


This article offers a point-by-point, case-based discussion on non-arteritic anterior ischemic optic neuropathy (NAION). We will go over the typical clinical presentation, investigation, differential diagnosis, and management of this condition.
NAION can be described as a “stroke of the optic nerve” confined to the optic nerve head, thus not involving the retrobulbar optic nerve. Oxygen supply to the optic disc is reduced when the designated blood flow is restricted. The oxygen-deprived cells may suffer irreversible damage.
Etiology of NAION
The posterior ciliary arteries (PCA) are the primary source of blood supply to the optic nerve head and surrounding retrolaminar cells.1 The short PCA branch from the ophthalmic artery as it crosses the retrobulbar optic nerve. These short PCA form a network as they divide into more branches, surrounding the optic nerve and the short ciliary nerves.
“They supply the choroid, up to the equator, after piercing through the sclera at the entrance of the optic nerve.”
Some branches form the circle of Zinn around the optic disc, while others link with the long PCA, the anterior ciliary arteries, and the arterial circle of the iris.1,2,3 NAION pathogenesis is described by the occlusion of these short PCA, resulting in partial or total ischemia of the optic nerve head. Consequently, the corresponding retinal ganglion cells may suffer from apoptosis.4,5
What causes the restricted blood flow?
The pathophysiology that causes insufficient blood flow to the laminar and prelaminar regions is considered controversial.1,3
Poor blood circulation is commonly believed to be caused by the following:
- A “compartment syndrome” of the optic disc, whereby mechanical crowding obstructs blood flow to the nerve fiber layer, and axonal edema arises.6
- Dysfunction of auto-blood-regulation.5
- Nocturnal hypotension causes reduced blood supply.4
Case report: initial consultation
A distressed 50-year-old male patient presents to your clinic for an urgent consultation on the same day as the onset of his visual symptoms. The patient’s general health background includes hypertension, high cholesterol, and the use of a blood thinner. He came in for acute superior vision loss in the left eye that onset in the morning, though he woke up with normal vision. No pain was reported. The patient previously had a corneal laser refractive surgery, uses +1.50 readers, and did not have a family history of ocular disease.
Clinical results recorded at the initial consult:
- Unaided visual acuity
- OD: 20/20
- OS: 20/132 (estimated, poor motivation)
