



Ocular trauma is a major cause of vision loss and blindness worldwide.
In the United States, an estimated 2 to 2.4 million cases of ocular trauma occur annually, with many leading to permanent vision loss.1 Ocular trauma has a 14% lifetime prevalence in the general population.2
Overview of traumatic cataracts
Trauma disproportionately affects children and young men.2 Traumatic cataracts form after direct or blunt ocular injury disrupts lenticular fibers, leading to their opacification. Cataracts may form immediately after trauma or may form months or even years later.
“Rapid cataract formation is more commonly seen with direct anterior capsule violation.”
Traumatic cataracts are believed to form due to direct rupture of the capsule or coup contrecoup injury with equatorial expansion from hydraulic forces transferring traumatic energy to the opposite side of the eye. The mechanism of injury greatly impacts the visual prognosis.
Patients presenting with other ocular co-morbidities, such as corneal or scleral lacerations, retinal detachment, and angle recession, will have a more guarded visual prognosis compared to a non-penetrating ocular trauma.
Diagnosing traumatic cataracts
A careful history and slit lamp examination are required in order to fully assess a patient with a traumatic cataract. History should focus on details of the mechanism of injury, including any possibility of direct penetrating injury or risk of foreign body exposure. The timeline of visual impact is also important. Of course, this will be more straightforward in a patient presenting immediately after a major trauma.
However, for patients presenting months or years later, knowing this timeline and the patient’s pattern of vision loss during that time can be helpful. For example, if a patient did not note any vision loss until years later, the patient may have a better visual prognosis as that suggests that more of their acute vision loss may be from the cataract alone and not other ocular co-morbidities.
Important considerations for diagnosing a traumatic cataract:
- Age: The patient’s age should also be taken into consideration, as children will be at risk of amblyopia if a visually significant cataract is not addressed promptly.
- Ocular history: The patient’s past ocular history, including past surgical history, should be reviewed as it may have implications for surgical management.
- Medical history: Past medical history and patient allergies should also be reviewed as they may have implications on intraoperative medications and post-operative healing. For example, diabetes is associated with a higher risk of infection. Poorly controlled diabetes and hypertension are also risk factors for intraoperative complications such as suprachoroidal hemorrhage.
Depending on the clinical presentation and mechanism of injury, a computed tomography (CT) scan of the orbits may be needed urgently to further characterize the posterior globe and look for the presence of intraocular foreign bodies. While an open globe cannot be completely ruled out with imaging alone, it can be a helpful tool when the view into the globe is limited due to lens opacification heme or other vitreous opacities. In addition, it can help identify orbital fractures, which may need to be addressed following globe closure (if pertinent) or prior to cataract surgery.
Examination protocol for a traumatic cataract
Examination should start with checking the patient’s visual acuity and carefully checking the patient’s pupils for the presence of an afferent pupillary defect. A relative afferent pupillary defect can result from traumatic optic neuropathy or optic nerve avulsion and ultimately suggest a more guarded visual prognosis. A cataract alone will not result in an afferent pupillary defect.
In the setting of acute trauma, it is then helpful to check the patient’s globe to ensure there is no direct penetrating injury before proceeding. For example, manipulation of the globe to obtain an intraocular pressure (IOP) can place additional force on the globe and lead to further prolapse of intraocular contents.
“Once globe stability is confirmed, an intraocular pressure may be obtained.”
A low pressure suggests either a penetrating injury with potential globe rupture or a cyclodialysis cleft. Of note, a normal intraocular pressure cannot rule out an open globe, as a self-sealing wound may be present. Sometimes, globe exploration with conjunctival cut down and scleral exploration may be needed to rule out an occult perforation.
An elevated IOP may be evidence of lens-associated glaucoma (phacomorphic, phacoantigenic, lens-particle glaucoma), hyphema, orbital compartment syndrome (for example, from a retrobulbar hematoma in the acute setting), or angle recession glaucoma (in a patient presenting after a more remote injury).
Clinical pearls for a successful slit lamp examination of a traumatic cataract
A slit lamp examination should then be performed to look for the presence of any penetrating injury. A fluorescein strip can be used to perform a Seidel test to identify the presence of full-thickness corneal lacerations. In an intact globe presenting after a remote injury, gonioscopy should be performed to look for the presence of angle recession.
The depth of the anterior chamber may be a helpful parameter. An asymmetric deep anterior chamber (relative to the other unaffected eye) can suggest angle recession or zonulopathy, leading to the patient’s lens being more posterior compared to an unaffected eye.
