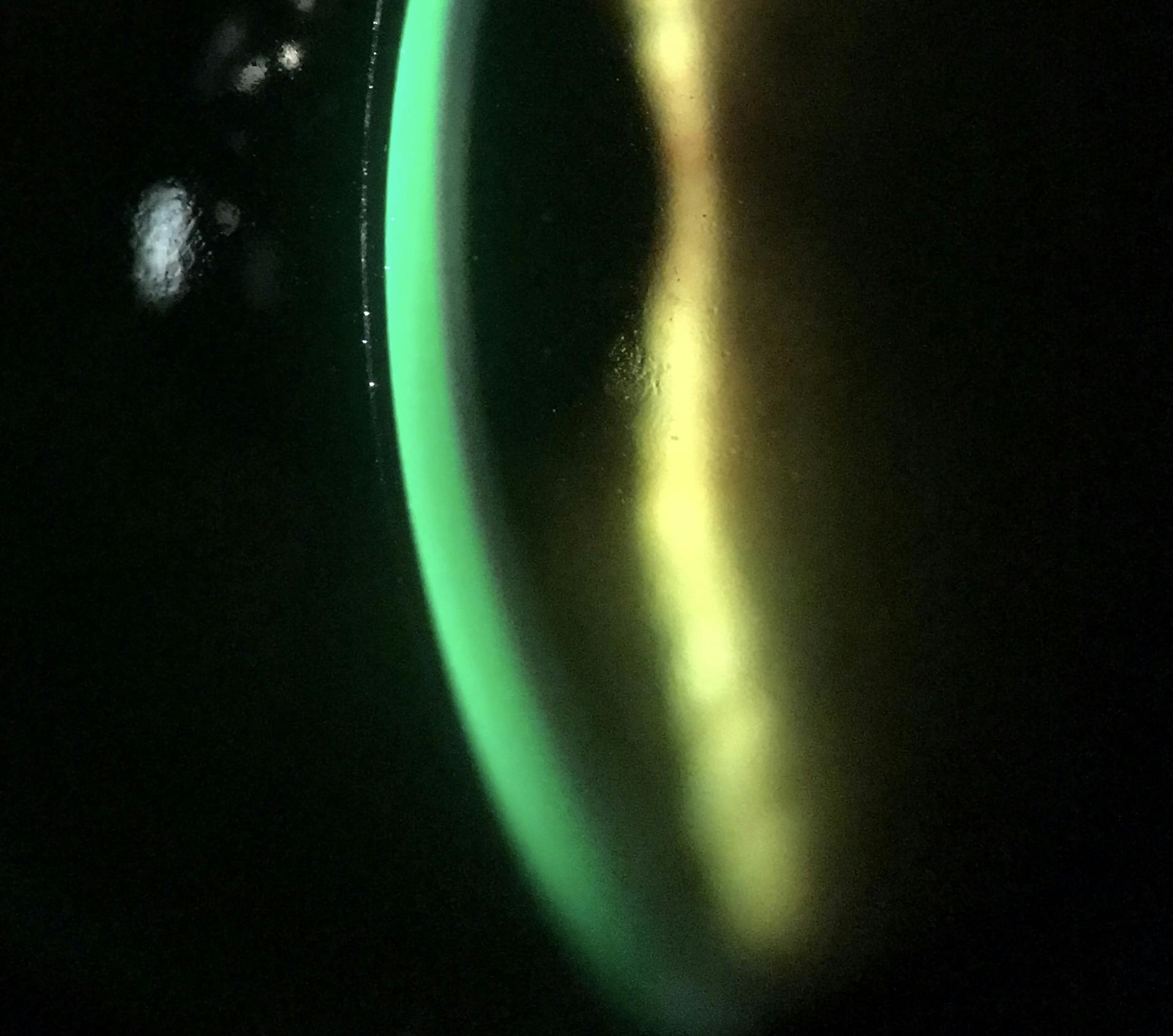
As demonstrated in figures 10-12, a scleral lens should be assessed under slit lamp biomicroscopy using an optic section and white light. When fluorescein dye is placed in the scleral lens bowl prior to application, it collects within the fluid chamber and is extremely useful in assessing the central clearance.
Figure 10 depicts excessive central clearance under a scleral lens as highlighted by a thick area of the fluorescein dye.