- Auto-refraction
- OD: -0.50/-0.75x3
- OS: -0.50/-1.25x20
- Handheld intraocular pressure (IOP)
- OD: 15mmHg
- OS: 15mmHg
A relative afferent pupillary defect (RAPD) was noted OS, and the anterior segment looked normal OU. While the posterior segment looked normal OD, mild optic disc edema was observed OS. Additionally, an MRI revealed asymptomatic incidental findings of a large posterior fossa arachnoid cyst and minimal ethmoid inflammatory changes unrelated to visual field (VF) loss. A blood work-up showed normal results for the erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), and platelet count.
Figures 1 and 2 are fundus imaging of the patient’s right and left eye, respectively.

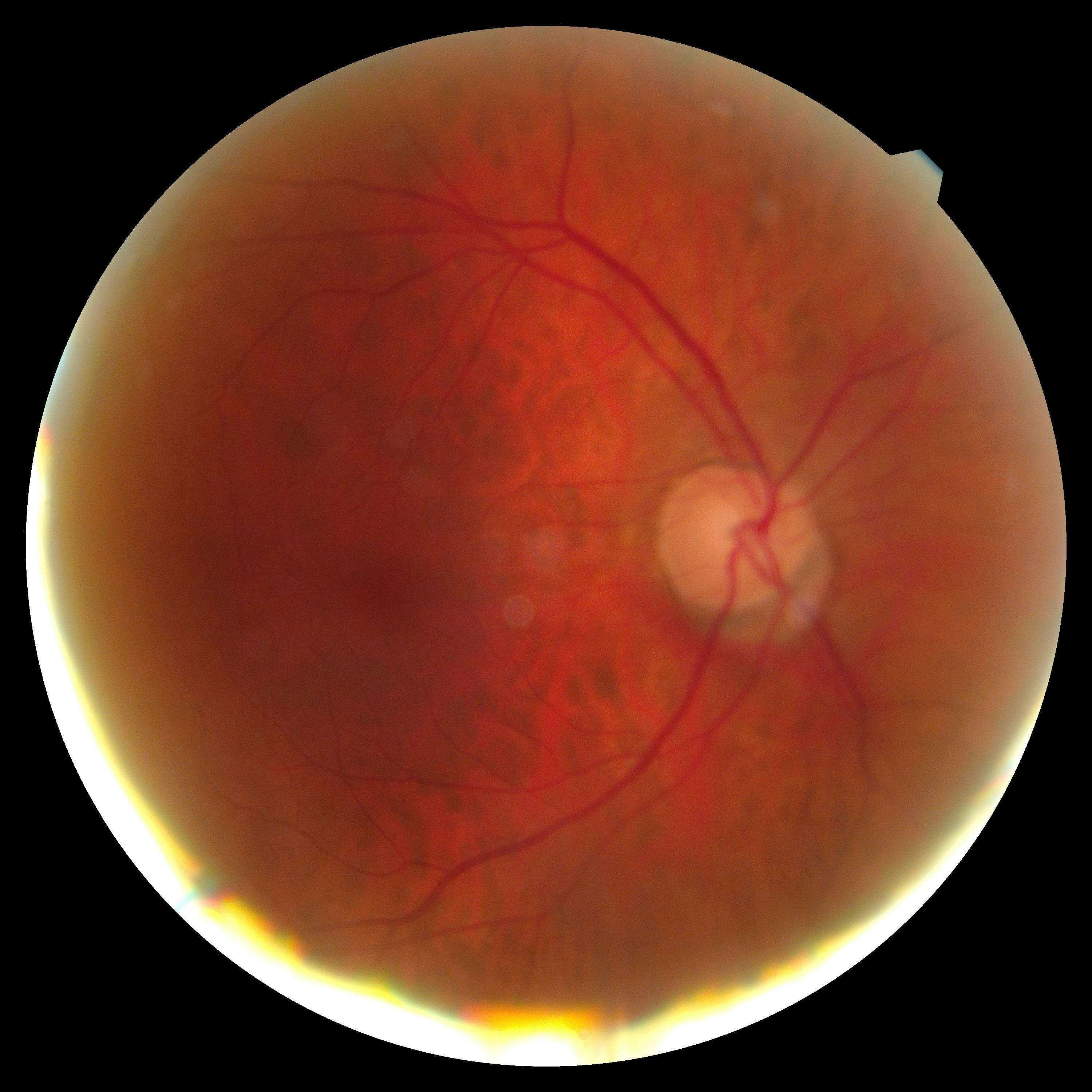
Figure 1: Image courtesy of Chantél Neethling, OD

Figure 2: Image courtesy of Chantél Neethling, OD
Symptoms of NAION
This patient presents with painless, sudden onset, unilateral reduced visual acuity, and unilateral arcuate visual field loss. Distinguishing symptoms of NAION include moderate visual loss, acute onset, and painlessness; also, it may initially be unilateral but eventually become bilateral.4,7,8
Typical NAION patient profile
This case portrays a typical patient profile for someone in the 40 to 70 year age group. Younger patients should not be excluded, especially if the contralateral eye presents with a crowded optic disc, as a small cup-disc ratio of less than 0.3 is identified as a “disc at risk.”4,5,7 The patient reports being hypertensive and having hyperlipidemia, fitting the profile of systemic health risk factors.4,7
Other associated risk factors may include:
- Diabetes4,7
- Arteriosclerosis7
- Anemia7
- Hyperhomocysteinemia4,7
- Collagen vascular disease4
- Acute blood loss5
- Antiphospholipid antibody syndrome4
- Carotid disease8
- Sleep apnea4,7
- Nocturnal hypotension
- Commonly visual loss is discovered upon awakening4,7
- Smoking8
- The use of some medications for erectile dysfunction4,7
Case report: 5-day follow-up
Five days after prescribing oral prednisone, the patient returned with no other ocular complaints and reported stabilization in superior visual field loss OS.
Clinical results recorded at the 5-day follow-up:
- Unaided VA
- OD: 20/20
- OS: 20/25
- Hertel exophthalmometer
- No proptosis
There was subtle RAPD noted OS, and the anterior and posterior segment results were the same as the initial consultation. Further investigation was suggested for a chest X-ray to rule out tuberculosis and blood tests to rule out syphilis and sleep apnea.
