


As of 2024, it is estimated that 9.7 million have undiagnosed diabetes, 29.3 million people have diagnosed diabetes, and 115.9 million have prediabetes.1 This makes up almost half the US population.
Because the incidence rate is increasing, screening is necessary to detect both diabetes and prediabetes in at-risk groups.2 Often, primary care optometrists prove key in the diagnosis through evidence and clinical findings gathered during routine eye exams.
Diabetes can lead to a wide range of ocular conditions, from diabetic retinopathy and diabetic papillopathy to glaucoma, cataracts, and even ocular surface diseases.
It is paramount that today’s ODs have a comprehensive understanding of the disease and its potentially sight-threatening ocular sequelae.3
Definition of diabetes mellitus
Diabetes mellitus (DM) is a disorder caused by an increase in blood glucose concentrations. Diabetes is classified into four general categories: type 1, type 2, diabetes due to other causes, and gestational diabetes.4
Type 1 DM is due to an autoimmune reaction that leads to the loss of insulin-producing beta cells in the pancreas, resulting in an absolute insulin deficiency and a lifelong dependency on exogenous insulin. Type 2 DM (~95% of all diabetes) is associated with insulin resistance, impaired secretion, and a relative insulin deficiency.5
Types 1 and 2 vary by clinical presentation, disease progression, and treatment. Both can be the result of various genetic and environmental factors that ultimately result in the progressive loss of β-cell mass and/or function and hyperglycemia.
Patients with both types of diabetes are at risk for developing the same systemic and ocular complications, though progression rates may differ.4
An overview of diabetic papillopathy
Diabetic papillitis, also called diabetic papillopathy (DP), is a relatively rare occurrence of systemic diabetes.6 It was first reported in 1971, and because it is considered a self-limited disease, the exact incidence rates are difficult to determine.
The prevalence is thought to be around 0.5% regardless of the patient’s glycemic control and the severity of the condition. It was initially found in younger patients but has since been found to affect diabetics of all age groups.7 Surprisingly, more patients with non-proliferative diabetic retinopathy (NPDR) present with DP compared to those with proliferative diabetic retinopathy (PDR).3
Diabetic papillopathy presents as a swelling of the optic nerve, usually unilateral, but can be bilateral, and is considered a diagnosis of exclusion. Both type 1 and type 2 diabetic patients may present with diabetic papillopathy.6
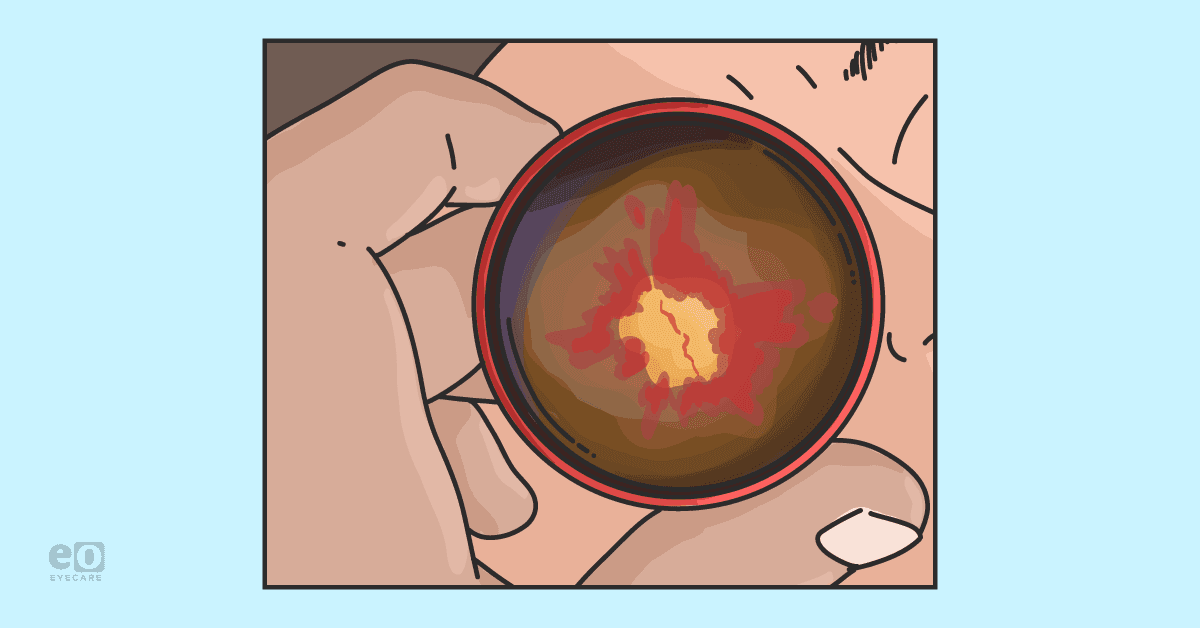
Figure 1 shows fundus photography of a patient with diabetic papillopathy that revealed a swollen optic disc, splinter hemorrhages, and dilated vessels over the optic disc.8


Figure 1: Reproduced with permission from Choi et al.