Figure 10
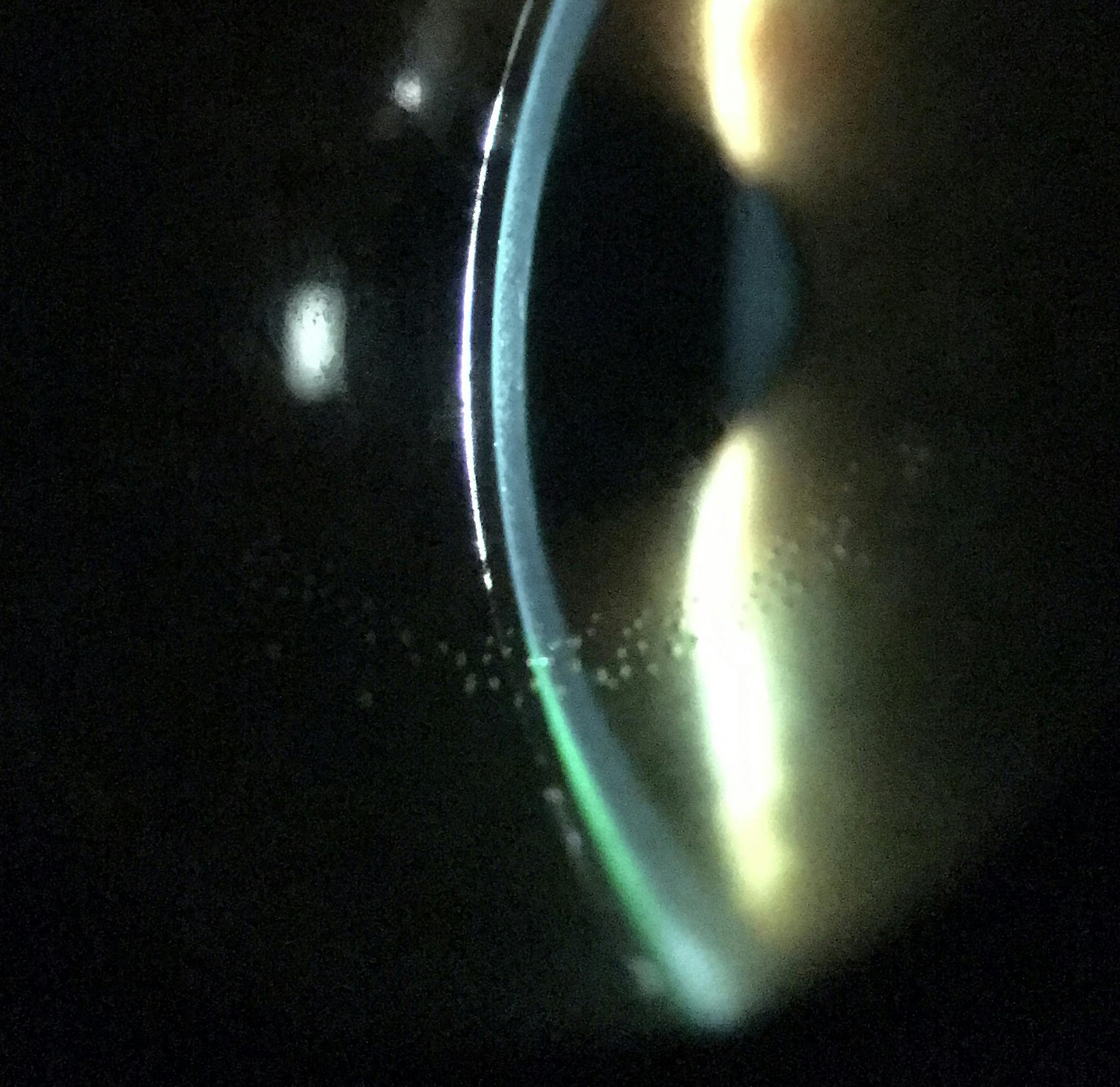
Figure 11 depicts inadequate clearance under the scleral lens as highlighted by minimal fluorescein dye observed under the scleral lens.