It is helpful to check the patient’s iris for the presence of transillumination defects before dilation. Intraocular foreign bodies may pierce through the iris and, therefore, the lens capsule as well. Iris synechiae, which may need to be lysed at the time of cataract surgery, may be present between the iris and the lens capsule. The presence of any vitreous should also be noted as it will become relevant in the upcoming surgery.
Then, a slit lamp examination focused on the lens should be performed. The examination should look for any focal opacities, violation of the anterior lens capsule, grade of the nucleus, and lens stability. Careful examination for potential phacodonesis, which suggests underlying traumatic zonulopathy, may be done by having the patient look in various directions at the slit lamp. Classically, a traumatic cataract presents with a rosette or stellate appearance.
Further valuable exams when assessing a traumatic cataract
A dilated exam is also important to rule out any posterior traumatic involvement and damage, which may limit the patient’s ultimate visual outcome. If a dense cataract limits the view, a B scan can be performed to rule out any major retinal detachment or vitreous opacity.
While B scans are helpful in this regard, they cannot completely rule out all retinal damage as photoreceptor damage from commotio retinae may still be present and ultimately limit the patient’s best corrected visual outcome. Additionally, ultrasound biomicroscopy can be a helpful adjuvant to better characterize the posterior capsule and lens position.
Surgical management of traumatic cataracts
Surgical management of a traumatic cataract depends greatly on the clinical presentation. The cataract should be removed urgently if there is lens capsule violation, phacomorphic glaucoma, or other risk factors for severe intraocular inflammation or elevated intraocular pressure, including severe lens dislocation. Lens implantation can be performed in a secondary surgery if there is poor visualization. Otherwise, it is reasonable to stabilize the globe and then perform cataract removal with intraocular lens (IOL) implantation in a more controlled manner at a future date.
