



WHAT YOU'LL LEARN
Understand the specific anterior segment pathologies
Learn about the role of scleral lenses in managing anterior segment pathologies
Introduction
Introduction
This course will review anterior segment pathologies and the role of anterior segment OCT in the fitting of scleral lenses to manage these conditions. Selected cases are included at the end of the course, as is a quiz.
The anterior segment includes structures in the front one-third of the eye, starting from the cornea to the crystalline lens. The cornea and ocular surface are especially complex, and, when functioning correctly, allow for clear and comfortable vision. However, significant visual impairment can result from abnormalities at the front of the eye, namely corneal ectasias and dry eye disease.
Anterior segment OCT can also be useful in managing glaucoma specifically when examining the angle, blebs, tubes and laser iridotomy assessments. Additionally it can help with managing ocular surface disorders such as dry eye disease, pterygia, pinguecula and scleromalacia. It can be helpful for surgical analysis for cornea, lens/cataract, biometry and LASIK. Anterior segment OCT provides a pivotal role in managing patients with corneal dystrophies and degenerations including keratoconus in addition to anterior segment tumors.
Keratoconus
Keratoconus
Keratoconus is a chronic, non-inflammatory ectasia of the cornea. It usually involves both eyes, but the severity per eye can be asymmetric. It is characterized by corneal steepening, visual distortion, corneal thinning, and central corneal scarring. Associated clinical findings that can be seen on slit lamp biomicroscopy are Fleischer ring, which are iron deposits around the cone’s base; Vogt’s striae, which are vertical stress marks in the areas of thinning; and apical scarring.
In Image 1, Fleischer ring is represented.

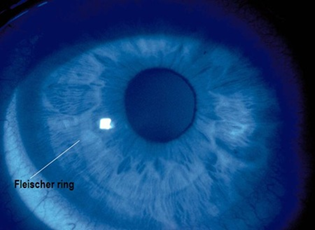
Image 1: Fleischer ring
In Image 2, we see an example of Vogt’s striae.

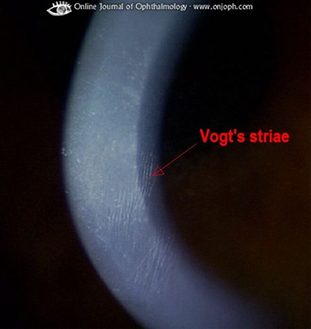
Image 2: Vogt's striae
In Image 3, Apical Scarring is shown.

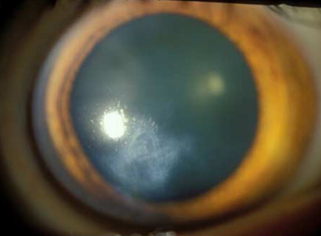
Image 3: apical scarring
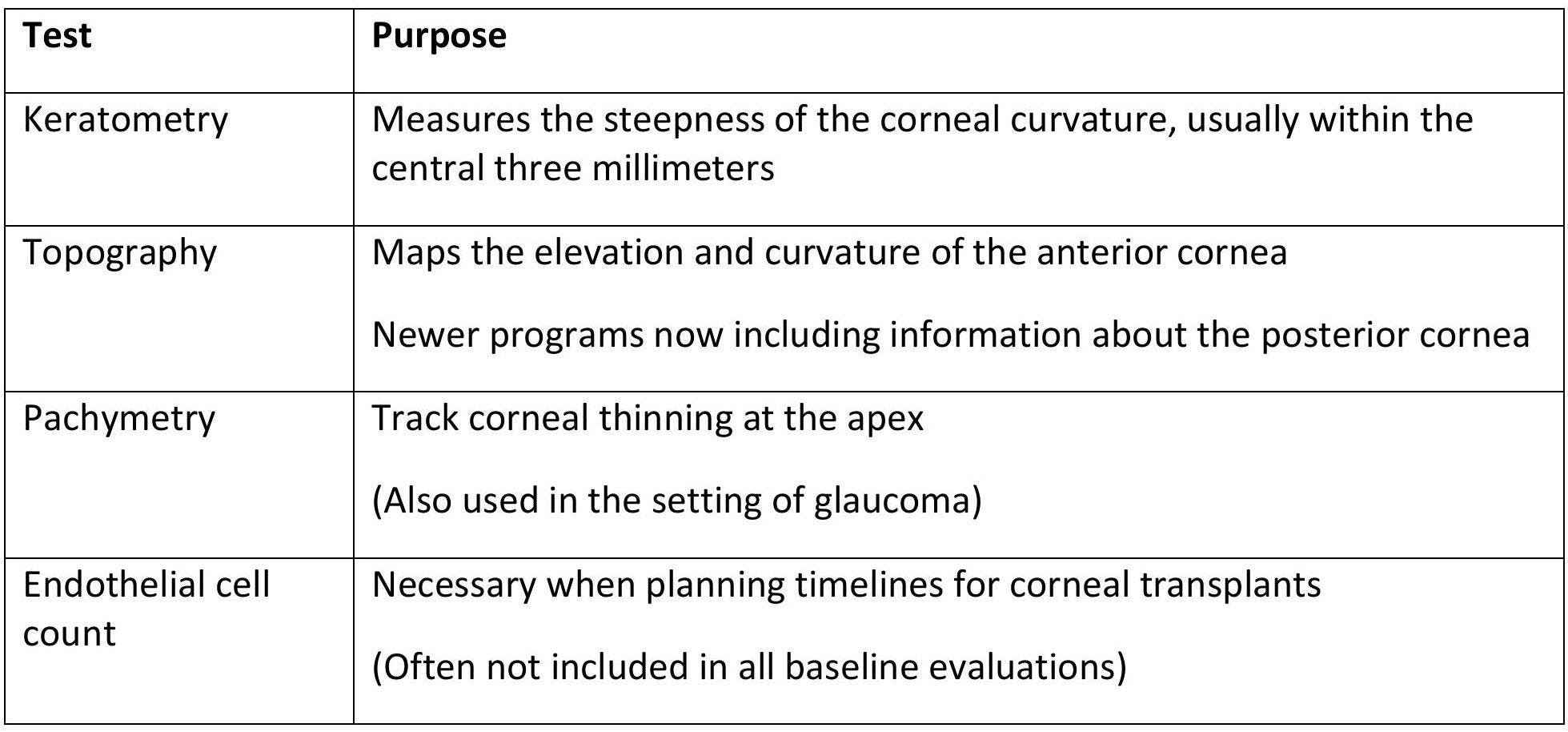
Keratoconus can be diagnosed and managed with the aid of numerous testing.