Figure 11
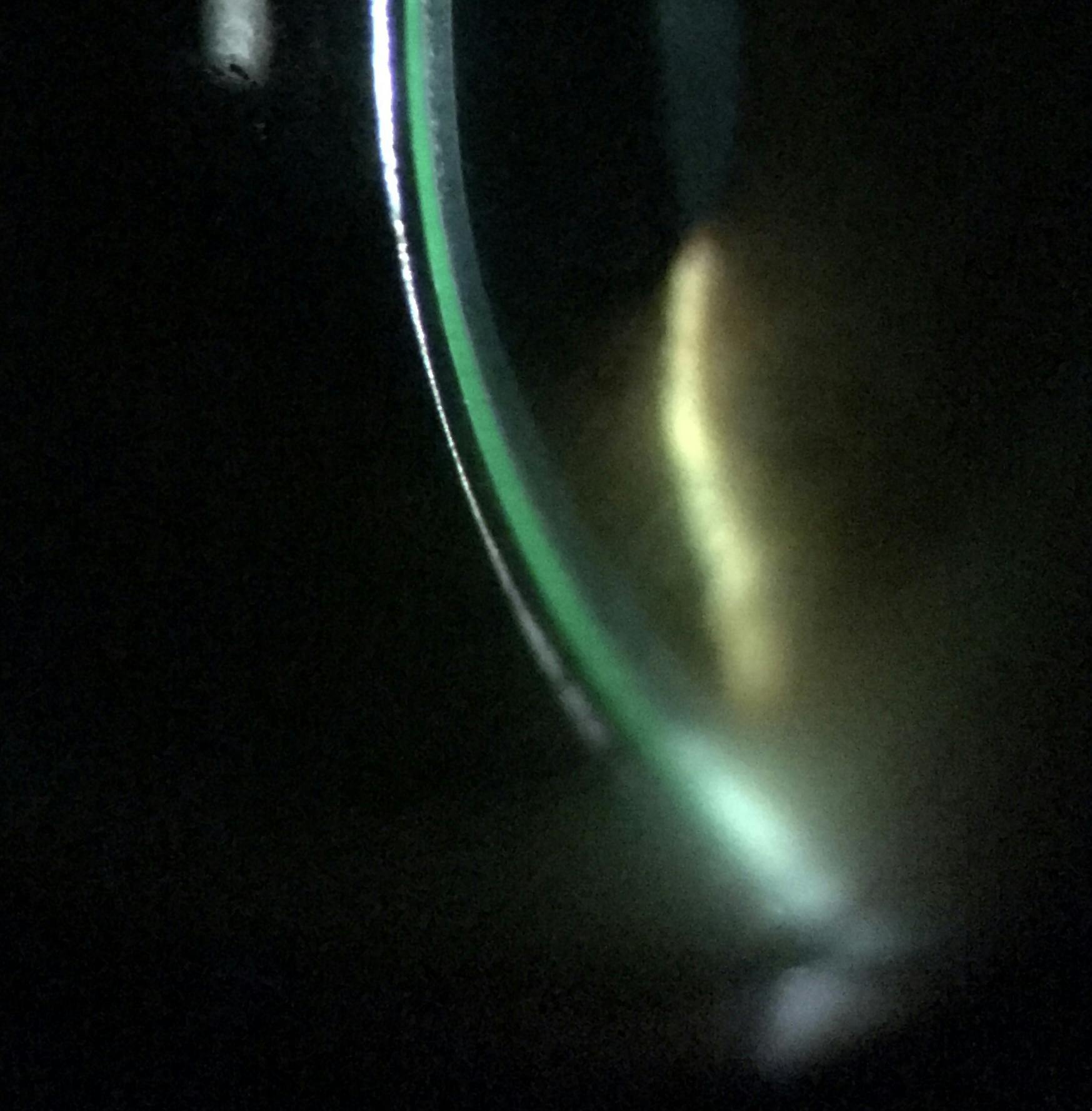
Figure 12 shows an ideal amount of central clearance under a scleral lens, post-settling.
Figure 12
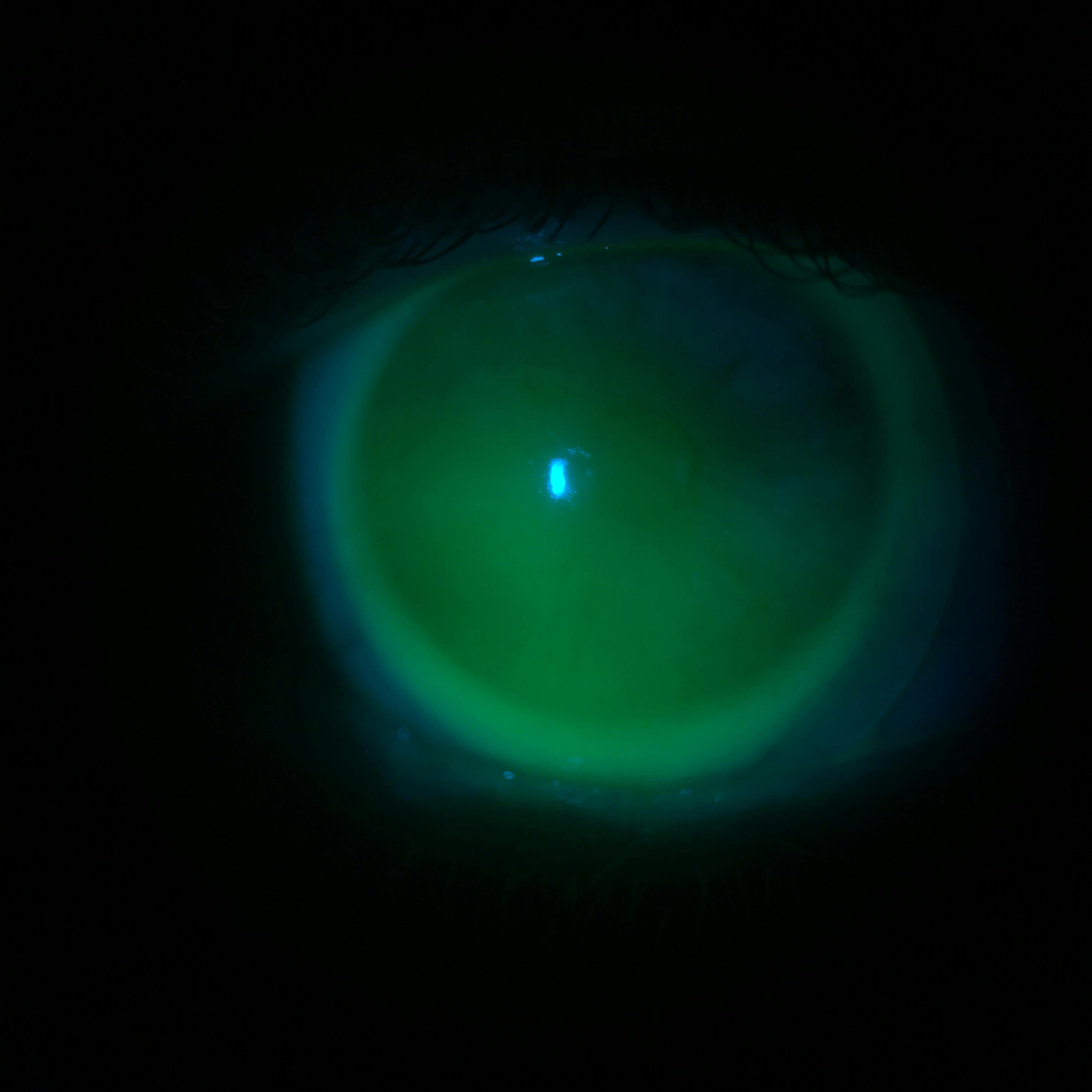
Figure 13 reveals how diffuse cobalt blue light can be used to observe any areas of contact between the back surface of a scleral lens and the cornea. In this image, there is minimal fluid or feather contact in the superior temporal area of the corneal and limbal area.
Figure 13