Pathophysiology of diabetic papillopathy
The exact pathophysiology of the condition is not fully understood, but researchers have proposed several ideas. Because there is no link between the condition and either diabetic retinopathy or metabolic control, DP may be a subtype of non-arteritic anterior ischemic optic neuropathy (NAION), but with some unique features.
The most likely mechanism is a limited impairment of the peripapillary vasculature and the superficial capillary network endothelial cells, leading to leakage in and around the optic nerve.3
Rapid changes in glycemic control are also associated, and it is thought this change may cause an accumulation of fluid between the retinal nerve fibers, ultimately causing compression at the retrolaminar part of the nerve. This leads to decreased axoplasmic flow at the lamina cribrosa and, finally, results in disc edema.9,10,11
Risk factors for DP
The biggest risk factor is a history of diabetes mellitus. Often, the condition may worsen in patients who underwent rapid changes in medications to correct their blood glucose levels.12
Study data regarding diabetic optic neuropathies, in general, reported that duration of diabetes, older age, systolic blood pressure, severity of diabetic retinopathy, central foveal thickness, and glycated hemoglobin are potential risk factors.13
Presentation of diabetes papillopathy
The condition generally occurs in patients with uncontrolled diabetes and presents with the following features:7
- Painless visual loss
- Macular edema
- Disk hyperfluorescence on fluorescein angiography
- Vision typically improves post-treatment
Patients with diabetic papillopathy present with few symptoms except mildly blurry vision. Presenting visual acuity may range from 20/20 to 20/200.13 Occasionally, it may be accompanied by intraretinal hemorrhages and hard exudates.14 In addition, the typical signs of optic neuropathy are usually not present, including an afferent pupillary defect (APD), dyschromatopsia, and visual field defects.13
The optic nerve appears swollen, hyperemic, and dilated optic nerve head vasculature is seen in 50% of cases; however, they remain on the disc surface and do not extend into the vitreous, differing from PDR. Macular edema is common in patients with diabetic papillopathy; it is present in more than 70% of patients.
Diabetic retinopathy may not be present in all patients but has been reported in 63 to 80% of cases. Just because a patient does not have diabetic retinopathy does not mean the ECP can rule out diabetic papillopathy as a cause for the optic nerve head swelling.13
Criteria for diabetic papillopathy diagnosis
Diabetic papillopathy is a diagnosis of exclusion, and all other causes should be ruled out first, including neovascularization of the disc (NVD) due to proliferative diabetic retinopathy.7 Optic disc edema has multiple etiologies and ECPs must differentiate between them to arrive at a final diagnosis by considering the patient’s history and the clinical examination.15
Infectious, inflammatory, and metastatic conditions, hypertension, papilledema, and pseudopapilloedema should all be differentials. Fluorescein angiography, orbital magnetic resonance imaging (MRI), and blood tests, including serum angiotensin-converting enzyme (ACE), antinuclear antibody (ANA), vitamin B12, folate, erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), and fluorescent treponemal antibody absorption (FTA-ABS) can be used to aid in diagnosis.7
A retrospective analysis of 47 patients (70 eyes) reported the most common causes for a swollen optic nerve(s). Hypertensive retinopathy and diabetic papillitis accounted for ⅓ of the bilateral cases of optic disc swelling. The data suggests that if the disc is swollen unilaterally, differential diagnoses should include optic neuritis, NAION, and neuroretinitis.
However, if the disc is swollen bilaterally, an ECP should consider increased intracranial pressure, hypertensive retinopathy, and diabetic papillitis. Optic neuritis and NAION can be bilateral also but are less common.15
Assessment and testing for DP
A neuro-ophthalmological assessment should be a part of the diagnostic work-up as further testing such as neuroimaging is required.6 Optic nerves are an extension of the central nervous system and imaging is vital to confirm the diagnosis.
MRI
An MRI plays an important role in the evaluation of the optic nerve and the entire visual pathway to rule out any life-threatening conditions. The imaging provides a detailed look into the anatomy of optic nerves using soft tissue contrast and without exposing the patient to ionizing radiation.
An MRI provides the ECP with a better view of the entire visual pathway to identify any potential intracranial pathologies.16
Visual fields
Visual fields may show blind spot enlargement in patients with diffuse disc edema, but most patients with diabetic papillopathy will not have a significant visual field defect.
An optic nerve head optical coherence tomography (ONH OCT) will show an increase in the thickness of the papillary profile without loss of the retinal nerve fiber layer (RNFL). The OCT of the macula is usually normal, but edema from the nerve may track towards the macula.13
Fluorescein angiography
Fluorescein angiography (FA) is the most useful test to distinguish diabetic papillopathy from other differential diagnoses like NVD.
Diabetic papillopathy may present with disc telangiectasias and disc edema, which look similar to NVD. However, diabetic papillopathy will show disc and peripapillary leakage with radial distribution of fluorescein in dilated vessels, whereas, with NVD, there will be a random pattern of the vasculature with intravitreal leakage.13
Figure 2 demonstrates fluorescein angiography of a patient with diabetic papillopathy showing hyperfluorescence caused by fluorescein leaks from the new vessels.8


Figure 2: Reproduced with permission from Choi et al.
