


Since its FDA approval in 2010, femtosecond laser-assisted cataract surgery (FLACS) has become an important technology for surgeons to enhance manual phacoemulsification techniques. FLACS also offers refractive advantages for patients undergoing cataract surgery.
I have found FLACS to be an incredible asset for my cataract surgeries. It has proven its benefits time and again in providing a safe, efficient method of performing cataract surgery across a variety of patients.
Basic Principles
Femtosecond laser-assisted cataract surgery is an innovative, growing technology for cataract surgery due to enhanced precision and minimized tissue damage from the femtosecond laser ablation.1-6 This attribute of femtosecond lasers is especially important for femtosecond laser cataract surgery, wherein the protection and preservation of ocular structures such as the capsular bag and corneal endothelium are critical for visual outcomes.1-8
Multiple commercial femtosecond lasers have been cleared for use by the US FDA for cataract surgery, including use in creating corneal incisions, capsulotomy, and lens fragmentation.1-6,9-12 These lasers include LenSx (Alcon Laboratories, Inc.), Catalys (Abbott Medical Optics), LensAR (LensAR Inc., Orlando FL), Victus (Technolas Perfect Vision and Bausch & Lomb, Rochester, NY), and Femto LDV (Zeimer Ophthalmic Systems AG). These are solid-state femtosecond lasers integrated with an optical coherence tomography (OCT) imaging subsystem.1-6,9-12
Steps in FLACS
Following pupillary dilation and application of topical anesthesia, applanation of the cornea with a docking system (which usually involves a contact lens with a circumferential suction device to distribute pressure evenly) is performed.4-6 The docking system mildly increases intraocular pressure while minimally distorting anatomy.4-6
Once docking is complete, anterior segment imaging (OCT) is performed to identify important anatomical landmarks for laser pattern mapping.4-6,12 Specific boundaries are mapped, including the iris and lens posterior capsule (this is especially important to avoid accidental cutting of the pupillary margin, as well as puncture of the posterior capsule).4-6,12 Pre-programmed corneal incisions for temporal wound, paracentesis, and any corneal relaxing incisions can be adjusted to surgeon preference at this point as well.4-6,12 The pattern is then centered, approved by the surgeon, and laser executed.
An example of the OCT-based image planning is shown below.

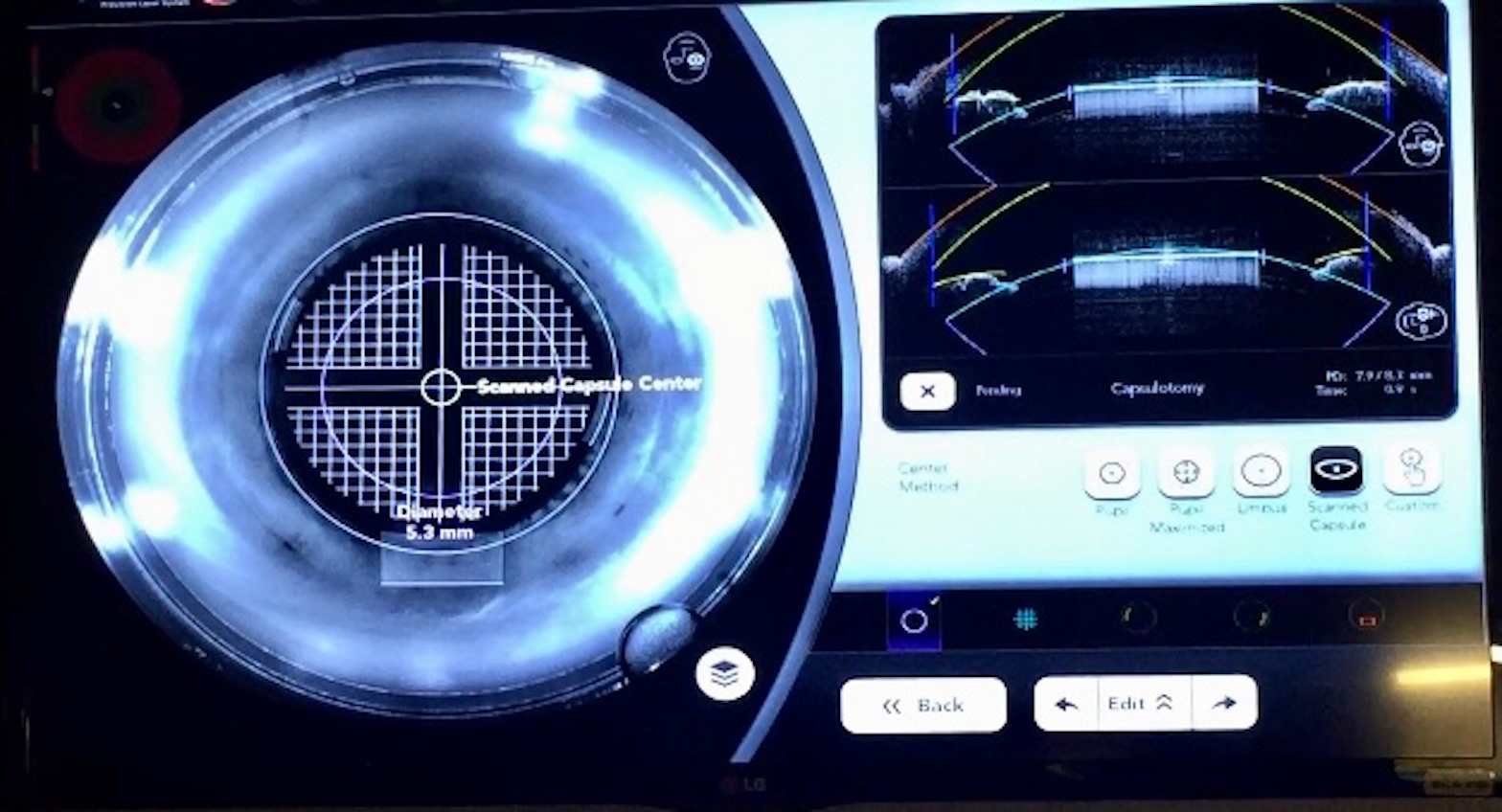
Once the laser portion is complete, the patient is moved into the operating room for cataract removal and IOL insertion.