The goal of keratoconus management is to improve visual function. In its earlier stages, vision can be corrected by spectacles and standard or custom soft contact lenses. With more progression, corneal rigid gas permeable lenses, hybrid lenses, or scleral lenses are utilized. Avoiding eye rubbing is another objective, as constant mechanical manipulation of the elastic cornea can morph the corneal curvature.1 Fortunately, there are many options for anti-allergy eye drops for symptomatic relief of itching.
The current available treatments for keratoconus aim to reduce progression, but cannot reverse pre-existing damage. Corneal cross-linking is the newest FDA-approved procedure to slow or halt progressive keratoconus. It utilizes riboflavin and ultraviolet light to reinforce the collagen within the cornea. INTACS, or intrastromal corneal ring segments, are another option, involving PMMA semicircular rings in the stroma to flatten the cornea. As a last avenue, corneal transplants are warranted when all other treatments have failed to preserve vision.
Keratoconjunctivitis sicca
Keratoconjunctivitis sicca
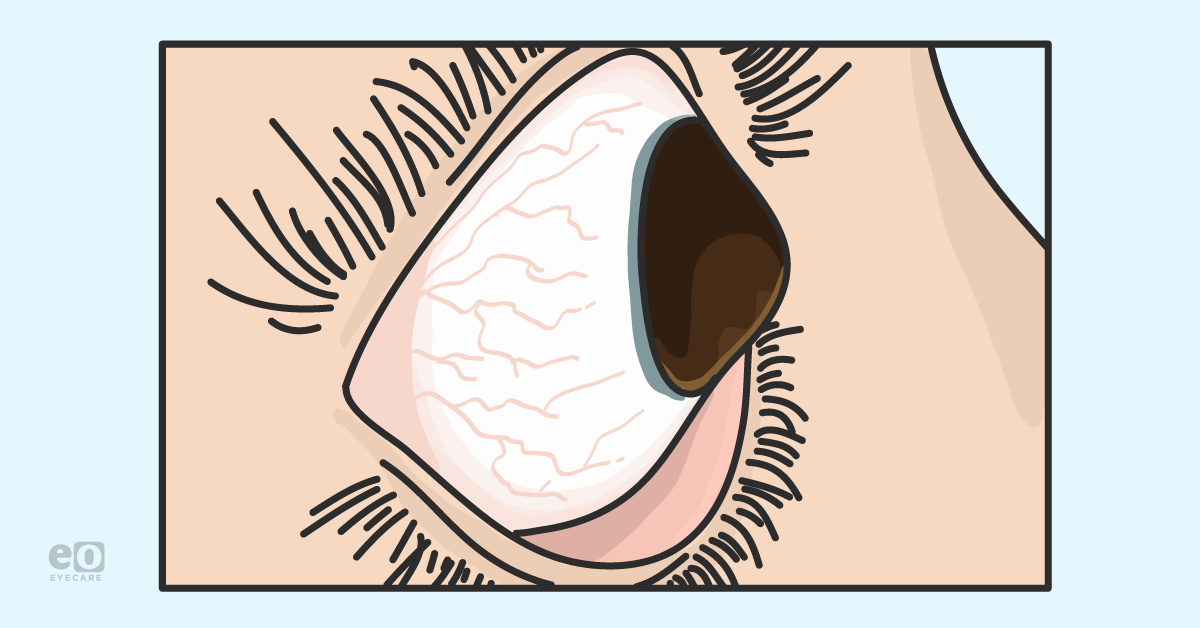
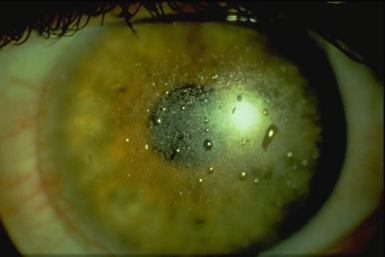
Dry eyes can sound like a mere nuisance, but keratoconjunctivitis sicca is the chronic dryness of the conjunctiva and cornea from an inadequate tear film. The etiology is often a combination of a tear production deficiency and inability to keep tears from evaporating from the eyes. This can change tear osmolarity and eventually lead to chronic ocular surface inflammation and corneal damage. Age, gender, medications, medical conditions, long-term contact lens use and history of LASIK can all contribute to dry eye disease. Symptoms can range from transient visual changes, discomfort, redness, photophobia, and pain. Various tests can assess dry eye disease, such as tear break up time, ocular staining, tear meniscus evaluation, Meibomian gland scans, and MMP-9 testing for tear film osmolarity.

