


As we are all too unfortunately aware, glaucoma is a silent killer of vision. It is the leading cause of irreversible blindness, affecting 5.7 million people in the US,1 and an estimated 76 million in the world. Unfortunately, these numbers are only expected to increase significantly, with a projected 111.8 million estimated to be affected in 2040.2
Glaucoma is typically marked by elevated intraocular pressure (IOP), which leads to progressive damage of the optic nerve and subsequent loss of vision. Generally, treatment is focused on controlling IOPs to minimize progressive vision loss.
Overview of glaucoma staging
In terms of staging glaucoma, mild-stage glaucoma is typically defined as early retinal nerve fiber layer changes without visual field abnormalities. Moderate-stage will also have retinal nerve fiber layer changes, plus visual field defects in one hemifield, but not within 5 degrees of fixation.
In advanced stages of glaucoma, there will be retinal nerve fiber layer changes, visual field defects in both hemifields, and/or vision loss within 5 degrees of fixation.
The shifting glaucoma treatment paradigm
Individual clinical scenarios will always dictate treatment plans; however, the historical treatment paradigm for many physicians treating glaucoma was typically to start off with drops, then proceed to laser when on maximum medical therapy, then follow incisional surgery when that failed.
However, even when these treatment methods are working at their best, they each have shortcomings that make them less than ideal. There can be a significant cost and time burden to the patient when it comes to drops. Further, many patients find it difficult to properly instill drops. There are also peaks and troughs of drop efficacy, as well as the potential for adverse reactions like ocular surface disease, allergic conjunctivitis, and atopic dermatitis, among many others.
Using selective laser trabeculoplasty to treat glaucoma
Selective laser trabeculoplasty (SLT) is sometimes considered after patients are on maximum medical therapy or some physicians will offer it as an option to patients who wish to forgo or minimize the amount of glaucoma drops they are on. Unfortunately, SLT does not adequately lower pressure in a significant amount of patients. Beyond this, when it does work, it typically only offers a modest drop in IOP, and the results typically only last for 2 to 3 years on average.
There is also the risk of reactivating uveitis and risk of pressure spikes. In modern times, incisional glaucoma surgery is typically thought of as the “last resort” when it comes to managing glaucoma. The IOPs are typically more labile, and the surgery itself is a much higher risk of morbidity, including significant vision loss due to hypotony, choroidal effusions, choroidal hemorrhages, and the lifetime infection risk with endophthalmitis.
The benefits of ab interno MIGS
Microinvasive glaucoma surgery (MIGS) has therefore become a very attractive option since its inception, as it offers many advantages. It has a high safety profile with a much lower risk of vision loss compared to incisional glaucoma surgery. Another benefit is that there is minimal disruption of normal anatomy, allowing for the option of further glaucoma surgery to be done on the same eye in the future.
Additionally, the ab interno trabeculectomy and trabeculotomy approach increases aqueous outflow via direct manipulation of the trabecular meshwork (TM) while inside the anterior chamber, creating a direct pathway from the anterior chamber to Schlemm’s canal and collector channels. The benefit of the ab interno approach is that it allows for direct visualization of the anatomic target.
It also allows for instant feedback on success, with the blanching of episcleral vessels in the patent collecting system. And when it is done successfully, it can offer significant IOP lowering and even get some patients off drops. It also offers more consistent IOPs, unlike topical medications. Additionally, it can be easier to manage by both the patient and physician, as it’s often done at the same time as cataract surgery with minimal additional downtime.
Tissue-preserving MIGS procedures
Tissue-preserving MIGS allows the surgeon to bypass the trabecular meshwork via a stent typically placed via an ab interno approach.
iStent
The iStent represents the “starter” MIGS for many anterior segment surgeons starting out in angle-based surgery. The latest generation is the Inject W, which employs two micro-bypass stents per injector, which is positioned flush into the trabecular meshwork before deploying and placed two to three clock hours apart through the main wound. It also has a wider flange for increased visibility.
Generally, this may see a more modest IOP reduction; however, you will also generally have less post-operative reflux, heme, and inflammation. This can be an advantage in patients on significant blood thinners.
Figure 1 is a still from a surgical video of a patient undergoing a MIGS procedure with the iStent device.