Figure 3 is fundus imaging taken at the 5-day follow-up appointment showing NAION in the patient’s left eye.
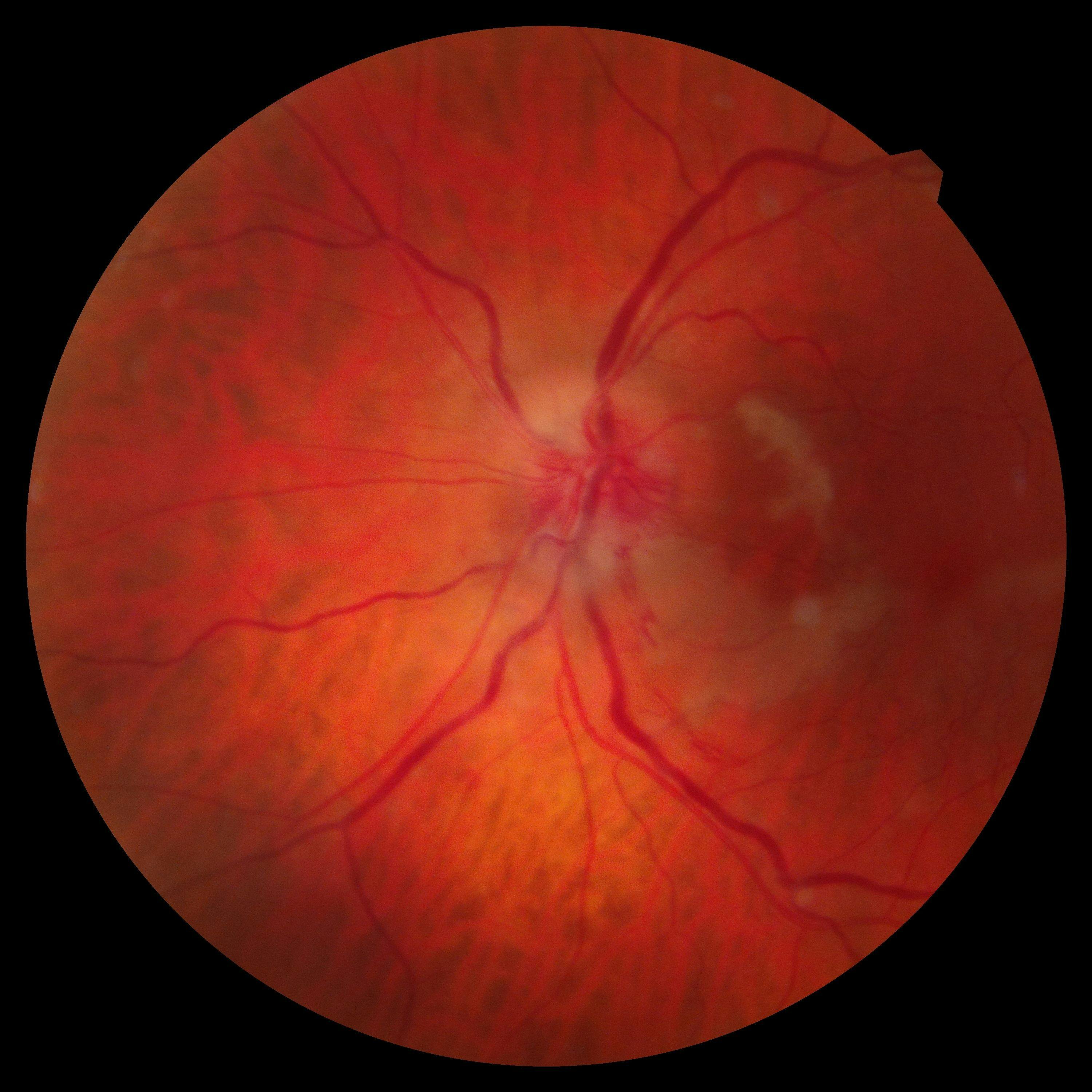
Figure 3: Image courtesy of Chantél Neethling, OD
Figure 4 compares optical coherence tomography scans showing optic nerve hypoplasia in the patient’s left eye.