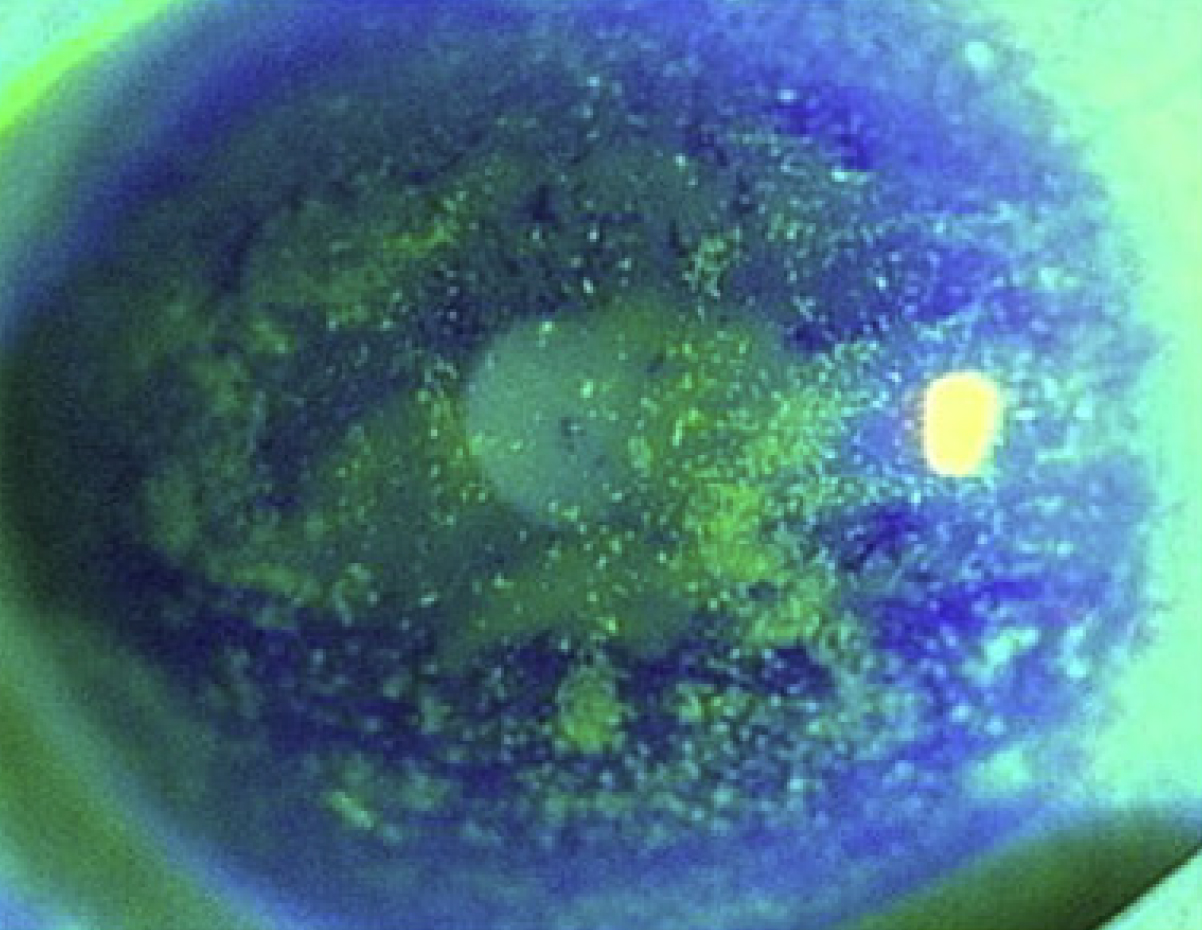
Image 4: Significant ocular surface disease due to severe dry eye
Dry eye disease can be a primary problem, isolated to the ocular surface itself. However, significant, recalcitrant dry eye disease can be secondary to another underlying disease. This can include patients who have Stevens-Johnson syndrome, Sjogren’s syndrome, Graft versus Host Disease, ocular cicatricial pemphigoid, and limbal stem cell deficiency. Mechanisms