Figure 1: Courtesy of Nicole Bajic, MD
Hydrus
The Hydrus stent is an 8mm curved nitinol stent with alternative spines for structural support and windows for aqueous outflow and inserts into and dilates Schlemm’s canal. It is inserted via a second paracentesis, typically about 2 clock hours to the right of the main wound.
After placement of the stent, the inserter can be used backhanded at the end of the stent to adjust and ensure good placement. If further adjustment is needed, the stent can be removed and placed again downstream.
Figure 2 is a still from a surgical video of a patient undergoing a MIGS procedure with the Hydrus device.


Figure 2: Courtesy of Nicole Bajic, MD
XEN
The XEN gel stent can be done as both ab interno and ab externo but is typically implanted with its injector ab interno to create a low-lying bleb. This can be done via the main corneal wound, with the injector needle advancing just above TM, through the sclera into the subconjunctival space.
When deployed, only about 1mm of the implant remains in the anterior chamber. An early low-lying bleb gives instant feedback on the patency of the stent.
Tissue-destructive MIGS procedures
Trabectome
Trabectome is an ablative device that performs an ab interno trabeculotomy via electrocautery. This can be done via a clear corneal incision, and treatment can be tailored per the surgeon.
GATT
GATT is a trabeculotomy device done ab interno via the main corneal wound. After a goniotomy is created in the angle, a microcatheter is then threaded into Schlemm’s canal and advanced a full 360 degrees. After this is complete, traction is then placed on the microcatheter, completing the circumferential trabeculotomy.
Omni
The Omni is also an ab interno trabeculotomy device; however, the microcatheter is advanced 180 degrees prior to placing traction on the microcatheter to complete the trabeculotomy.
Some surgeons take advantage of this to “customize” their treatment for individual patients and may elect to only treat 180 degrees, or will complete the same maneuver on the other 180 degrees. Instead of this, some surgeons may elect to do a stent instead on the opposite 180 degrees. The key to success for ab interno trabeculotomies is to thread the catheter initially in the ideal position.
Figure 3 is a still from a surgical video of a patient undergoing a MIGS procedure with the Omni.

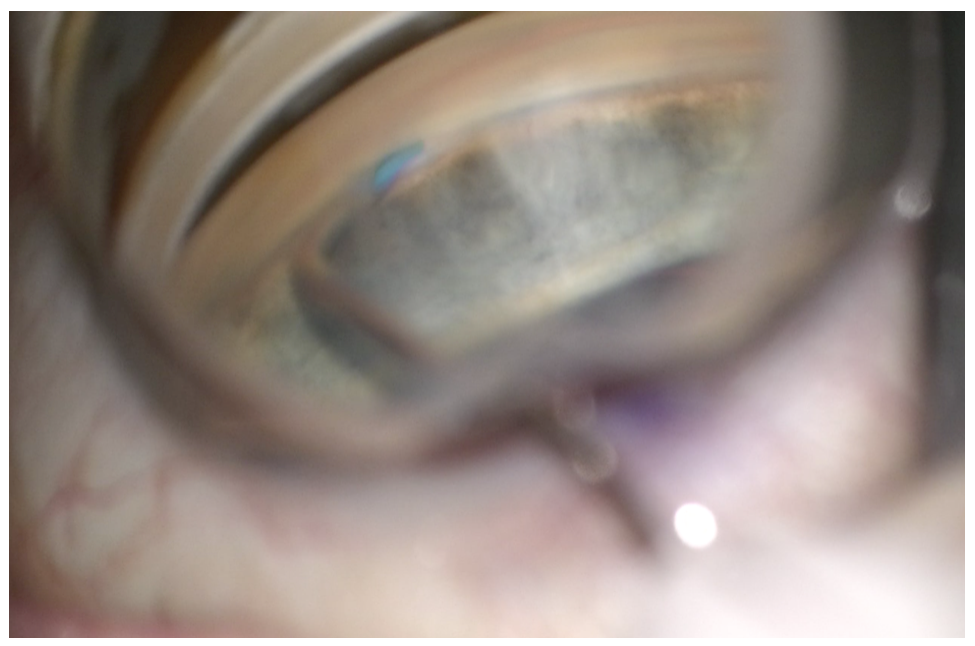
Figure 3: Courtesy of Nicole Bajic, MD
Ab Interno Canaloplasty (ABiC)
ABiC uses the iTrack microcatheter device. It can be done through the main corneal wound. After a nasal goniotomy is done, the microcatheter is advanced 360 degrees to allow for viscodilation of the canal and outflow system.
Goniotomy
The Kahook Dual Blade (KDB) performs a nasal goniotomy through the main corneal wound with a specially designed bevel blade. First, the trabecular meshwork is pierced with the tip, then the heel of the blade is leveled flush with the canal with a sweeping forehand motion to extend two to three clock hours.
The trabecular meshwork will scroll up, and there is no need to remove it. This can be repeated backhand. One benefit is that it is indicated for many types of glaucoma as well as ocular hypertension. It can also be done as a standalone procedure, so patients who are already pseudophakic can still be offered this procedure if needed.
Figure 4 is a still from a surgical video of a patient undergoing a MIGS procedure with the Kahook Dual Blade.