Capsulotomy
Multiple studies have shown that manual creation of the capsulorhexis, known to be one of the most technically difficult parts of cataract surgery for those in training, can lead to tears in 0.8% of cases.1,4-6 Additionally, the unpredictable diameter observed in the creation of a manual capsulorhexis may have effects on IOL centration, unpredictable anterior chamber depths, suboptimal refractive outcomes, and increased rates of posterior capsular opacification.1,4-6 In fact, a shift of 1mm in IOL position, which may result from an inappropriately sized capsulotomy, can lead to a 1.25D change in refractive error.1,4-6,13
On the other hand, FLACS-created capsulotomy offers greater precision and predictability. The capsulotomy affects the ultimate lens position and how the capsular bag shrinks around the implanted IOL, which is size and centration-dependent.1,4-6 The accuracy and repeatability of a FLACS-created capsulotomy is another benefit—a manual capsulotomy may be smaller and even misshapen when created by hand versus by laser.
When performing cataract surgery using premium IOL technology (e.g., toric, presbyopia-correcting, and/or extended-depth of focus IOLs), FLACS can deliver a well-centered, standardized capsulotomy at surgeon size-preference to allow for guidance on IOL centration as well.1,4-6,13
Lens Fragmentation
FLACS can be extremely beneficial in very dense cataracts: the laser is able to pre-soften as well as divide the lens into quadrants, sextants, or octants.1,3-7,9 This ‘pre-phacoemulsification’ treatment can have a significant impact on the amount of ultrasound energy used during surgery, and save any undue excessive ultrasound trauma to the corneal endothelium.1,3-7,14
Less ultrasound energy use during cataract surgery can also translate to less potential surgical trauma to the surrounding tissues as well as a potentially faster recovery.1,3-7,14
Peripheral corneal relaxing incisions (Limbal Relaxing Incisions)/Astigmatic keratotomies:
Treatment of astigmatism with FLACS can allow for more precise visual outcomes; untreated residual corneal astigmatism may require spectacle correction or other refractive surgery post-cataract surgery in some patients if warranted.1,4-6,11,15-17 There are several corneal relaxing incision/astigmatic keratotomy nomograms a surgeon may choose from for treatment.1,4-6,11,15-17 LRICalculator.com, as well as LRICalc.com, are some widely used online resources a surgeon may use preoperatively to calculate the degree and length of corneal relaxing incisions.
