


Acute corneal hydrops is a known but rare complication of ectatic corneal disorders such as keratoconus (KCN).1 Although the pathogenesis of acute corneal hydrops is not fully understood, it is believed that a break in the Descemet’s layer is the leading cause.1 Such a break allows aqueous humor to penetrate the corneal stroma, resulting in bullous edema of the overlying corneal layers.1,2 The prevalence of acute corneal hydrops in patients with keratoconus is approximated at 2.6-2.8%.2
Most acute corneal hydrops resolve spontaneously within 2 to 6 months; however, this can vary depending on the severity of the edema and break in Descemet’s.1–4 Younger patients also have been reported to have slower healing.5 The duration of corneal edema is proportional to increased complications which may include infection, perforation, and corneal neovascularization.1,2
Case report: Cornea hydrop
A 22-year-old Hispanic male with a history of severe and progressive keratoconus (KCN) was referred for scleral lens evaluation with complaints of poor comfort and vision with their habitual scleral lenses in both eyes. Entering best corrected visual acuity was 20/125 with pinhole to 20/60 for the right eye and 20/60 with pinhole to 20/30 for the left eye. Uncorrected visual acuity was count fingers for each eye.
He continued with average daily wear time (AWT) of 18 hours. Habitual scleral lens parameters including design and diameter were unknown. Clinical examination revealed tight fitting decentered scleral lenses with apical corneal touch which left an impression ring upon lens removal for both eyes (Figure 1).
There was also notable conjunctival hyperemia for both eyes. Other clinical findings were consistent with advanced KCN with associated corneal steepening, thinning, striae, Fleischer ring, and apical subepithelial haze for both eyes. The patient had no prior history of corneal cross linking (CXL) as he was deemed a noncandidate due to severely thin corneas (Figure 2). Posterior segment findings were normal for both eyes at the patient’s most recent dilated fundus examination.
In Figure 1, below, diffuse white light slit lamp images under low magnification for the right and left eye immediately upon habitual scleral lens removal. The impression ring on the conjunctiva and conjunctival hyperemia are consistent with tight fitting and poorly functioning scleral lenses. Mild apical corneal haze can be appreciated for both eyes as well.

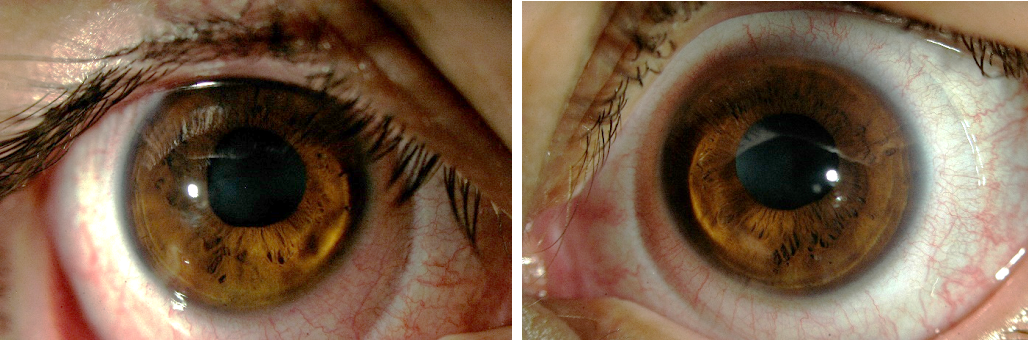
Figure 1: right and left eye slit lamp image.
Figure 2 of corneal topography (Pentacam, Germany) scans demonstrates the front axial curvature (top) and corneal thickness (bottom) for both eyes at baseline. The right eye Kmax value was 82.6D, with the thinnest location measuring 140 microns. The left eye (B) Kmax value was 90.1D, with the thinnest location measuring 135 microns.