Performing primary cataract removal with lens implantation has the advantage of a single hospital stay, decreased risk of elevated IOP in phacomorphic or phacoantigenic cases, and decreased visual rehabilitation time. For pediatric cases, there is also less risk of subsequent amblyopia with primary cataract removal with lens implantation. In the setting of an open globe, when there is an increased risk of endophthalmitis, cataract removal and IOL implantation may be considered at a later date, once the eye has had time to heal and visual prognosis can be more accurately assessed.
“Planning for a secondary procedure to remove the cataract leads to the ability to obtain more accurate IOL calculations and typically improved visualization during surgery.”
For cases where primary cataract lens removal with IOL implantation is being performed, IOL calculations from the unaffected eye or with the use of average K values of 44D can be helpful. When selecting an intraocular lens, a three-piece lens should be considered as it can provide more stability in the capsular bag and also more options for sulcus placement or even subsequent scleral fixation in the future if needed. Sutureless scleral fixation with a scleral glued technique or a Yamane technique can also be safely utilized for secondary lens placement in the setting of significant capsule and zonular loss.
Figure 1 shows scleral fixation using the Yamane technique, which can be performed when there is complete capsular instability and zonular loss. In this photo, the leading haptic is being introduced into a thin lumen 30G TSK needle.

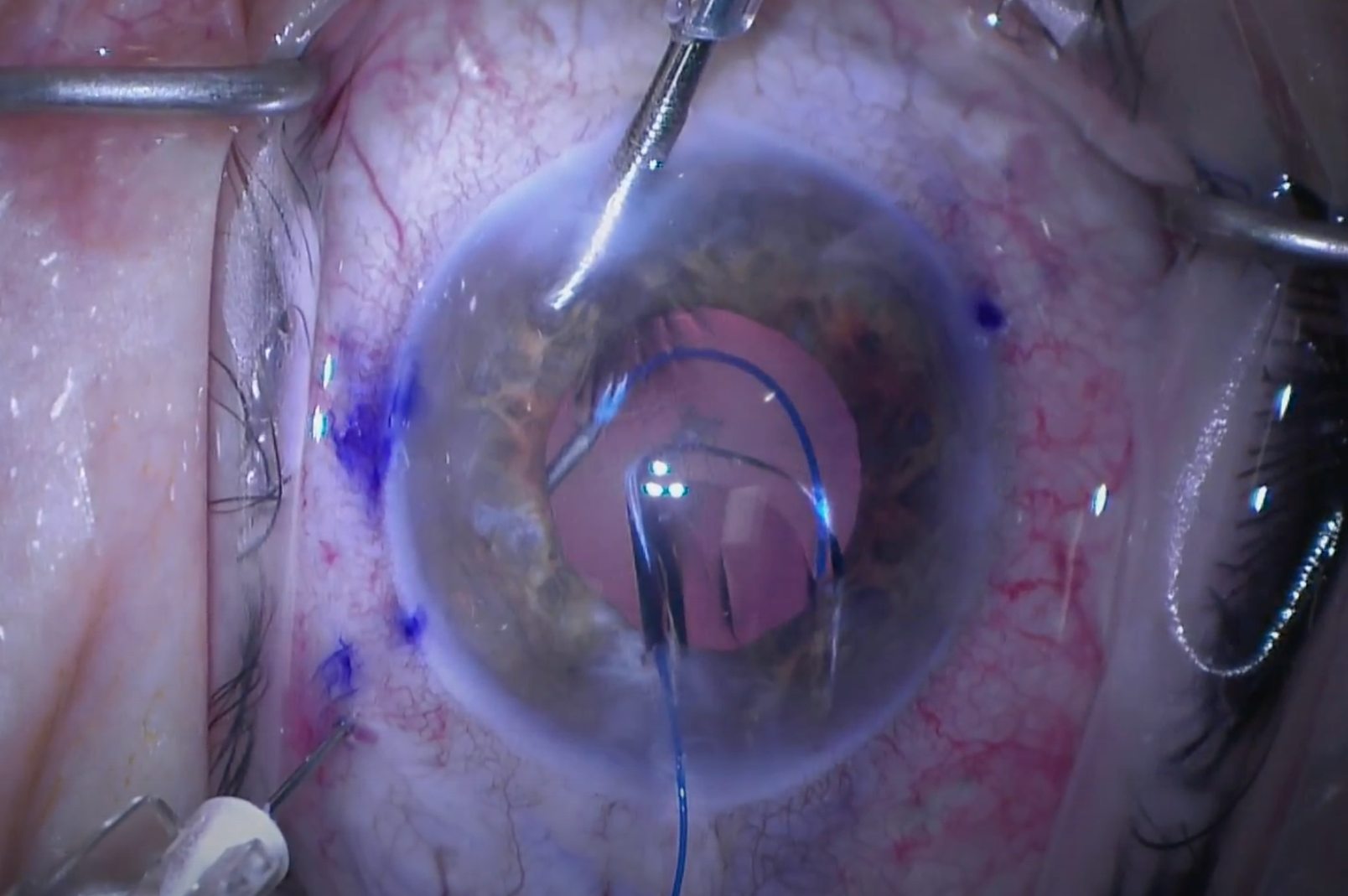
Figure 1: Courtesy of Mina Farahani, MD.
Potential surgical complications
There is higher risk of intraoperative complications depending on the mechanism of injury. Capsular violation, zonulopathy, vitreous prolapse, and hyphema can all be encountered depending on the injury and chronicity of the cataract. There may be some anterior and posterior synechiae that need to be gently released to ensure adequate visualization for surgery.
Once releasing these, there still may be poor pupillary dilation; therefore, iris hooks or a Malyugin ring can be considered to achieve adequate visualization. If there has been significant iris loss or trauma, pupilloplasty can be considered in the primary surgery or at a later date.
Figure 2 highlights pupilloplasty, which can be considered in the case of iris trauma.