The laser is able to produce precise location and depth for the femto-laser-generated relaxing incisions, therefore providing accurate and reproducible astigmatism correction for patients undergoing cataract surgery.1,4-6,11,15-18
The ability to treat corneal astigmatism with FLACS is limited, however; higher degrees of astigmatism (~1.50D and above) may be better treated by placement of a toric IOL (or use of spectacles by the patient postoperatively, should they choose). In addition, some argue that the astigmatic keratotomies created during FLACS (and even those by hand) may induce higher levels of dry eye and a degree of neurotrophic keratopathy (either temporary or permanent post-operatively) due to the severing of corneal nerves in the process.1,4-6,11,15-18 While this has yet to be proven, it may be an important factor to consider in those patients at risk for refractory dry eye or neurotrophic disease.
Toric Marking
If a surgeon is planning on performing cataract surgery using a toric IOL, the laser may also assist in making precise marks on the cornea to help ensure correct toric alignment at the time of surgery.1,4-6 Some FLACS systems have iris registration and precise 3D imaging to allow for precise axis markings for toric IOL implantation.1,4-6
Corneal incisions (paracentesis and main corneal incision)
FLACS also has the option of pre-placing the surgical paracentesis and main corneal incisions; the size and length of the incision can be tailored to the individual surgeon.5,6,9,10,19 These incisions can be opened at the time of surgery using a blunt instrument, rather than a blade.5,6,9,10,19 In addition, studies have been performed that demonstrate increased wound integrity and less potential for wound leak with femtosecond laser-created incisions versus those made manually, partially due to the ability to manipulate and create wound architecture in a way that is not feasible by hand.5,6,9,10,19
Overall benefits of FLACS
By performing key steps of cataract surgery: incisions, capsulotomy creation, lens fragmentation, as well as astigmatic correction, FLACS makes cataract surgery easier for the surgeon.1,3-5 There is less stress regarding perfect capsulotomy centration, and laser arcuate incisions/astigmatic keratotomies are reported to be more accurate, precise, and reproducible than most can perform by hand. Lens fragmentation can also make phacoemulsification more efficient.
FLACS may also make more challenging cases easier in some regards. Dense intumescent cataracts can have a fast, centralized capsulotomy created with little risk of radialization of an anterior capsular tear.1,3-6 Traumatic cataracts may be pretreated, potentially allowing for less manipulation during surgery, especially important in an already compromised situation.1,3-6
Risks or downsides of FLACS
While FLACS can be used in most eyes, not all system capabilities can be used in each case. Proper patient selection for FLACS can help improve outcomes. Patients with dense corneal opacities/scars that may affect laser energy transmission across the cornea to the lens may not be good candidates; these opacities may result in incomplete capsulotomy.1,6 In patients with keratoconus, astigmatic keratotomies are not advised; surgeons may want to avoid full-nuclear fragmentation in eyes with pre-existing posterior capsular defects or posterior polar cataracts, as this can put increased stress on an already weakened posterior capsule.1,6 Patients with small pupils, such as those with extensive posterior synechiae may not be candidates for laser-assisted capsulotomy creation (most surgeons prefer a capsulotomy around 5.0mm), but can still benefit from astigmatism correction.
The use of FLACS has been shown to cause prostaglandin release, which can induce pupillary miosis. Some surgeons may need to administer additional dilating eye drops prior to starting phacoemulsification for this reason.1,6 A large study evaluating data from the European Society of Cataract and Refractive Surgeons multicenter European Register of Quality Outcomes for Cataract and Refractive Surgery showed similar results for best-corrected vision between eyes that underwent manual cataract surgery vs. FLACS.2,8
Some surgeons argue that FLACS adds surgical time. Often the laser is first performed in a laser suite, and the patient is then escorted to the operating room for removal of cataract and insertion of IOL. Patient mobility and staffing may affect patient flow in these cases and perhaps add time (albeit a small amount) to the OR day.
FLACS systems are expensive, and in the US, are most commonly used in private practice surgical centers, rather than large academic medical centers or county hospitals. In addition, patients do incur an added cost with FLACS, as this technology is not currently covered by insurance.
Conclusions
There are continuous technological advancements in all aspects of cataract and refractive surgery. The addition of FLACS to the cataract surgeons’ armamentarium permits a streamlined ability to perform corneal wound and capsulotomy creation, as well as treat mild degrees of astigmatism, with the use of possibly less ultrasound energy. While this technology is still expanding in availability, it will be exciting to see future directions it takes in being able to provide safer, quicker, and incredibly precise outcomes for our cataract patients.