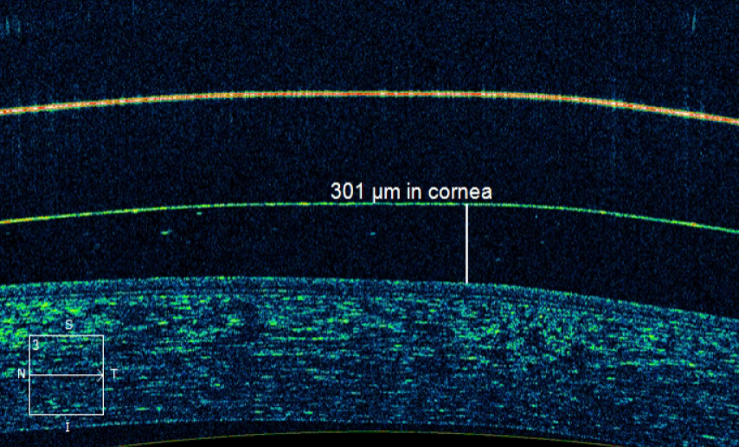
Figures 14-15 represent anterior segment optical coherence tomography (OCT) can be useful in highlighting and quantifying the number of microns of fluid clearance under a scleral lens. Figure 14 is using the ruler function of the OCT to depict the number of microns under the scleral lens.
Figure 14
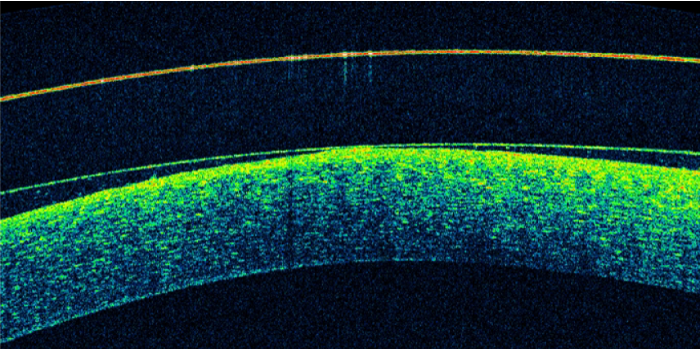
Figure 15 shows an area of contact between the posterior surface of the scleral lens and the cornea.