that hinder complete lid closure and normal blinking can cause chronic exposure keratopathy, like in Graves’ disease and facial palsies.
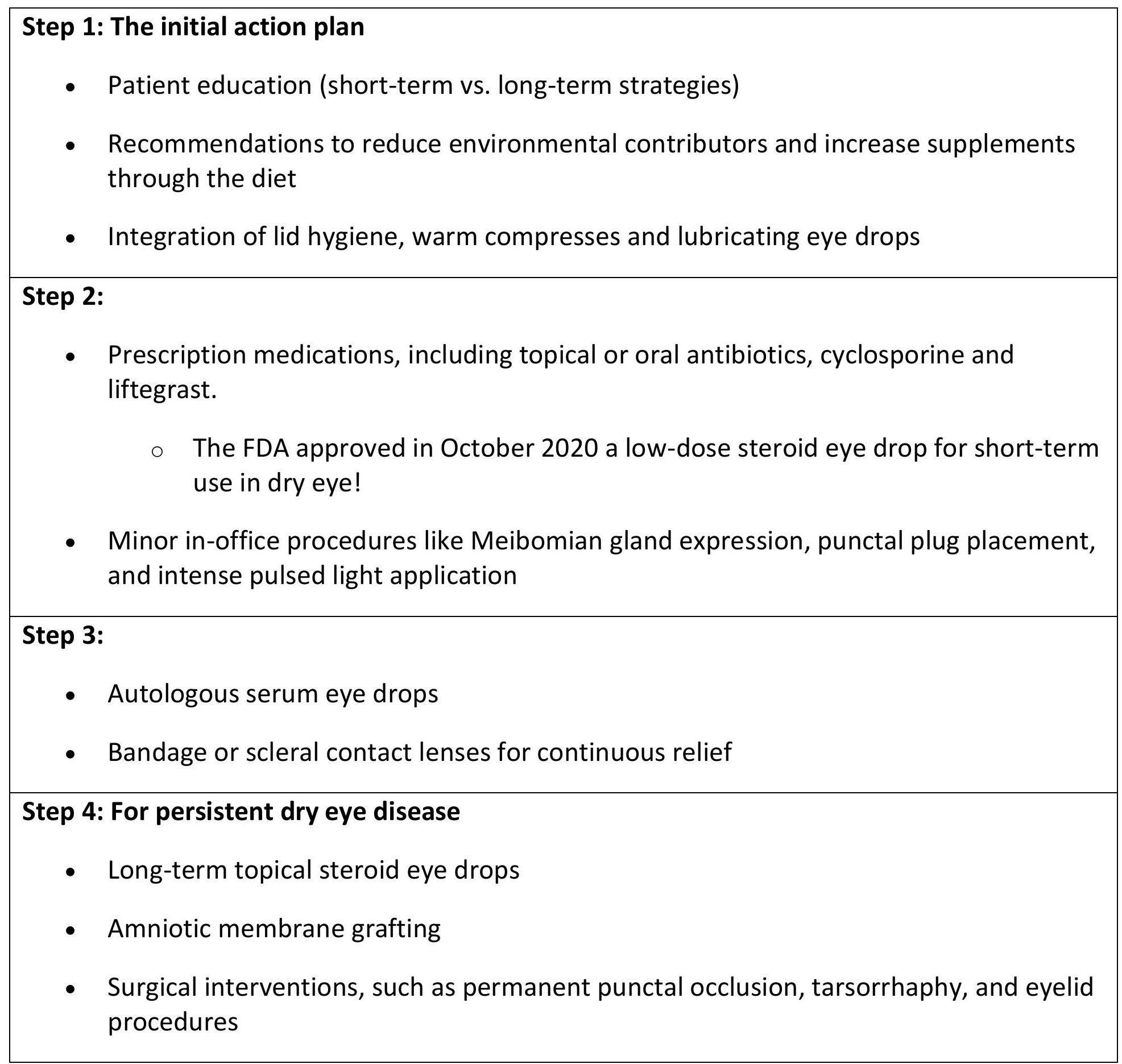
Specific treatment regimens can be challenging to implement, given that each patient can have a unique clinical profile regarding severity and progression. The Tear Film & Ocular Surface Society (TFOS) has developed guidance in 2016 for a stepwise approach for managing dry eye disease.2