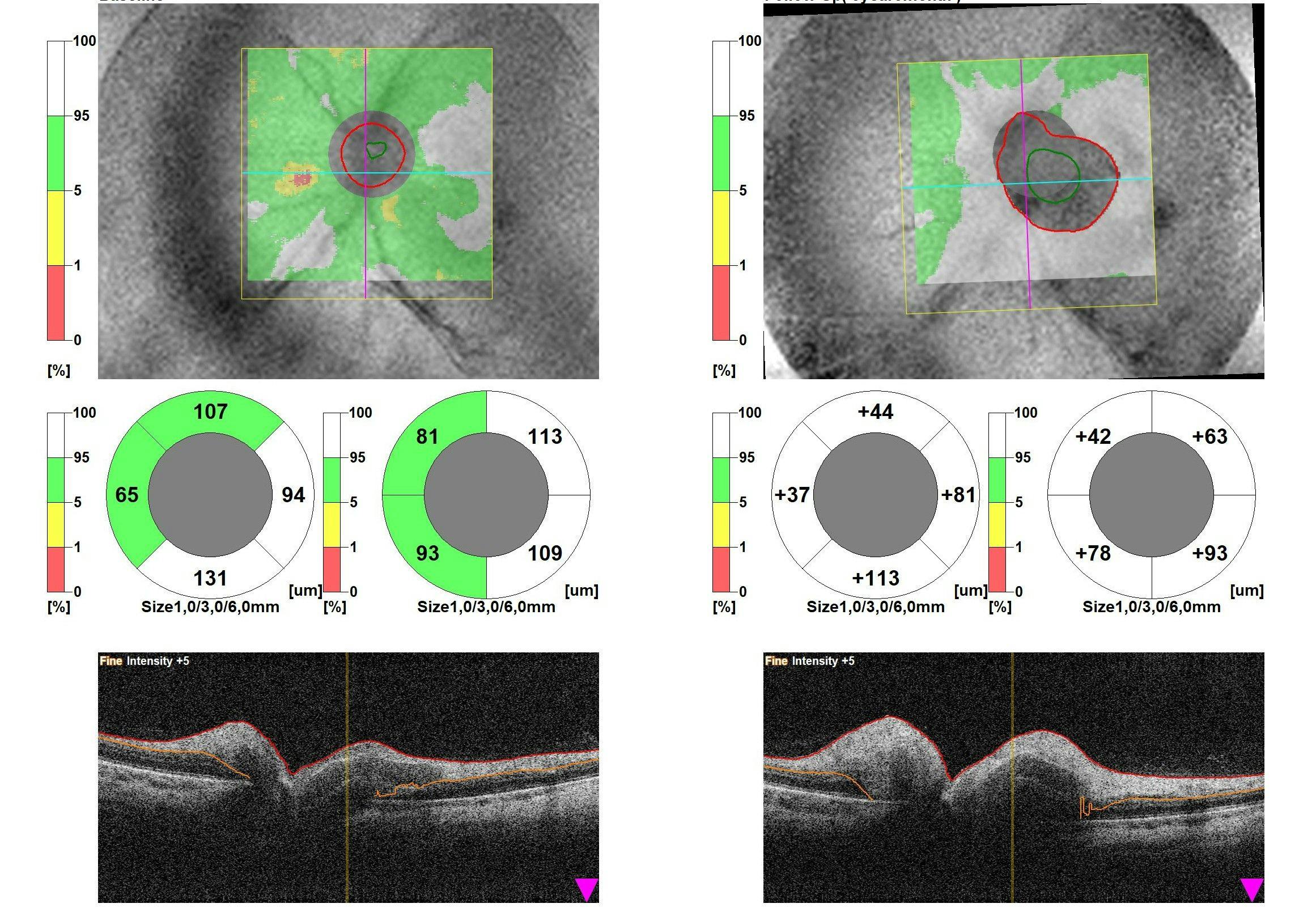
Figure 4: Image courtesy of Chantél Neethling, OD
Clinical signs and presentations
In this case report, the following ocular vitals and recordings support the diagnosis of NAION.