Figure 15
Once the appropriate trial lens is chosen based on optimal central vault, the next step is to ensure sufficient limbal clearance. Many lens designs allow for independent manipulation of the limbal curvatures (or transitional zones) in isolation and without affecting other parameters of the scleral lens design.
Lastly and perhaps most importantly, the landing zones should be carefully evaluated. The goal here is for the lens to land evenly on the surface of the sclera without excessive edge lift or compression. If there is evidence of either edge lift, vascular compression or lens edge bearing into the conjunctiva, the lens haptics need to be modified accordingly. Based on the scleral lens design, this can be accomplished using toric or quadrant-specific adjustments to the peripheral landing zones. The haptics are tightened when there is excessive edge lift and the haptics are loosened if there is conjunctival impingement or vascular compression causing blanching.
As we discussed earlier, patients with DED may benefit with the selection of larger scleral lens designs. These lens designs may require a more customized peripheral haptic design due to the increasing peripheral scleral lens toricity.12
Lens handling, care, and hygiene
Once the fitting process is completed, it can be quite exciting to dispense the lens to your patient, however thorough patient education and training on lens handling, application and removal processes, care and hygiene will be key to success. As you will experience, these patients require extensive and frequent ongoing management and education. If the patient is a previous contact lens wearer, emphasizing the scleral lens handling differences from both soft and corneal RGP contact lenses will better prepare them for what’s to come.
Application and removal
Given the larger diameter of the lens coupled with the need to preserve fluid in the scleral lens bowl during the application, the process of application and removal can represent a challenging task for some patients, especially those with reduced visual acuity or limited dexterity. Difficulty with lens application is a top reason for scleral lens drop-out14 therefore it is important to ensure that the patient feels comfortable with every step of the application and removal process. A scleral lens is typically applied using an application plunger and removed using a smaller removal plunger (Figure 16).
Figure 16
Alternatively, the patient can be taught to use their fingers for application and removal as well. For those patients that may have trouble with fixation or dexterity, there are numerous tools, such as light emitting stands or the ring applicator, that can assist with the application/removal process.
The Dalsey Adaptives See-GreenⓇTM Light Stand is a favorite in our clinic as the green light provides a target for fixation while the stand allows the use of both hands in maintaining eyelid control (Figure 17).
Figure 17
As mentioned above, preservative-free (PF) saline is used to fill the scleral lens bowl prior to lens application. It is necessary to emphasize the importance of using a non-preserved sterile saline solution for lens filling to avoid toxicity to the cornea; a point especially important for the patient with dry eye. Several options for PF saline are available on the market. Patients with DED may be sensitive to certain buffers in the saline solution. Non buffered sterile PF saline solutions indicated for scleral lens rinsing and filling may be the best option for these patients. 0.9% sodium chloride inhalation solution is used off-label for rinsing and filling and may be a good option for some patients.
Further, patients may find additional relief by using a viscous preservative free artificial tear combined with PF saline for scleral lens filling prior to application. A scleral lens filling solution with electrolytes mimicking the natural tear film has also worked well for our patients with DED.
When the lens is being applied on the eye, it is critical to avoid application bubbles under the lens. These bubbles represent areas of trapped air behind the lens and can ultimately lead to corneal desiccation which is a complication that should be avoided at all costs, especially for the patient with ocular surface disease. If an air bubble is found to be present, the lens should be removed, refilled with preservative-free saline and reapplied.
It is important to train your patients to look for these bubbles after every application. This point is especially important for beginners to scleral lens wear. With time and practice, the application bubbles will become less frequent.
Figure 18 illustrates a stagnant application bubble can lead to corneal desiccation in the area of the bubble. New scleral lens patients should all be trained to identify bubbles immediately after scleral lens application. An application bubble can be seen inferiorly in Figure 18.
Figure 18
Lens care
The lens is applied and removed daily and a thorough cleaning and disinfection is performed after every use. Proper scleral lens hygiene and care will be vital for patients with DED. Due to ocular surface instability and inflammation, their scleral lenses will be more prone to deposits.
- A gas permeable cleaner and disinfection system should be recommended for everyday use and storage overnight.
- Multipurpose RGP lens cleaners or hydrogen peroxide systems (especially for patients with preservative sensitivities) can be used as a daily cleanser and storage system.
- Manual rubbing with the solution for removal of deposits prior to overnight storage should be recommended.
An additional step such as an extra strength cleaner or an alcohol-based cleaner can be used biweekly in conjunction with the daily cleaner for patients with excessive lens deposits. Surface coatings, such as
Tangible Hydra-pegTM can help improve lens wettability, minimize friction, and reduce surface deposits. This coating does not last the lifetime of the lens and may require recoating.