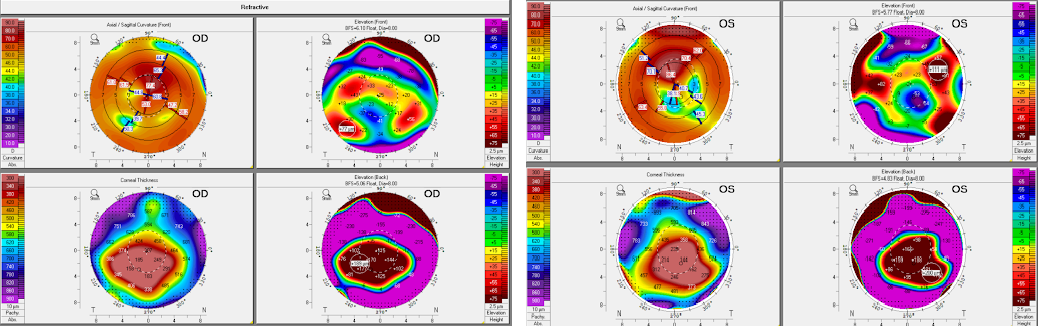
Figure 2: right and left eye corneal topography.
The patient underwent scleral lens refitting for both eyes to improve fit and vision. With his optimized new scleral lenses, his BCVA was 20/50 with pinhole to 20/40 in the right eye and 20/60 with pinhole to 20/30 in the left eye. The patient continued with scleral lens wear and was doing well with lens wear at the two-week follow-up visit.
One-month later, the patient presented for evaluation with complaints of extreme light sensitivity and poor vision in the left eye. He continued comfortably with scleral lens wear for the right eye with stable BCVA of 20/50. His entering uncorrected visual acuity (UCVA) was hand motion without improvement with pinhole for his left eye. Clinical examination revealed stable corneal findings for the right eye and an acute corneal hydrop in the left eye (Figure 3).
Figure 3 shows a slit-lamp diffuse white light image with medium magnification (A) of the left eye at presentation with acute corneal hydrop.

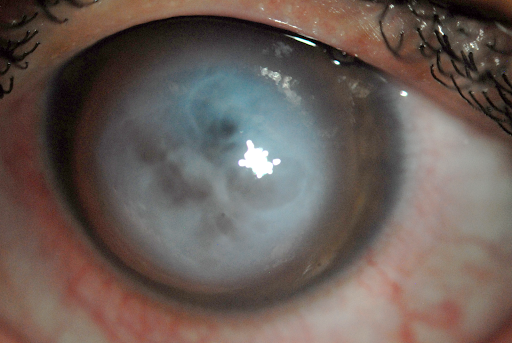
Figure 3
In Figure 4, there is significant corneal edema, which can be visualized in the anterior segment optical coherence tomography (OCT).

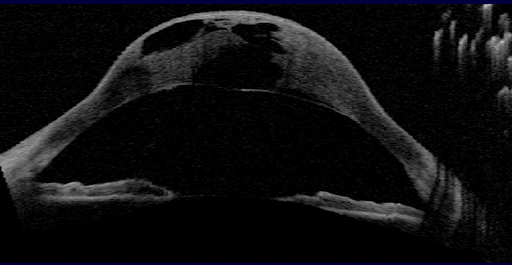
Figure 4
The patient was advised to discontinue scleral lens wear for the left eye and to start cycloplentolate 0.5% twice daily for comfort and Muro 125 ointment every 4 to 6 hours in the left eye for the corneal edema. The patient continued to be monitored over the next several weeks with tapering of topical medications and, by 8 weeks, the hydrop had completely resolved. No ophthalmic steroids or surgical intervention were undertaken for corneal healing.
Entering UCVA was 20/125 with pinhole to 20/30. There was subsequent increased corneal scarring and corneal thickening (Figures 5-7). The significant improvement in UCVA was also due to drastic corneal flattening following corneal healing (Figure 7). A scleral lens refitting was initiated and the patient’s BCVA improved to 20/25, which was superior to BCVA in recent years with prior optimized scleral lenses.
The patient resumed daily scleral lens wear for the left eye with adequate tolerance and stable vision. The patient avoided corneal transplantation and had no plans to pursue surgical intervention.
Figure 5 represents a slit lamp diffuse white light image in low magnification of the left eye following resolution of acute corneal hydrop.

Figure 5
Figure 6 shows the corresponding high resolution anterior segment OCT showing residual descemet’s scarring in area of initial break.

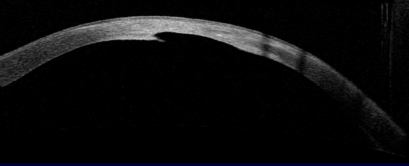
Figure 6
In Figure 7, a corneal topography (Pentacam, Germany) scan demonstrates the front axial curvature (top) and corneal thickness (bottom) for the left eye following resolution of corneal hydrop. The Kmax value was 53.3D, with the thinnest location measuring 353 microns.

