


Sometimes, too much hardware in the eye can pose issues during cataract surgery.
This patient is a 78-year-old female who presented with visually significant cataracts in both eyes. Her right eye saw counting fingers, and her left eye was 20/40+. She had a 4+ nuclear sclerotic cataract in the right eye and a 3+ nuclear sclerotic and 2+ cortical cataract in the left eye. Her pupils dilated to only 4mm in both eyes. The posterior pole view was hazy but appeared normal.
Cataract extraction with insertion of a monofocal intraocular lens was planned first for the right eye, given the worse vision, and then the left eye. Due to significant pupillary miosis, Malyugin Ring insertion was planned for both eyes. The featured surgical video of this case displays the intra-operative technique for cataract extraction used in the patient’s right eye.

Watch the surgical video!
This surgical video demonstrates how to extract a dense cataract using the Malyugin ring and MiLOOP.

Dense cataract surgery: miLOOP versus Malyugin ring
After manually stretching the pupil with two Kuglen hooks, a 7.0 mm Malyugin Ring was placed to expand the poorly dilating pupil. Trypan blue was used to stain the anterior capsule due to a poor red reflex, and a large capsulorhexis was created.
Given the density of the cataract, a miLOOP was used to segment the nucleus. The miLOOP, manufactured by ZEISS, is an endocapsular nitinol ring that is injected through a clear corneal incision and encircles the nucleus. As the loop is withdrawn, it bisects the lens nucleus and makes a full-thickness cut. The lens can then be rotated and the miLOOP can be re-deployed.
The miLOOP shines in dense lenses where it can help break the lens nuclei, particularly dense nuclei with thick posterior plates, such as in this case, into 2 or 4 segments, that can then be more easily removed with phacoemulsification. When used correctly, the miLOOP can impose low zonular stress and reduce the time and energy needed to remove these types of cataractous lenses.
Too much hardware: just chop!
As I deployed the miLOOP, I felt that the lens nucleus was rotating more than usual, which concerned me for zonulopathy. In cases of zonulopathy, I do not like to proceed with using the miLOOP as this can cause further zonular disinsertion or capsular bag rupture. I chose to remove the miLOOP and move with chopping techniques.
Image 1 depicts deploying the miLOOP.

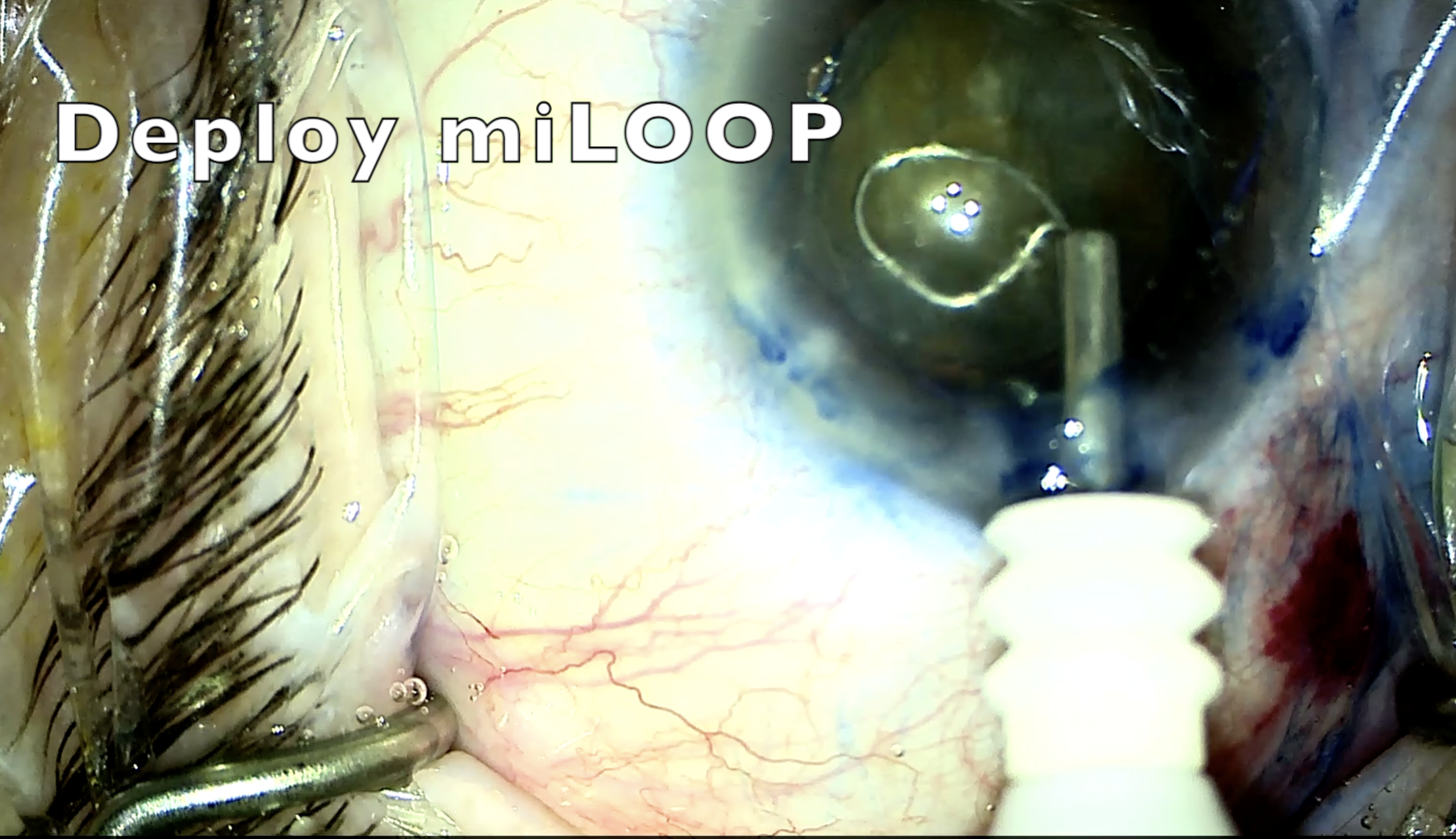
Image 1
Image 2 illustrates how the miLOOP causes the lens nucleus to tilt.