Additionally, only approved solutions can be used for cleaning/disinfection when lenses are coated with Hydra-pegTM. Caution and close monitoring should be used when prescribing this coating as it may not be beneficial for every patient with ocular surface disease and in some cases, it may make deposits worse.
As you can imagine, entering the world of cleaning and care of scleral lenses can be overwhelming. Despite written handouts and instructions, from the patient’s perspective, it is easy to become confused when shopping for these products both online and in retail stores. Advise the patient to bring all of their products, including cleaners and filling solutions, with them to every follow up visit. This will align your recommendations with products they are actually using and will make troubleshooting more manageable.
Special considerations for scleral lenses and dry eye
Frequent follow up evaluations and thorough patient counseling and education are important elements for any specialty services being offered in your clinic, however they become extra important when managing patients with dry eye in scleral lenses. Setting expectations of the scleral lens fitting process, including the advanced handling, care, potential complications and more frequent follow up schedule is imperative for success with fitting scleral lenses. The first lens ordered may not be the last lens dispensed and the fitting process may require multiple adjustments.
Additionally, the application and removal process may require several visits before both you (the practitioner) and the patient feel comfortable enough to allow the patient to conduct the application and removal independently.
Patients with moderate to severe dry eye may encounter additional complications due to their underlying condition.
- Poor-lens wetting or front surface fogging can occur increasingly in patients with dry eye disease, especially those with severe dryness, exposure keratopathy, or other reasons for incomplete eyelid closure. Patients will complain of poor visual quality and decreased comfort. Oftentimes, a poor quality or quantity tear film is to blame. Improper spreading of moisture across the anterior surface of the scleral lens will leave the lens surface dry and desiccated. Further, patients with DED are more prone to secrete mucus, which can deposit on the front or back surface of the lens and can further exacerbate the wetting issues.
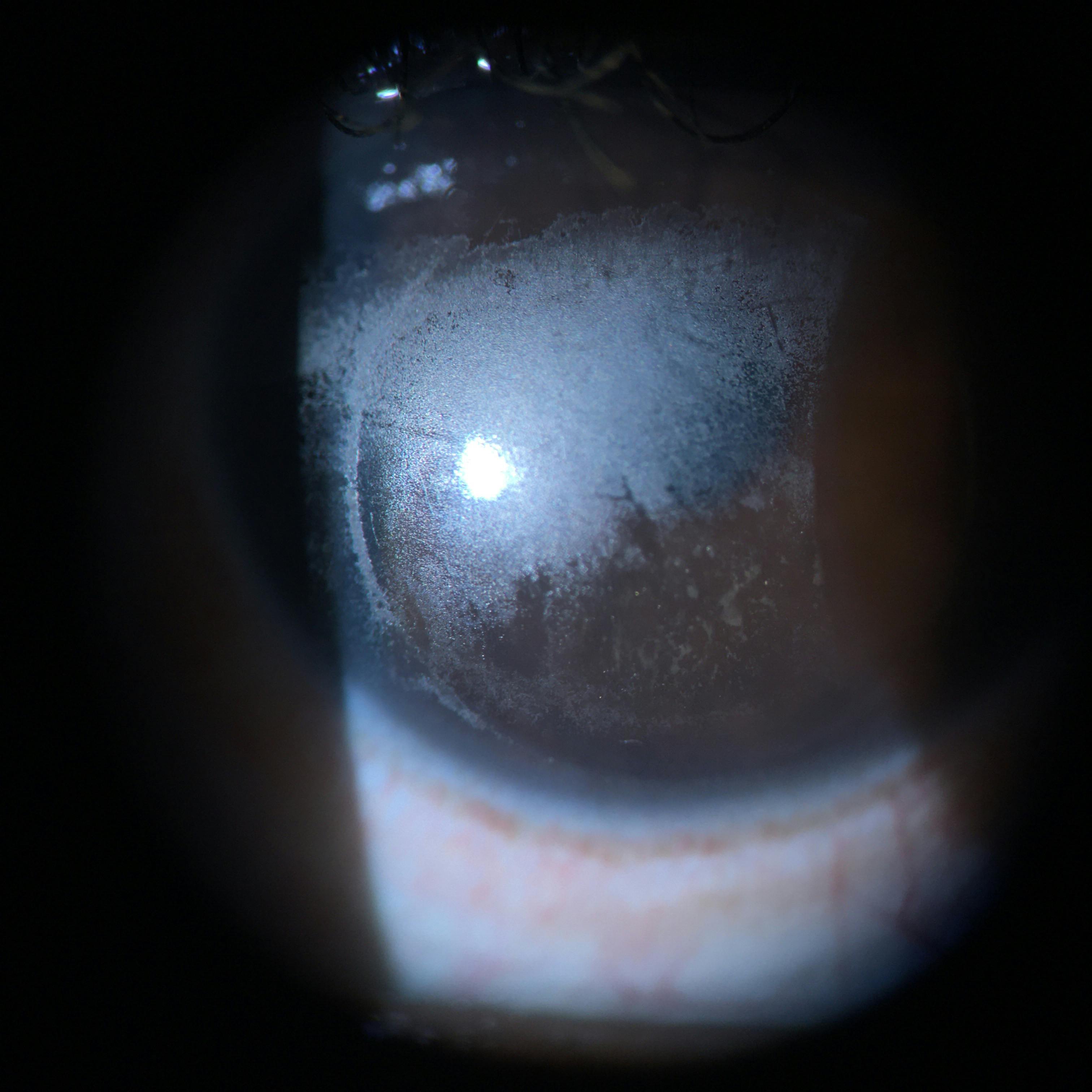
Figure 19 demonstrates poor anterior surface wetting of a scleral lens is a common complication for a patient with dry eye. The poor quality of the patient’s tear film leaves the anterior surface of the lens with poor wettability.