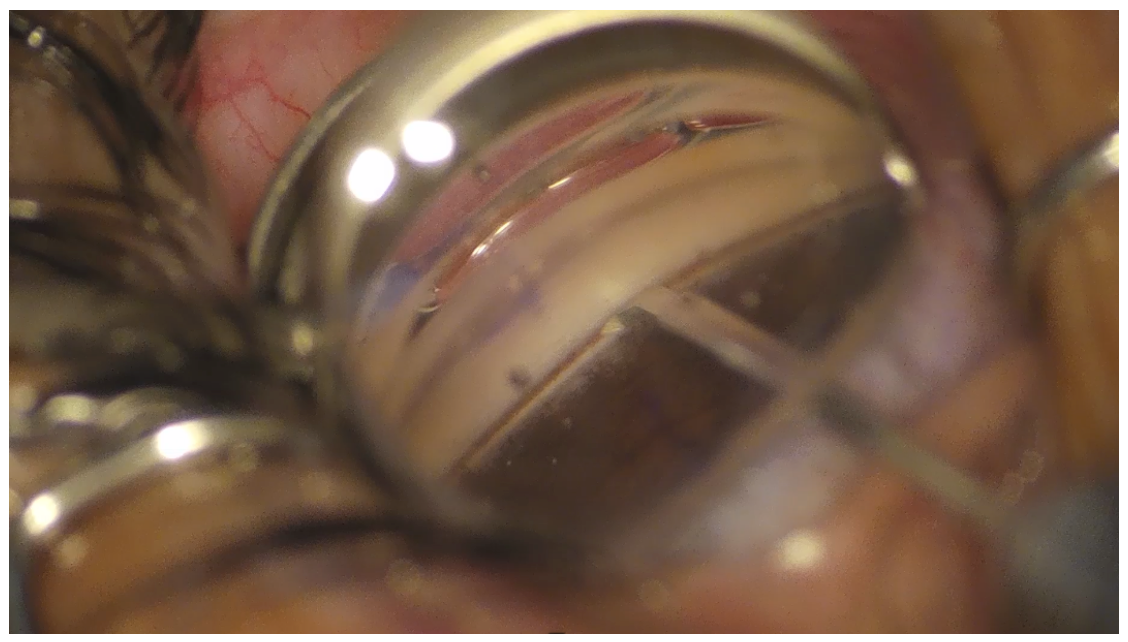
Figure 4: Courtesy of Nicole Bajic, MD
Endocyclophotocoagulation (ECP)
In ECP, an endoscopic laser probe is inserted through a clear corneal incision. The ciliary body is identified and directly ablated.
Surgical pearls for ab interno MIGS procedures
Appropriate patient selection is key to success for MIGS procedures. Gonioscopy must be done preoperatively, and angle structures should be easily visible. Further, other patient factors that can make positioning challenging are kyphosis, deep-set orbits, or lids with small fissures.
Intraoperatively, do not tape the head or use wrist rests. Visualization is the most important, and when it’s time for the MIGS procedure, you will want to tilt the microscope and patient’s head 35 degrees away. You will also need to lower the chair height and move the oculars up to adjust your view. Take care to ensure no pressure is placed on the cornea, which can cause striae and limit your view. You may consider using trypan and doing the MIGS prior to phacoemulsification to improve the view.
Some surgeons prefer performing MIGS after phacoemulsification, as the angle is deeper, and there is also often heme in Schlemm’s canal which also aids in visualization. Surgical follow-up depends on the clinical scenario; however, for the vast majority of routine MIGS cases, it typically doesn’t require more post-operative visits than the standard cataract surgery. IOP should be followed and managed as appropriate.
Figure 5 is a still from a surgical video depicting an up-close visualization of the angle.