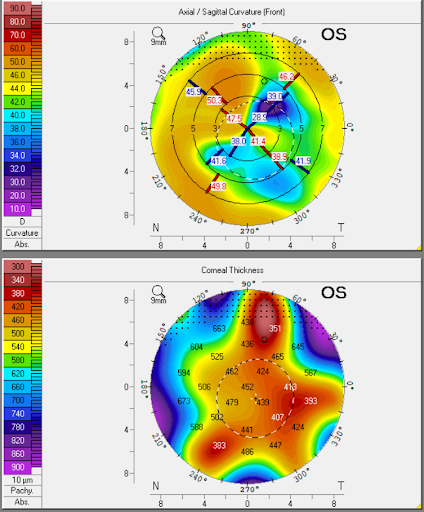
Figure 7
Treatment protocol for corneal hydrops
Treatment for acute corneal hydrops aims to reduce pain and reduce inflammation to prevent further complications. Surgical treatments including the use of intracameral air/gas injection or compression corneal sutures may be considered in the healing process of an acute corneal hydrop.2 In cases where vision potential is limited following recovery of an acute corneal hydrop, a penetrating keratoplasty (PKP) may be considered.2,6
It is reported that up to 60% of eyes may need PKP for visual rehabilitation once edema has resolved following acute corneal hydrops.6 It is also reported that prior history of corneal hydrop poses an increased risk of allograft rejection after PKP.3
Patients who experience acute corneal hydrops should be monitored periodically while awaiting resolution to assess the vision potential as secondary scarring may result in corneal flattening which can improve contact lens fitting endpoints and even vision.3 Considerable corneal flattening followed resolution of an acute corneal hydrop has been reported to improve vision in patients.1,3,6
In this case, the patient experienced nearly forty diopters of corneal flattening with 150 microns increase in corneal thickening. Despite the significant residual corneal scarring following resolution of the hydrop, the patient’s UCVA and BCVA both improved relative to baseline and with scleral lens wear pre-hydrop.
There is little literature to support the application of scleral lenses or other specialty contact lenses following resolution of acute corneal hydrops. Kreps et al studied patients who were successfully fit with scleral lenses following acute corneal hydrops. In their study, 68.8% of patients were successfully fit with scleral lenses following resolution of corneal hydrops. Only 18.8% of patients underwent PKP following resolution of acute corneal hydrops, which is significantly less than the reported 60% of patients in literature.4 The patients who did proceed with PKP did so because of limited visual acuity with scleral lenses.
Conclusion
In this case, a young habitual scleral lens wearing patient experiences a severe acute corneal hydrop. There was resolution of the hydrop following 8 weeks from initial onset, and no surgical intervention was undertaken. The patient’s uncorrected vision improved significantly relative to their pre-hydrop state. Despite the patient’s significant corneal scarring, their BCVA also improved, and they were able to resume daily scleral lens wear.
This case highlights the importance of close monitoring and fully assessing each patient’s vision potential with scleral lenses or other specialty contact lenses following resolution of acute corneal hydrops. With adequate visual rehabilitation with a scleral lens, patients who heal from acute corneal hydrops may avoid a PKP and its associated risks.
References
- Barsam A, Petrushkin H, Brennan N, et al. Acute corneal hydrops in keratoconus: A national prospective study of incidence and management. Eye. 2015;29(4). doi:10.1038/eye.2014.333
- García de Oteyza G, Bregliano G, Sassot I, Quintana L, Rius C, García-Albisua AM. Primary surgical options for acute corneal hydrops: A review. Eur J Ophthalmol. Published online 2021:112067212110378. doi:10.1177/11206721211037833
- Grewal S, Laibson PR, Cohen EJ, et al. Acute hydrops in the corneal ectasias: Associated factors and outcomes. In: Transactions of the American Ophthalmological Society. Vol 97. ; 1999. doi:10.1016/s0002-9394(00)00447-5
- Kreps EO, Claerhout I, Koppen C. The Outcome of Scleral Lens Fitting for Keratoconus with Resolved Corneal Hydrops. Cornea. 2019;38(7):855-858. doi:10.1097/ICO.0000000000001946
- Meyer JJ, McGhee CNJ. Acute Corneal Hydrops Complicated by Microbial Keratitis: Case Series Reveals Poor Immediate and Long-Term Prognosis. Cornea. 2016;35(7). doi:10.1097/ICO.0000000000000883
- Meyer JJ, Gokul A, Crawford AZ, McGhee CNJ. Penetrating Keratoplasty for Keratoconus With and Without Resolved Corneal Hydrops: Long-term Results. Am J Ophthalmol. 2016;169. doi:10.1016/j.ajo.2016.07.001