Figure 19
As Figure 20 illustrates, patients with dry eyes are more prone to secreting mucus, depositing these on the front and back surface (in the fluid chamber) of a scleral lens.
Figure 20
To manage this complication effectively, continue treating the underlying cause. Remember, scleral lenses will help with the symptoms of dry eye disease, however aggressive management of the underlying condition will serve as the key to success with scleral lenses. Therefore, appropriate step 1+2 TFOS DEWS II therapies (warm compresses, lid scrubs, topical lubricants etc. ) should be implemented or continued for these patients. Utilizing the most appropriate rigid lens material when designing the scleral lenses can help remedy these issues.
In addition, using surface treatments, such as plasma treatment or surface coatings can improve wettability and provide relief for some patients.
Lastly, do not discount the necessity of introducing an additional cleaning step, such as an alcohol-based cleaner (for lenses without surface coatings), in addition to the patient's regular cleaning solution and regimen. If the front surface fogging is occuring after several hours of lens wear, the patient can be instructed to remove the lenses midday, clean the lenses and reapply with fresh non-preserved saline. Frequent surface lubrication by applying artificial topical lubricants directly over the lens surface may also help with comfort and visual stability.
- Debris in tear-film or post lens tear reservoir fogging is another common complication that can occur with dry eye patients wearing scleral lenses. Excess debris from the tear film becomes trapped under the lens causing a decrease in vision and visual discomfort. Though both types of findings lead to similar patient complaints, post lens tear debris or reservoir fogging is different from front surface fogging described above. Each can be easily distinguished during a slit lamp examination or with anterior segment OCT.
In Figure 21, debris or post-lens tear reservoir fogging can be identified via slit lamp biomicroscopy using an optic section and focusing on the fluid layer under the scleral lens. In this image, the debris is the refractile dots under the scleral lens.
Figure 21
When presented with this finding, take a careful look at the peripheral edge alignment of the scleral lens and rule out any areas of edge lift. Any areas of edge lift will provide an entry point for the debris. Adding fluorescein dye after lens application can help identify areas of lift as the dye will enter the fluid reservoir via the area of the greatest edge lift. Anterior segment OCT can also be useful in assessing edge lift around the scleral lens.
If asymmetric edge lift is found, use toric or quadrant specific peripheral curves to align the haptics evenly around the sclera. This will improve patient reported comfort and may increase overall wearing time.15 If the central vault is excessive, decreasing central clearance can also remedy this issue. If all else fails, oftentimes, prescribing a more viscous non-preserved artificial lubricant in the lens bowl in conjunction with the non-preserved saline filling solution might just be the answer.
Lastly, keep in mind that the patient may ultimately need to remove, cleanse and reapply the lens midday on a regular basis as a solution to this complication. Once again, treating the underlying cause, usually MGD, will be key to combating any type of fogging experienced during scleral lens wear.
Conclusions
Patients wearing scleral lenses for dry eye have continued to report an improvement in their symptoms and functional vision. Wearing time can influence this outcome as scleral lens use during all waking hours (16h+) has shown to improve visual outcome.
16 Despite the
underlying cause of the dry eye disease, scleral lenses have consistently shown to provide benefits by improving patient symptoms and visual quality.