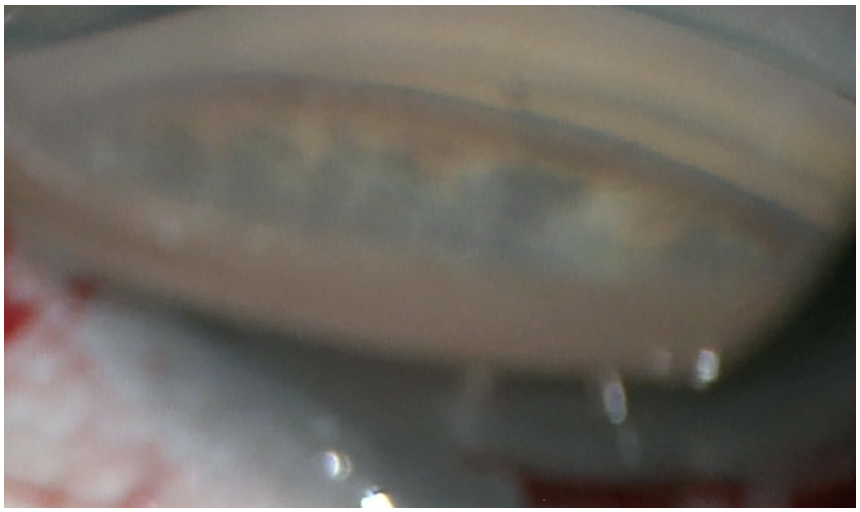
Figure 5: Courtesy of Nicole Bajic, MD
Figure 6 is a still from a surgical video showing blood in the Schlemm's canal, with deep-angle visualization secondary to MIGS combined with cataract extraction.

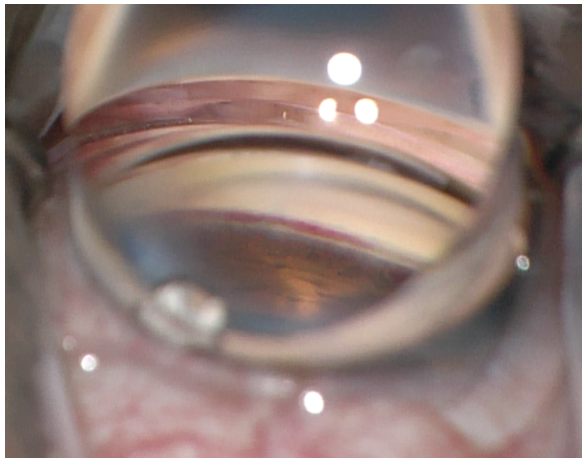
Figure 6: Courtesy of Nicole Bajic, MD
What's on the horizon?
MIGS is an exciting area within ophthalmology, as it seems there is constantly something new in the pipeline. Streamline Surgical System is a new implant-free and tissue-preserving device that dilates outflow channels via the delivery of small amounts of viscoelastic into Schlemm’s canal. It remains to be seen what role it will play in many surgeon’s toolbox in the treatment of glaucoma and ocular hypertension.
Regardless, we are fortunate to serve patients in an era with many fantastic MIGS options, with some surgeons considering it becoming a new standard of care. If a patient has glaucoma, needs cataract surgery, and is a good candidate for MIGS, they should be either offered MIGS by the surgeon themselves or referred to a colleague that is comfortable performing MIGS.