The Role of Scleral Lenses
The role of scleral lenses
Scleral lenses are not new, but have become more integrated into clinical practice since the 1980s and 1990s. They are currently used to manage corneal irregularities, such as keratoconus and complications post corneal transplants, as well as to protect the ocular surface especially in patients with keratoconjunctivitis sicca. Though the term “scleral lens” is commonly associated with large diameter scleral lenses, scleral lenses fall under the general umbrella of rigid gas permeable lenses and have different names based on the diameter of the lens.
Each lens brand has proprietary naming, but all essentially have three main zones. The optic zone vaults over the cornea with a fluid reservoir, simultaneously providing corneal hydration and optical correction. The transition zone overlies the limbus, and the haptic or landing zone rests on the conjunctiva.
Image 5 shows Scleral contact lens basic fit.

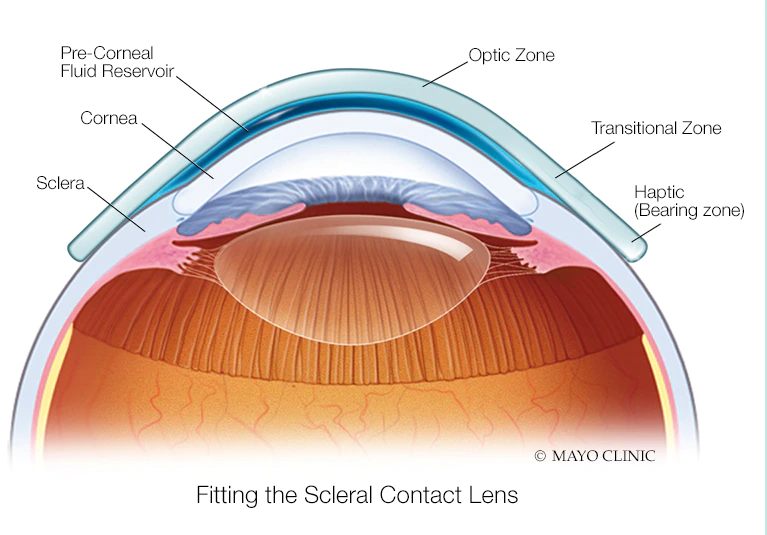
Image 5: scleral contact lens basic fit
When assessing the fit of a scleral lens, the slit lamp is the first place to check with both white light and blue cobalt light. Michigan College of Optometry at Ferris State University developed a valuable scleral lens fit scale to evaluate the fitting relationships between the lens and the eye.
Image 6 represents the Scleral lens fit scales from Ferris State University.

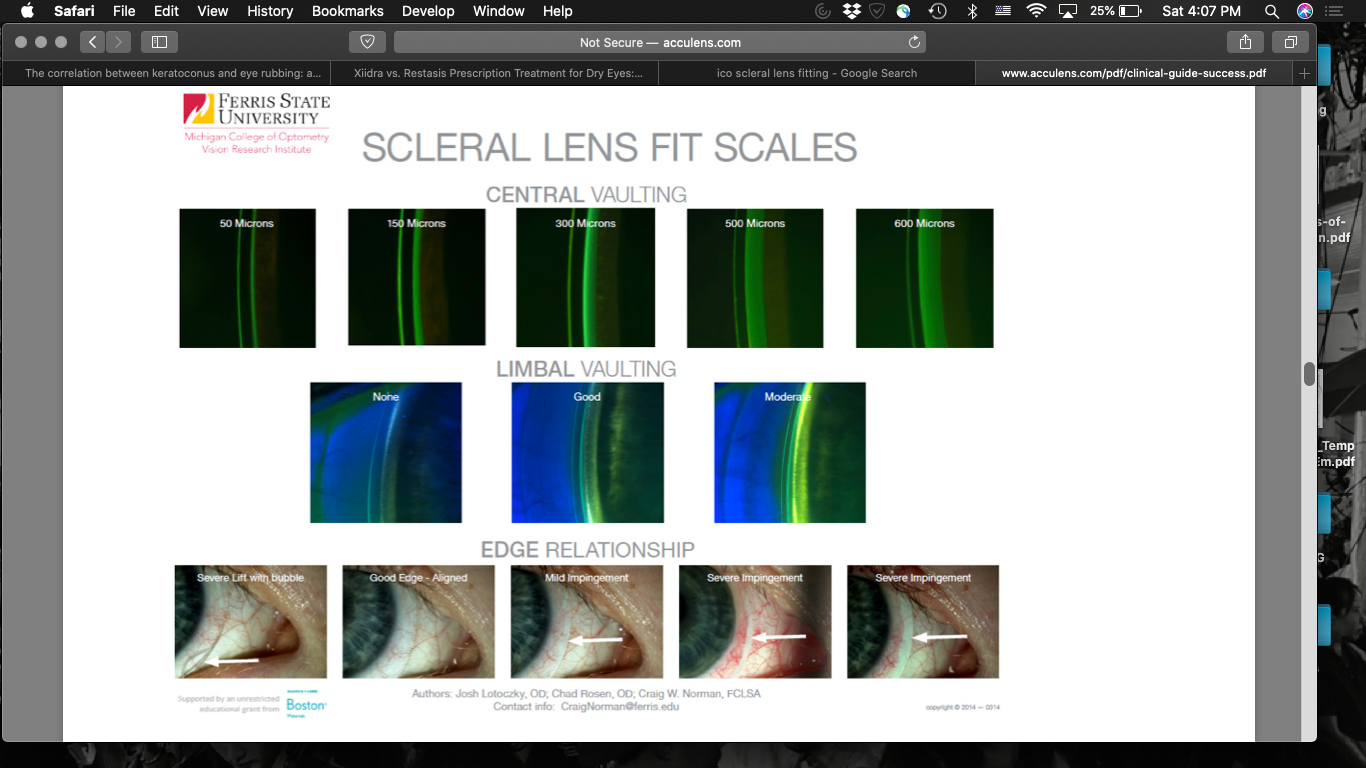
Image 6: scleral lens fit scales from Ferris State University
The anterior segment OCT has become an increasingly valuable tool to quantify the microns of clearance and document fitting relationships. In fact, most doctors who fit scleral lenses regularly would not do so today without the help of an anterior segment OCT. This allows for precision fitting in all aspects of the lens/ocular surface interaction which is especially useful for patients with corneal irregularities who make up a large percentage of patients being fit with scleral lenses.
Image 7 shows tear film after allowing the lens to settle.