16-17Identifying the appropriate patient will be the first step in managing dry eye patients with scleral lenses. Achieving success with scleral lens management for the dry eye patient goes well beyond an appropriate scleral lens fit. Setting appropriate expectations at the consultation visit will provide a strong foundation for the scleral lens fitting process. Emphasizing an adjunctive therapeutic model will further contribute to success. Utilizing scleral lenses will not mean a discontinuation of previously prescribed dry eye therapy.
Aggressive and persistent management of the underlying cause of dry eye disease will impact the ultimate outcome for the patient.
Comanagement with optometry, ophthalmology and other healthcare physicians will serve as a cornerstone for ensuring success for a lot of the severe dry eye and
ocular surface disease patients stemming from systemic conditions. After the conclusion of the fitting, a summary letter of the outcome should be sent to the referring provider. Communication will lay a strong foundation for proper patient management and will allow for future collaborations.
Scleral lens management can be a complex and advanced process, however after a few successful fittings, it may prove to be one of the most rewarding aspects of the multitude of clinical care you provide to your patients. Scleral lenses have demonstrated efficacy in their therapeutic role in rehabilitating the ocular surface and relieving discomfort.
16-17 This dry eye disease solution has rightfully earned its place in
dry eye disease management.
Scleral lenses will certainly prove to be useful in your “dry eye toolbox” and when utilized for the appropriate patient will make all the difference.
References
- Ian J. Saldanha, Rebecca Petris, Matthew Makara, Prabjot Channa, Esen K. Akpek,Impact of the COVID-19 pandemic on eye strain and dry eye symptoms,The Ocular Surface,Volume 22,2021,Pages 38-46,ISSN 1542-0124.
- Nau, Cherie, Harthan, Jennifer, Shorter, Ellen, et al. Demographic Characteristics and Prescribing Patterns of Scleral Lens Fitters: The SCOPE Study. Eye Contact Lens. 2018;44:S265-S272.
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. The Ocular Surface. 2017;15(3):276-283.
- Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. The Ocular Surface. 2017;15(3):438-510.
- Foster JB, Lee WB. 3 - The Tear Film: Anatomy, Structure and Function. Ocular Surface Disease: Cornea, Conjunctiva and Tear Film. January 2013:17-21.
- Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. The Ocular Surface. 2017;15(3):575-628.
- Van der Worp E. A Guide to Scleral Lens Fitting. 2nd ed. Forest Grove, OR: Pacific University; 2015.
- Harthan JS, Shorter E. Therapeutic uses of scleral contact lenses for ocular surface disease: patient selection and special considerations. Clinical Optometry. 2018;ume 10:65-74.
- Levitt AE, Galor A, Weiss JS, et al. Chronic dry eye symptoms after LASIK: parallels and lessons to be learned from other persistent post-operative pain disorders. Mol Pain. 2015;11:21. Published 2015 Apr 21.
- Kornberg DL, Dou E, Wang Y, et al. Clinical experience with PROSE fitting: significance of diagnosis and age. Eye Contact Lens. 2016;42:124–128
- Barnett M, Courey C, Fadel D, et al. BCLA CLEAR - Scleral lenses. Contact Lens and Anterior Eye. 2021;44(2):270-288.
- Shorter, E., et al., Scleral Lenses in the Management of Corneal Irregularity and Ocular Surface Disease. Eye Contact Lens, 2018. 44(6): p. 372-378.
- Vincent SJ, Alonso-Caneiro D, Collins MJ. Optical coherence tomography and scleral contact lenses: clinical and research applications. Clin Exp Optom 2019; 102(3):224–41.
- Macedo-de-Araújo RJ, van der Worp E, González-Méijome JM. A one-year prospective study on scleral lens wear success. Cont Lens Anterior Eye. November 13, 2019.
- Visser ES, Visser R, Van Lier HJ. Advantages of toric scleral lenses. Optom Vis Sci. 2006;83:233–236.
- Bavinger JC, DeLoss K, Mian SI. Scleral lens use in dry eye syndrome. Current opinion in ophthalmology. 2015;26(4):319-324.
- Segal, O. , Barkana, Y. , Hourovitz, D. , Behrman, S. , Kamun, Y. , Avni, I. & Zadok, D. (2003). Scleral Contact Lenses May Help Where Other Modalities Fail. Cornea, 22 (4), 308-310.
- Fadel D. Scleral lens complications: their recognition, etiology, and management. Ontario, Canada: Dougmar Publishing Group; 2020. p. 337–8.
- Sonsino J, Mathe DS. Central vault in dry eye patients successfully wearing scleral lens. Optom Vis Sci. 2013;90(9):e248-251.
- Sindt CW, Longmuir RA. Contact lens strategies for the patient with dry eye. Ocul Surf. 2007;5(4):294-307.