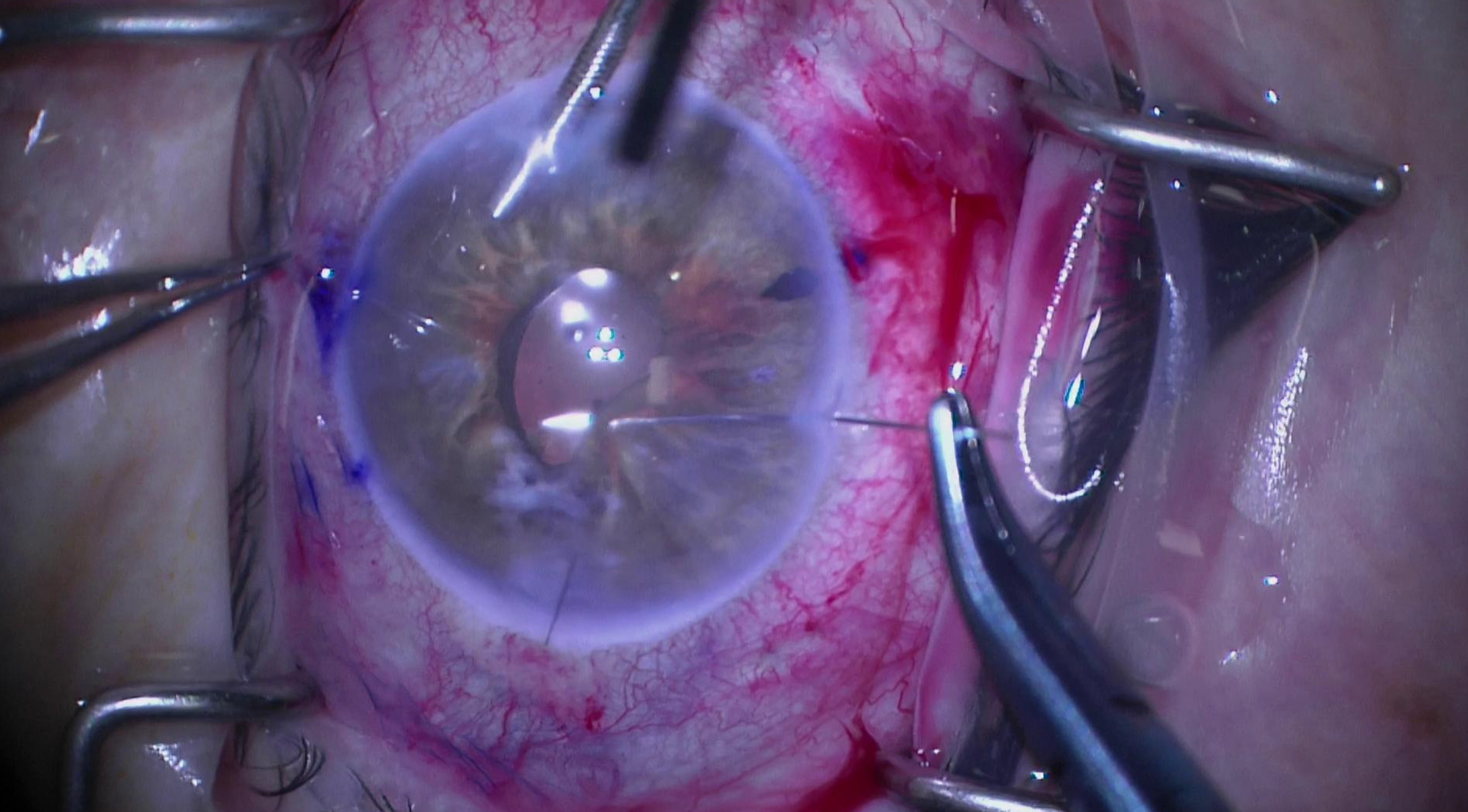
Figure 2: Courtesy of Mina Farahani, MD.
Dense anterior stellate and white cataracts can make anterior capsule visualization difficult. Trypan blue can be used to aid in performing a continuous curvilinear anterior capsulorrhexis.
Figure 3 shows Trypan blue, which can be used to visualize the anterior chamber in the setting of a white cataract.

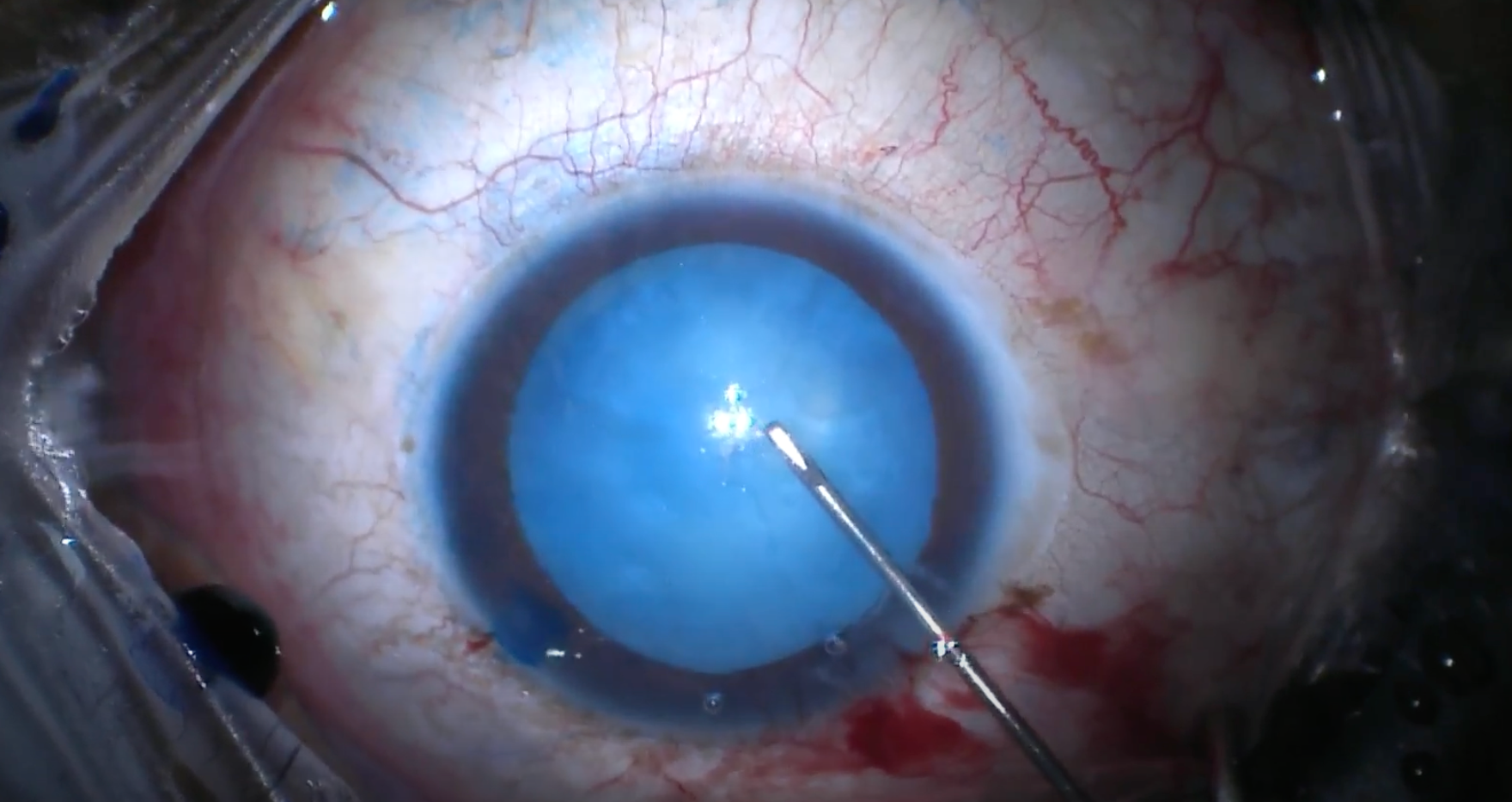
Figure 3: Courtesy of Mina Farahani, MD.
Surgical pearls for managing complications from traumatic cataracts
Surgeons should go into these cases expecting some level of zonulopathy. When instilling viscoelastic into the anterior chamber, movement of the lens more posteriorly may suggest significant zonulopathy. When making the rhexis, striae or wrinkling of the anterior capsule, with lack of tension of the anterior capsule flap, also suggest zonulopathy. Hydrodissection and phacoemulsification should be performed with minimal downward pressure, as it can induce further stress on the zonules.
During phacoemulsification, lowering the bottle height, low aspirate rate, and low vacuum settings should all be considered in order to minimize additional stress on the zonules. Anterior vitrectomy may be required for any vitreous prolapse related to zonulopathy or capsule violation.
“Capsule retractors can be placed to keep the capsular bag anterior as surgery is being performed.”
For cases with 3 clock hours or less of zonular dehiscence, a capsular tension ring can be placed in the capsular bag. For cases with more than 3 clock hours of zonulopathy, capsular segments (i.e., Ahmed segments) or a Cionni ring can be sutured to the sclera using prolene or Gore-Tex suture.
For chronic traumatic cataracts with expected zonulopathy, there may be an additional benefit to using femtosecond laser-assisted cataract surgery (FLACS). FLACS can provide a perfectly centered and sized anterior capsulorrhexis while providing some lens fragmentation that can facilitate easier lens removal and manipulation.
Post-operative care for traumatic cataract
Post-operatively, care is often similar to routine cataract surgery, with attention to intraocular pressure and anterior chamber inflammation. Post-operative visits for day 1, week 1, and month 1 are typically done, with additional appointments as needed to address any complications.
As soon as there is an adequate view, a dilated examination should be performed to look for the presence of any posterior pathology that may not have been easily visualized in the setting of a dense cataract. Often these cases will have more post-operative inflammation; therefore, a longer course of topical steroids may need to be considered.