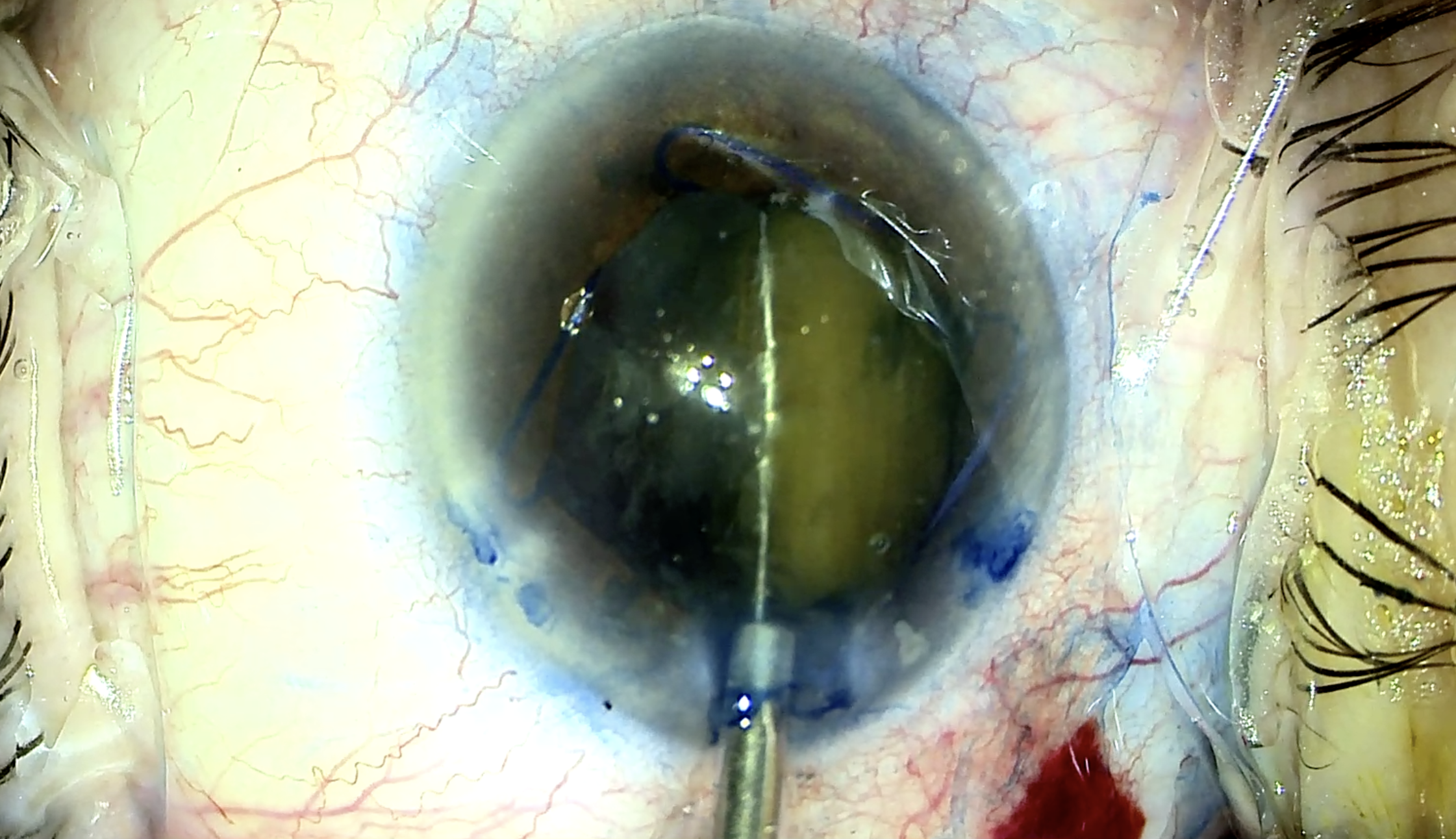
Image 2
However, as I attempted to retract the miLOOP rapidly, the nitinol snare got caught in the inferior loop of the previously inserted Malyugin Ring!
Image 3 demonstrates the stuck miLOOP.