References
- Berk TA, et al. Visual and Refractive Outcomes in Manual versus Femtosecond Laser-Assisted Cataract Surgery: A Single-Center Retrospective Cohort Analysis of 1838 Eyes. Ophthalmology. 2018; 125(8): 1172-1180
- Manning S, Barry P, Henry Y, Rosen P, Stenevi P, Young D, Lundstrom M. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: Study from the European Registry of Quality Outcomes for Cataract and Refractive Surgery. J Cataract Refract Surg. 2016; 42(12): 1779-1790
- Schweitzer C. Evidence from the French FEMCAT Study. Presented at European Society of Cataract and Refractive Surgeons meeting; Oct 7-11 2017; Lisbon, Portugal
- Roberts H, Day A, O’Brart DPS. Femtosecond laser-assisted cataract surgery: A review. European Journal of Ophthalmology. 2019; 30(3): 417-429
- Roberts TV, Lawless M, Chan CC, et al. Femtosecond laser cataract surgery: technology and clinical practice. Clin Exp Ophthalmol. 2012; 41: 180-186
- Moshirfar M, Churgin D, Hsu M. Femtosecond Laser-Assisted Cataract Surgery: A Current Review. Middle East Afr J Ophthalmol. 2011;18(4): 285-291
- Chang D. Does femtosecond laser-assisted cataract surgery improve corneal endothelial safety? The debate and conundrum. J Cataract Refract Surg. 2017; 43(4): 440-442
- Lundström M, Manning S, Barry P, Stenevi U, Henry Y, Rosen P. The European registry of quality outcomes for cataract and refractive surgery (EUREQUO): a database study of trends in volumes, surgical techniques and outcomes of refractive surgery. Eye and Vision. 2015;2(8)
- Masket S, Sarayba M, Ignacio T, et al. Femtosecond laser-assisted cataract incisions: architectural stability and reproducibility. J Cataract Refract Surg. 2010; 36(6): 1048-1049
- Donnenfeld ED, Rosenberg E, Boozan H, Davis Z, Nattis A. Randomized prospective evaluation of the wound integrity of primary clear corneal incisions made with a femtosecond laser versus a manual keratome. J Cataract Refract Surg. 2018; 44(3): 329-335
- Lim C, Somani S, Chiu H, Maini R, Tam E. Astigmatic Outcomes of Single, Non-Paired Intrastromal Limbal Relaxing Incisions During Femtosecond Laser-Assisted Cataract Surgery Based on a Custom Nomogram. Clin Ophthalmol. 2020;14:1059-1070
- Sun, Hui. “Femtosecond-Laser-Assisted Cataract Surgery (FLACS).” High Resolution Imaging in Microscopy and Ophthalmology., edited by Josef Bille, Springer, 2019, pp. 301–316.
- Hollock EJ, Spalton DJ, Meacock WR. The effect of capsulorhexis size on posterior capsular opacification: One-year results prospective trial. Am J Ophthalmol. 1999;128:271-279
- Conrad-Hengerer I, Schultz T, Jones JJ, Hengerer FH, Dick B. Cortex removal after laser cataract surgery and standard phacoemulsification: a critical analysis of 800 consecutive cases. J Refract Surg. 2014; 30(8): 516-520
- Baharozian CJ, Song C, Hatch KM, Talamo JH. A novel nomogram for treatment of astigmatism with femtosecond-laser arcuate incisions at the time of cataract surgery. Clin Ophthalmol. 2017; 11:1841-1848
- Roberts HW, Wagh VK, Sullivan DL, Archer TJ, O’Brart DPS. Refractive outcomes after limbal relaxing incisions or femtosecond laser arcuate keratotomy to manage corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2018;44(8):955-963
- Nichamin L. Nomogram for limbal relaxing incisions. J Cataract Refract Surg. 2006; 32(9):1408
- Donnenfeld E, Rosenberg E. Assisting femto incisions with nomograms: Treat corneal astigmatism during cataract surgery. Ophthalmology Management. 2015: 48-52
- Uy H, Shah S, Packer M. Comparison of Wound Sealability Between Femtosecond Laser-Constructed and Manual Clear Corneal Incisions in Patients Undergoing Cataract Surgery: A Pilot Study. J Refract Surg. 2017; 33(11): 744-748