Differential diagnosis: DP vs. NAION
Diabetic papillopathy differs from NAION because of the inflammatory component. If prominent telangiectasia is not present, the delayed filling pattern of the disc in diabetic papillopathy can mimic NAION.
The level of vision loss and condition of the nerve can be used to make a diagnosis. Patients with an NAION typically present with a sudden loss of vision, swelling at the optic disc, varying degrees of APD, dyschromatopsia, and altitudinal visual field defects.6
Studies have suggested that DP patients have a shorter disease duration and are relatively younger compared to patients with NAION.17 NAION is more common in the elderly because they often have other systemic conditions such as hypertension, DM, dyslipidemia, and cardiovascular illnesses that lead to microvasculopathy at the optic disc.15
OCT imaging does not provide a clear diagnostic distinction between DP and NAION patients. After the disc swelling has resolved, an OCT can show secondary atrophy of both the peripapillary RNFL and the macular ganglion cell layer, regardless of the patient’s visual acuity.
No thinning of the macular inner nuclear layer (mINL) was observed in either condition. The data suggests there were no distinguishing structural imaging biomarkers for NAION and diabetic papillopathy either acutely or later in the disease course.6
Lastly, patients should be asked if diabetic medications have recently been added and/or changed. Several clinical cases show the development of diabetic papillopathy after new hyperglycemic therapy was added to the patient’s regimen.12,18
Table 1 lists differential diagnoses to consider when treating a patient suspected of having diabetic papillopathy.
| Condition | Uni/Bilateral? | Testing? | VF Defects? | APD? | VA Loss? |
|---|---|---|---|---|---|
| Diabetic Papillopathy | Unilateral | FA: Diagnosis of exclusion | Varies | No | Mild |
| Optic Neuritis | Unilateral | MRI/FA | Yes | Usually | Significant |
| NAION | Unilateral | FA | Yes | Yes | Significant |
| NVD | Either | FA, HbA1c | Varies | No | Varies |
| Neuroretinitis | Unilateral | FA, Blood Tests | Yes | Yes | Significant |
| Hypertensive Retinopathy | Bilateral | Dilated Fundus Examination, Blood Pressure Reading | Varies | Yes | Varies |
| Papilledema | Either | MRI, LP | Yes | Yes | Varies |
Table 1: Courtesy of Courtney Dryer, OD.
Medical management of diabetic papillopathy
At present, no treatment can change the disease progression, but most edema resolves without vision loss, within a few months. Observation is indicated for mild visual acuity and mild disc swelling after life-threatening conditions have been excluded.13
Intravitreal anti-VEGF injections
However, the presence of severe disc edema and macular edema may require treatment. A few studies have shown a benefit to intravitreal injections.19 The main indication of using anti-vascular endothelial growth factor (VEGF) therapy like bevacizumab is to treat the macular edema.20
Anti-VEGF injections did improve visual acuity; however, the long-term effects are unknown.21,22 The exact mechanism of action of a drug like bevacizumab on DP is not well understood.20
Steroid injections
Other studies suggest there may be a benefit to periocular steroid injections in symptomatic cases of diabetic papillopathy. A study by Mansour et al. found that steroid treatment shortened the duration of diabetic papillopathy from a median of 5 months to 3 weeks, with rapid visual recovery.23
It is thought that periocular steroids work by stabilizing the blood-ocular barrier at the disc, leading to the resolution of the edema.7 Intravitreal triamcinolone acetonide use does have potentially adverse effects, including elevated intraocular pressure (IOP), cataract progression, pseudo-endophthalmitis, and infectious endophthalmitis.19
Combination therapy
A case study from 2021 demonstrated the benefit of using a combination of the two aforementioned therapies. Intravitreal aflibercept and subtenon triamcinolone acetonide together led to a rapid and safe improvement in visual acuity.19
When comparing both treatments, steroids vs. anti-VEGF, Choi et al. reported that both routes had similar effects on diabetic macular edema (DME), but that steroid injection increased IOP after 3 months.24 Both injections led to a significant constriction of retinal arteries and veins and a decline in vascular permeability and leakage.19
Patients with any type of diabetic retinopathy, including diabetic papillopathy, require multispecialty management. Communication amongst specialties leads to better patient care and disease management.25
In some cases, referral to neuro-ophthalmology and/or retina may be indicated to confirm the diagnosis and to decide the best course of treatment.
Prognosis for diabetic papillopathy
Visual prognosis is good for patients with diabetic papillopathy. Most often, the condition will resolve on its own without intervention.
Though the data is somewhat limited, steroid injections and/or anti-VEGF treatment may resolve both the disc edema, and/or macular edema more quickly.
In conclusion
Diabetic papillopathy is a rare but significant manifestation of diabetic eye disease that requires prompt evaluation and management.
This condition is characterized by optic disc edema, mild visual acuity loss, and can be a challenge to diagnose because it resembles other optic nerve disorders.
Further research is needed into the underlying pathophysiology to enhance our understanding, management, and the development of improved treatment protocols.
