


Approximately 3 million Americans are afflicted by glaucoma, a progressive and irreversible optic neuropathy characterized by loss of retinal nerve fiber layer tissue and visual field.1 Glaucoma is characterized by “cupping” of the optic nerve, which describes the loss of the neuroretinal rim.2 The visual field becomes compromised due to damage to the optic nerve. A major risk factor of glaucoma is increased intraocular pressure (typically an IOP of >24-30 mm Hg) due to increased aqueous production or decreased aqueous outflow.2
Additional glaucoma risk factors include positive family history, hypertension, and diabetes.2 It is important to note that some patients may have “glaucomatous optic nerve damage despite having IOPs in the normal range.”2 This form of glaucoma is known as normal or low tension glaucoma.
The ciliary body produces aqueous humor; its purpose is to provide nutrition to the eye as well as maintain the eye’s pressurized state. The buildup of aqueous humor can be due to overproduction by the ciliary body or decreased outflow via the eye’s trabecular meshwork. Present-day pharmacotherapy is directed towards reducing the production of aqueous humor at the ciliary body and increasing its outflow via the uveoscleral and trabecular meshwork pathways.2
Figure 1 illustrates the mechanisms of open-angle and closed-angle glaucoma.

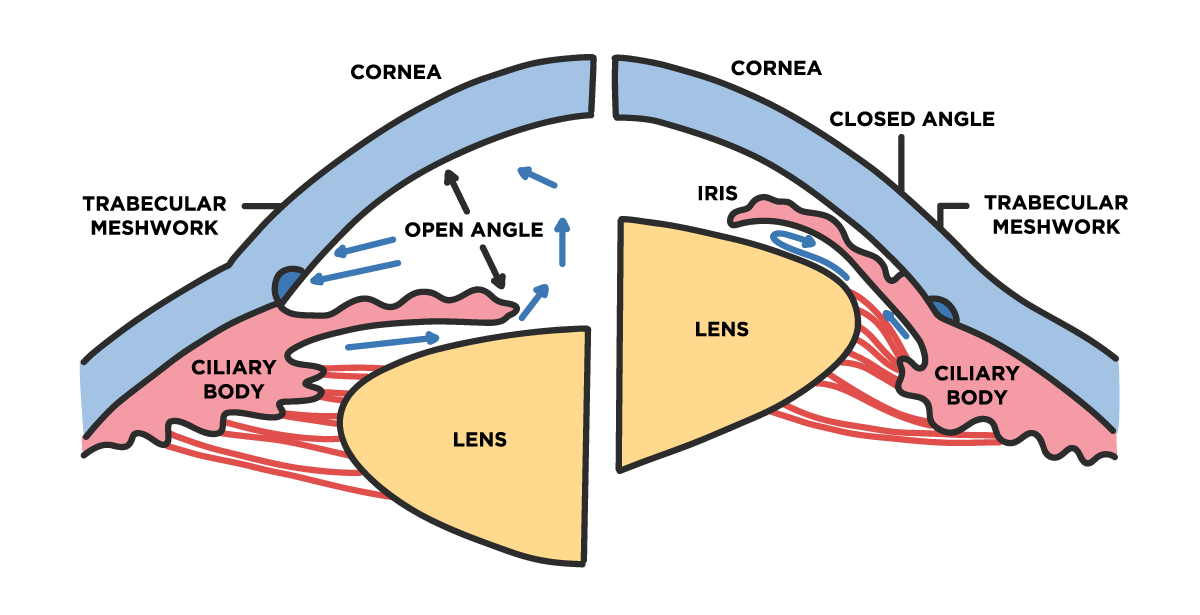
Figure 1: Adapted from NIH (3).
There are no cures for glaucoma; instead, primary management of the disease is based on reducing the intraocular pressure with glaucoma eye drops.2 With regularly scheduled visits to an ophthalmologist and adherence to an eyedrop regimen, patients with glaucoma may have very few limitations.
Here we will discuss the variety of pharmacologic eye drops available to manage glaucoma. We will dive into drug classes, pharmacodynamics, typical side effects, and physician-patient considerations when choosing a glaucoma drop.
Download the cheat sheet now!

Glaucoma Drops Cheat Sheet
This comprehensive cheat sheet outlines glaucoma drops along with their concentration, mechanisms, and contraindications.