A good-fitting scleral lens will have apt vaulting over the cornea with no areas of touch. A final central clearance after accounting for lens settling should be in the ballpark of 200 microns. Adequate limbal clearance of less than 50 microns is also important, so as to not contribute to corneal edema or hypoxia. A soft and wide scleral alignment without areas of impingement or blanching has clinical and comfort implications. This factor contributes to patient comfort, as a tight lens will be hard to remove and uncomfortable while a loose lens will cause lens awareness and lens fogging from debris entering into the fluid reservoir. Recent evidence demonstrates that the sclera has inherent toricity, so landing zones should be tailored accordingly. Fortunately, every zone of the scleral lenses can be modified independently, so creating the ideal lens is achievable. When fitting scleral lenses, aim to avoid corneal/limbal touch, bubbles, blanching/impingement and excess edge lift or movement.

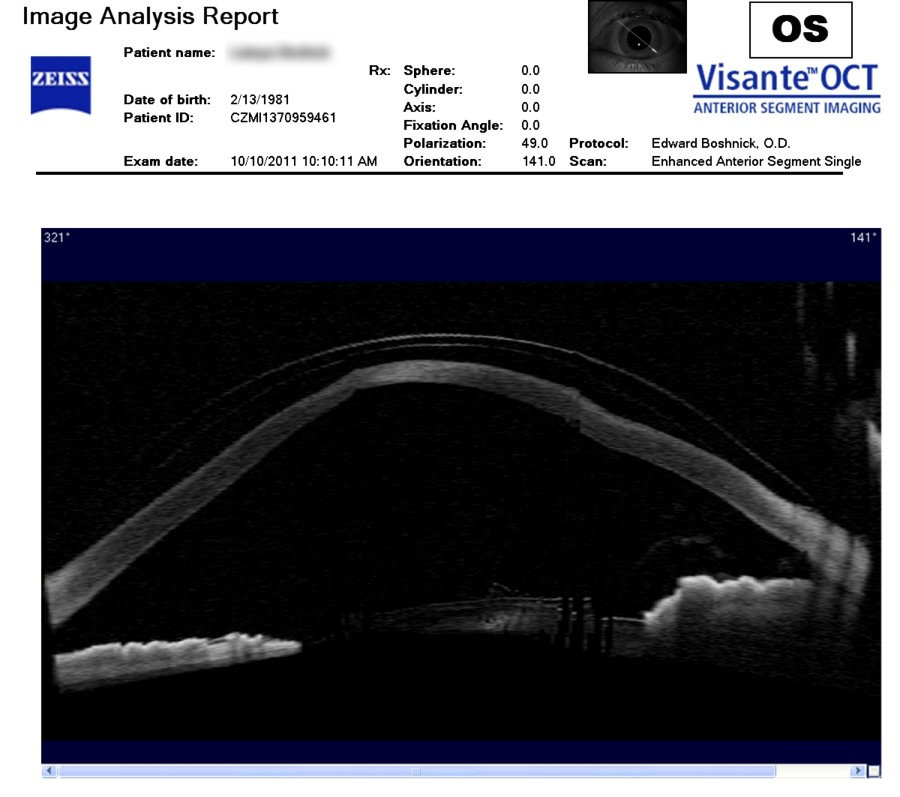
Image 8
Case 1: Keratoconus
Case One: Keratoconus
A 63-year-old male with a medical history of hypertension and chronic kidney disease was seen for evaluation of keratoconus which he has had for 40 years. He has previously been intolerant to RGp and hybrid contact lenses. He discontinued scleral lens wear due to lens fogging two years ago. Best corrected acuity with spectacles is 20/50 in the right eye and 20/25 in the left.