- Visual acuity: Most patients will have some degree of reduced visual acuity, which could vary greatly from 20/200 to 20/64 or better.4,9
- Pupils: A RAPD is expected on the involved side.5,8
- Optic disc edema: The swelling may be diffused or sectorial with accompanying peripapillary splinter hemorrhages.4,5
- Visual fields:
- The visual field loss will correspond to the anterior visual pathway (pre-chiasmic).5
- An inferior altitudinal defect is common, resulting from the anatomical superior and inferior portions of the circle of Zinn. The superior portion is more often affected with no definitive scientific explanation.2
- Conversely, the defect may be central, paracentral, quadrant specific, or arcuate.4,5
- Blood results: Check for normal ESR, CRP, and platelet count.
- Note: Inflammatory markers are essential to rule out life-threatening giant cell arteritis (GCA) that will present with a differential diagnosis of arteritic anterior ischemic optic neuropathy (AAION).4,7
- MRI of brain and orbits: No contributing comments.
- Note: Neuro-imaging is essential to rule out compressive lesions, even so in previously undiagnosed episodes of NAION, which present with optic disc pallor and corresponding visual field loss.4,7
Another investigation that may aid in establishing an accurate diagnosis is testing the patient’s color vision, as dyschromatopsia is proportional to visual loss.4,5
Differential diagnosis of NAION
Other optic nerve pathologies that may present similar clinical findings need to be ruled out. Below are some important distinguishing factors for optic neuritis, AAION, and PION.
Optic neuritis
Optic neuritis usually occurs in younger age groups,7 and is associated with painful eye movements.8 Also, dyschromatopsia may present as severe with only mild visual loss.4
Arteritic anterior ischemic optic neuropathy
AAION, which is caused by giant cell arteritis (inflammatory),4 has similar ocular signs and symptoms to NAION but with accompanying systemic symptoms. These include headache, jaw claudication, temporal scalp tenderness, proximal muscle and joint aches, and/or fever.7 Patients also tend to present with elevated ESR, CRP, and platelet count.7 With AAION, visual loss is more severe, often to the degree of finger counting or even worse.4,7
Posterior ischemic optic neuropathy
PION is much rarer, and involves ischemia of the retrobulbar optic nerve, usually without optic disc edema.8 It is not associated with crowded optic discs.4
Management of NAION
To date, no confirmed treatment has been proven effective for NAION.6 However, there are management strategies that can aid in getting a better prognosis.
1) Manage underlying risk factors
First is managing the underlying known risk factors.4 It’s important to note that in this case report, the patient’s hypertension and cholesterol should be well-controlled with routine vital evaluation, lifestyle adjustments, and medicinal treatment.
2) Refer to an internist
Next, refer to an internist to rule out vascular complications and sleep apnea.7 If nocturnal hypotension is the culprit, the patient should avoid hypertensive medication before bedtime.7
3) Medications
Prescribing anticoagulants or antiplatelets can reduce clotting vascular events,4,8 but to date; it has not been proven to reduce the chance of recurrence of fellow eye involvement.6 Our patient reported that he was already using a blood thinner. Corticosteroids may reduce edema but adversely have other steroid-related complications. On top of that, controversy exists on whether or not corticosteroids support visual restoration.5,6 Intravenous or intravitreal erythropoietin efficacy is still being questioned.6
Setting NAION treatment expectations
The patient needs to be counseled on a realistic visual outcome expectation upon spontaneous recovery, as the visual acuity may initially worsen 2 weeks after onset. Generally, the optic nerve edema may settle within 3 to 6 weeks of onset, with residual optic disc pallor (atrophy) at the area of infarction.
Therefore, visual acuity may restore within 2 to 3 months, to possibly 20/30 or better, but rarely back to “normal.” Assuring no further visual loss should be experienced, as long as there is no recurring episode or fellow eye involvement.4,5,10
Patient education on risk factors
Risk factor management should be judged case-by-case, considering the risk-benefit ratio and side-effect profile. Patients should be informed about the available management options but also their current lack of definitive efficacy.
This way, they are equipped with the necessary knowledge to give treatment consent if so desired. Educate your patients on timely reporting upon a repeat of this unfortunate neuro-ophthalmological event.
Conclusion
NAION continues to be an oculo-neurological complication that requires ongoing research to identify how to protect the optic nerve against damage and restore vision. Until an identified, trialed, and proven treatment protocol is established, NAION is best managed by accurately identifying and controlling the involved risk factors and by ruling out AAION.