A breakdown of glaucoma medications
Topical prostaglandin analogs
There are a variety of glaucoma medications, each with its respective class. The topical prostaglandin analogs include eye drops such as Latanoprost (Xalatan, Viatris, Canonsburg PA), Bimatoprost (Lumigan, Allergan, Parsippany NJ), and Travoprost (Travatan Z, Novartis, Cambridge MA).4 These medications reduce the IOP by increasing the outflow of the aqueous humor via the uveoscleral pathway.4
While these drugs may be used alone; they can also be paired with drops from other classes for a combinatory effect. An upside to these drops is that they are used once daily, which is highly convenient for patients. Potential ocular side effects include eyelash growth, darkening of the iris and periocular tissues, conjunctival hyperemia, and a foreign body sensation.4 Topical prostaglandin analogs may also exacerbate inflammation of the eye and are therefore not first-line for uveitis patients.4
Topical beta-adrenergic receptor antagonists
Another class of eyedrops includes topical beta-adrenergic receptor antagonists. The beta-receptor regulates the function of the sympathetic nervous system; by inhibiting these receptors located on the ciliary body, aqueous humor production is reduced. Common drops of this class include Timolol, Betimol (Oak Pharmaceuticals, Lake Forest, IL), and Carteolol.4
Because different types of beta receptors are found in the body; these drugs can cause systemic side effects, including bronchoconstriction and bradycardia.4 Thus, these eye drops are contraindicated in patients who suffer from pulmonary conditions such as asthma and chronic obstructive pulmonary disease (COPD).
Topical adrenergic-2 receptor agonists
Topical adrenergic-2 receptor agonists lower the IOP via a dual action: decreasing aqueous humor production and increasing drainage through the uveoscleral outflow.4 The alpha-2 receptor is responsible for inhibiting the sympathetic nervous system when activated. The typical drugs of this class include Brimonidine and Apraclonidine.4 Brimonidine is typically used in patients who cannot tolerate a beta-blocker.
Side effects may include a burning or stinging sensation when instilling the drop, conjunctival redness, and dry mouth. Apraclonidine has similar ocular side effects and a higher incidence of systemic effects, including bradycardia, decreased diastolic blood pressure, and insomnia.4 Currently, apraclonidine is typically reserved for patients who present with increased intraocular pressure after laser surgeries performed on the anterior segment (lens and iris) of the eye, such as cataract surgery.
It is important to note that this class of medications also has a higher incidence of contact ocular allergy and contact dermatitis, a major reason for discontinuation.
Topical carbonic anhydrase inhibitors
Topical carbonic anhydrase inhibitors include Brinzolamide and Dorzolamide; these drugs inhibit the carbonic enzyme anhydrase in the ciliary body’s epithelium to decrease the production aqueous humor.4 They may be used in conjunction with another glaucoma drop and are instilled 2 to 3 times daily.
Adverse effects include allergic reactions present in the conjunctiva and superficial punctate keratopathy.4 Patients may complain of a bitter aftertaste, which can be abated by performing punctal occlusion (pressing down on the lacrimal duct when instilling to drop to prevent it from seeping down the nose/throat and into the systemic circulation).
Topical direct-acting cholinergic agonists
Another class of drops includes the topical direct-acting cholinergic agonists, which can improve the intraocular pressure by increasing aqueous outflow via the trabecular meshwork.4 The eye drops of this class include Pilocarpine and Carbachol. They are prepared in two formulations, including a drop and gel form.
Like carbonic anhydrase inhibitors, these drugs are instilled several (2-4) times daily. Pilocarpine may cause corneal edema, an achy sensation, and ocular redness and should not be used in patients suffering from acute uveitis.4 Carbachol may be used if the patient does not respond to pilocarpine and has a duration of action of 4-6 hours, hence the multiple doses per day.
Through the continual development of glaucoma drops, there are now combination preparations, which reduce the number of drops a patient must instill each day to control their glaucoma (and improve patient compliance).4 Some of these preparations include Combigan, which is brimonidine and timolol (Allergan, Parsippany NJ), Cosopt, which is dorzolamide and timolol (Merck, Readington Township NJ), and Simbrinza, which is brinzolamide and brimonidine (Alcon, Fort Worth TX).4
These drops can usually be used just twice daily instead of having two separate medications, which would need to be used anywhere from 4-6 times a day.
Considerations when choosing glaucoma eye drops
Physicians should consult with their patients when selecting a glaucoma regimen best suited for them. Each patient requires an individualized therapy that provides the best possible outcome with the least likely toxicities. In addition, the progression of the disease must be taken into consideration, and the established target IOP.
Patients may be started on a single regimen or a combination of drops until the desired IOP is achieved. Adjuvant laser or surgical therapy may be warranted if glaucoma is not adequately controlled with medications alone.
Patients should be fully informed of eye drop side effects and be told to report any discomfort when using a particular drop to ensure compliance. Physicians must work with patients to establish the best possible regimen with many options available.
Don't forget to download our Glaucoma Drops Cheat Sheet!
References
- CDC. “Don't Let Glaucoma Steal Your Sight!” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 24 Nov. 2020.
- Henderer, Jeffrey D., and Christopher J. Rapuano. "Ocular Pharmacology." Goodman & Gilman's: The Pharmacological Basis of Therapeutics, 13e Eds. Laurence L. Brunton, et al. McGraw Hill, 2017.
- Krizaj , David. “What Is Glaucoma? - Webvision - NCBI Bookshelf.” National Library of Medicine , NIH , 30 May 2019, https://www.ncbi.nlm.nih.gov/books/NBK543075/.
- Riordan-Eva, Paul, et al. "Ophthalmic Therapeutics." Vaughan & Asbury's General Ophthalmology, 19e Eds. Paul Riordan-Eva, and James J. Augsburger. McGraw Hill, 2017.
- WebMD. “Combigan Ophthalmic (Eye): Uses, Side Effects, Interactions, Pictures, Warnings & Dosing.” WebMD, WebMD.
- WebMD . “Cosopt Ophthalmic (Eye): Uses, Side Effects, Interactions, Pictures, Warnings & Dosing.” WebMD, WebMD.
- WebMD . “Simbrinza Ophthalmic (Eye): Uses, Side Effects, Interactions, Pictures, Warnings & Dosing.” WebMD, WebMD.