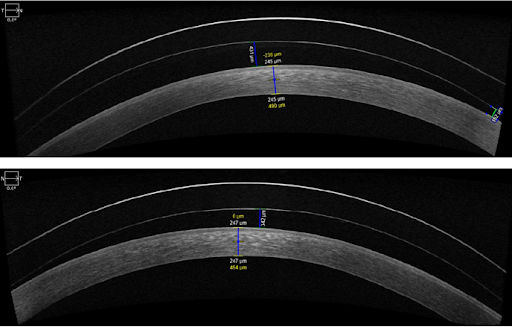
As Image 9 below shows, anterior segment OCT was used to determine the fit of the scleral lens at multiple positions of the corneal/lens and limbus/lens interface.

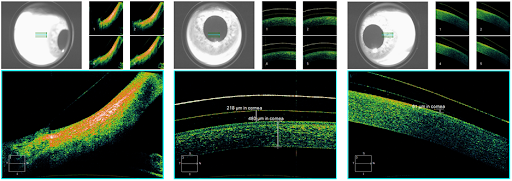
Image 9: Courtesy of Dr. Patel
Due to conjunctival toricity, the peripheral curves were changed to enhance patient comfort in a scleral lens. With a Visionary Optics Europa lens in the following parameters, the patient was able to see 20/20 and have lens comfort.
OD: BC 50.5, 16mm, PWR -1.75 D sph, 200 um toric haptic; VA 20/20
OS: BC 49.0, 16mm, PWR -3.50 D sph, 200 um toric haptic; VA 20/20
Case 2: Keratoglobus
Case 2: Keratoglobus
A 38-year-old male was referred for a corneal evaluation for keratoglobus in both eyes. Keratoglobus is a rare condition that is grouped with other non-inflammatory corneal ectasia and includes keratoconus and pellucid marginal corneal degeneration (PMCD). Keratoglobus is characterized by diffuse thinning of the cornea from limbus-to-limbus associated with protrusion of the cornea. The corneal diameter is normal which differentiates it from megalocornea and buphthalmos. Keratoglobus is a bilateral condition that is usually present at birth. It is usually minimally progressive. Keratoglobus has been associated with systemic connective tissue disorders such as Ehlers-Danlos syndrome, Marfan syndrome and Rubenstein-Taybi Syndrome.
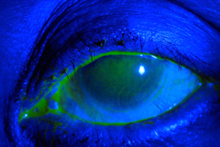
Figure 10 shows keratoglobus.


Figure 10
This patient has a medical history of cutis laxa and history of globe rupture in the left eye 10 years before presentation. His best corrected visual acuities with glasses on presentation was 20/50 in the right eye and 20/70 in the left eye. Slit lamp examination demonstrated diffuse peripheral thinning in both eyes and a temporal corneal opacity in the left eye.
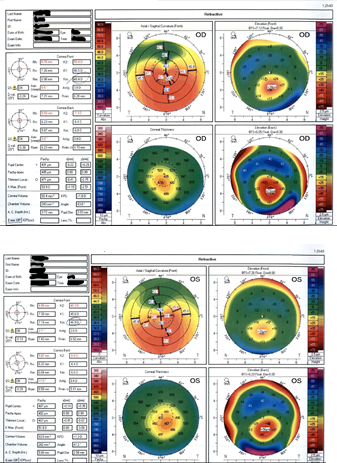
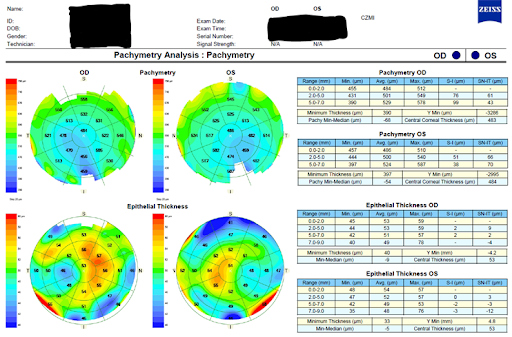
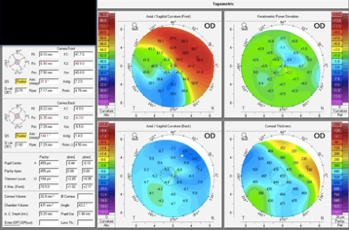
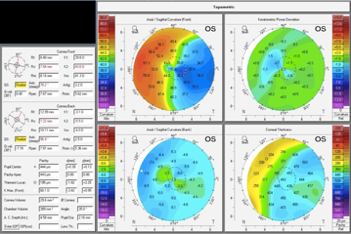
His topography scans are below. Notable findings are the remarkable pachymetry values of 184 microns in the right eye and 194 microns in the left eye.


With highly irregular and very steep corneas, the patient would benefit from a large diameter scleral lens with higher sagittal depth to protect the limbus from congestion. He was fit in a 18.5 mm diameter BostonSight scleral lens, and was able to achieve vision of 20/20 in both right and left eyes.
Image 11, below, shows the BostonSight Scleral lens fitting over the area of corneal thinning. This lens provided the patient with 20/20 vision.

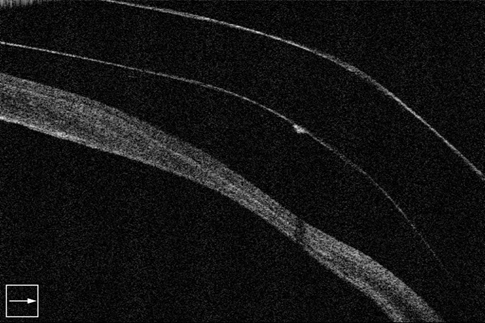
Image 11: Courtesy of Dr. Patel
For similar patients with highly irregular corneas or advanced stage disease, impression molding technology like the EyePrint Pro could be considered. Scleral topography can also provide additional information to create the best lens.
Image 12 demonstrates making a mold of a patient’s eye using EyePrint Pro.


Image 12
Case 3: Dry eye disease
Case 3: Dry Eye Disease
A 26-year-old female medical student with a history of Ankylosing Spondylitis treated systemically with Humira and Methotrexate presented with complaints of severe dry eye after LASIK 4 years prior. She was referred by outside OMD for scleral lens fitting. Best corrected spectacle VA was OD 20/20, OS 20/20. Ocular therapies at time of presentation were Restatis 4/4, Xiidra 2/2, Lotemax 2/2, PF Artificial Tears, Autologus Serum Tears prn, Lacriserts, Azasite, Ointment qhs, punctal plug on both upper and lower lids and Prokera treatments. The goal of a scleral lens fitting was to improve patient comfort and possibly limit topical medications.
Image 13 shows The patient was fit with BostonSight Scleral 18.5 mm OU 20/20, Optimum Infinite.
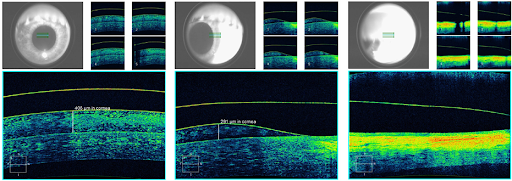
Image courtesy of Dr. Patel
Case 4: Stevens-Johnson Syndrome
Case 4: Stevens-Johnson syndrome
A 47-year-old female presented with chronic eye pain, itching, and decreased vision in both eyes. Her medical history was significant for Stevens-Johnson Syndrome which was presumed to be from a doxycycline reaction. She had severe ocular surface disease, symblepharon OU, and a history of punctate epithelial defects and trichiasis. She had scheduled surgery for her brunescent cataracts, but her surgeon elected to postpone the operation until her ocular surface was better managed. She was unsuccessful with multiple therapies to manage her ocular surface symptoms, and was wearing a bandage contact lens in both eyes. Her best corrected visual acuities with Kontur lenses on presentation was 20/200 in the right and left eyes. Her intractable ocular surface disease is demonstrated below and was a large contributor to her poor vision.

She was fit with a scleral lens which provided much improved vision. However, because of her Stevens-Johnson syndrome, there were apparent deficiencies with the lens wetting, as shown below. Adding a coating like Tangile Hydra-PEG is a great option for lens wettability and enhanced comfort.

After the coating was added, the patient had clear and comfortable vision with scleral lenses–a notable 20/20 vision in both eyes! This was a necessary step to improve her ocular surface for cataract surgery as well provide enhanced vision, protection, and comfort.
Conclusion
Conclusion
Corneal ectasias and keratoconjunctivitis sicca can be visually debilitating conditions, but patient outcomes continue to improve as diagnostic and imaging technologies develop. Testing is a critical adjunct to the clinical examination to fully understand the severity and progression of anterior segment diseases. The treatment plans for keratoconus and dry eye disease often follow a stepwise approach for improved vision and symptoms. These plans should include scleral lenses, as they are an excellent option to preserve vision before more challenging therapies, like surgery, are needed. The ability to customize parameters and create a uniform refracting surface positions scleral lenses as a promising treatment option for patients.
References
References
- McMonnies CW. Mechanisms of rubbing-related corneal trauma in keratoconus. Cornea. 2009;28(6):607-615.
- Craig JP et al. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017 Oct;15(4):802-812.