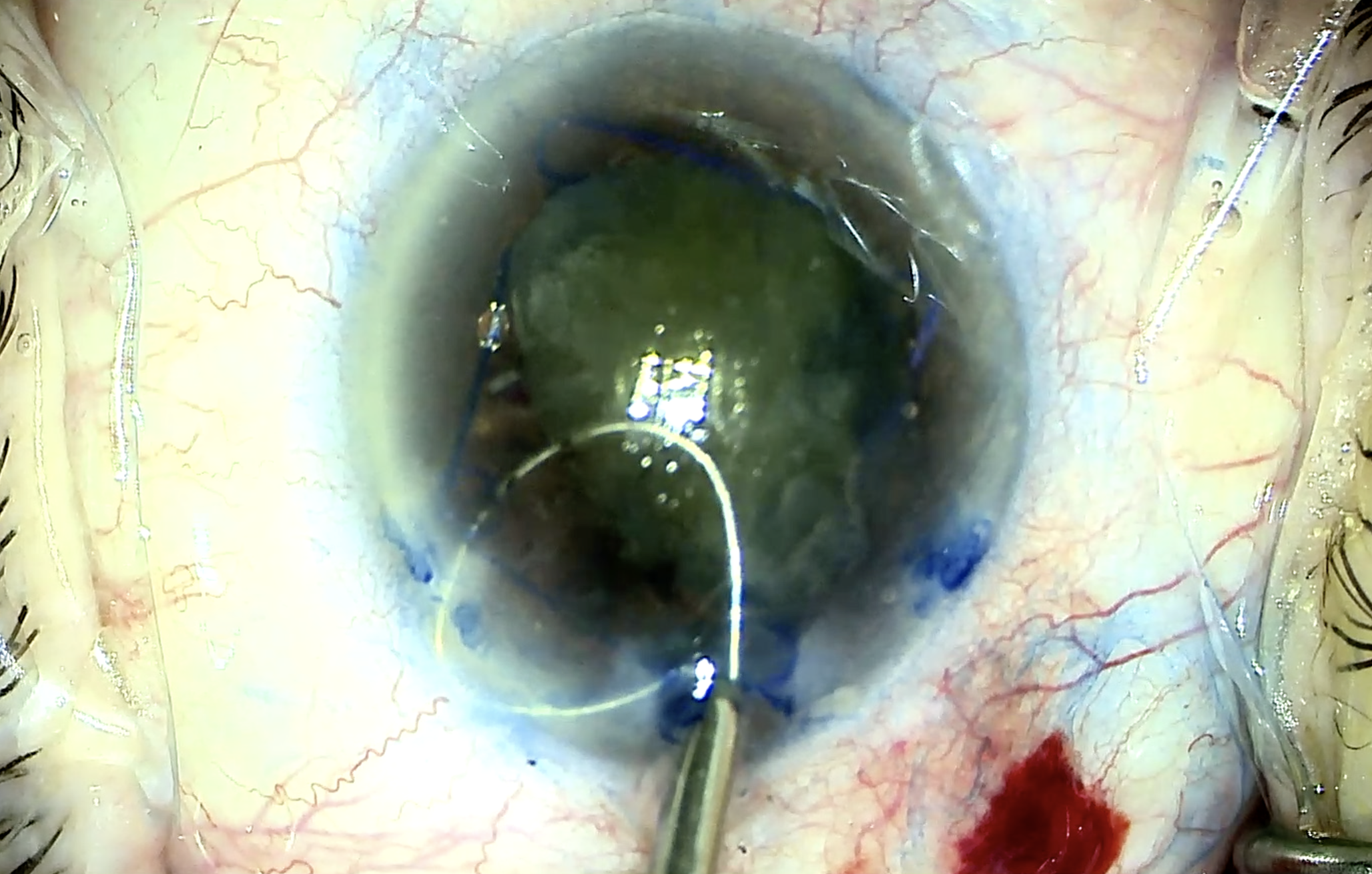
Image 3
This was the first time I had encountered such a scenario. At this point in the case, I paused and had to evaluate how to remove the Malyugin Ring. I gently retracted the miLOOP and simultaneously moved the inferior ring of the Malyugin Ring off to the side with a Sinsky hook and was able to slide the loop off the ring edge.
Interested in other complex cataract case reports? Check out the reports on White Cataracts and the Morgagnian Cataract!
Image 4 demonstrates gently retracting the miLOOP.

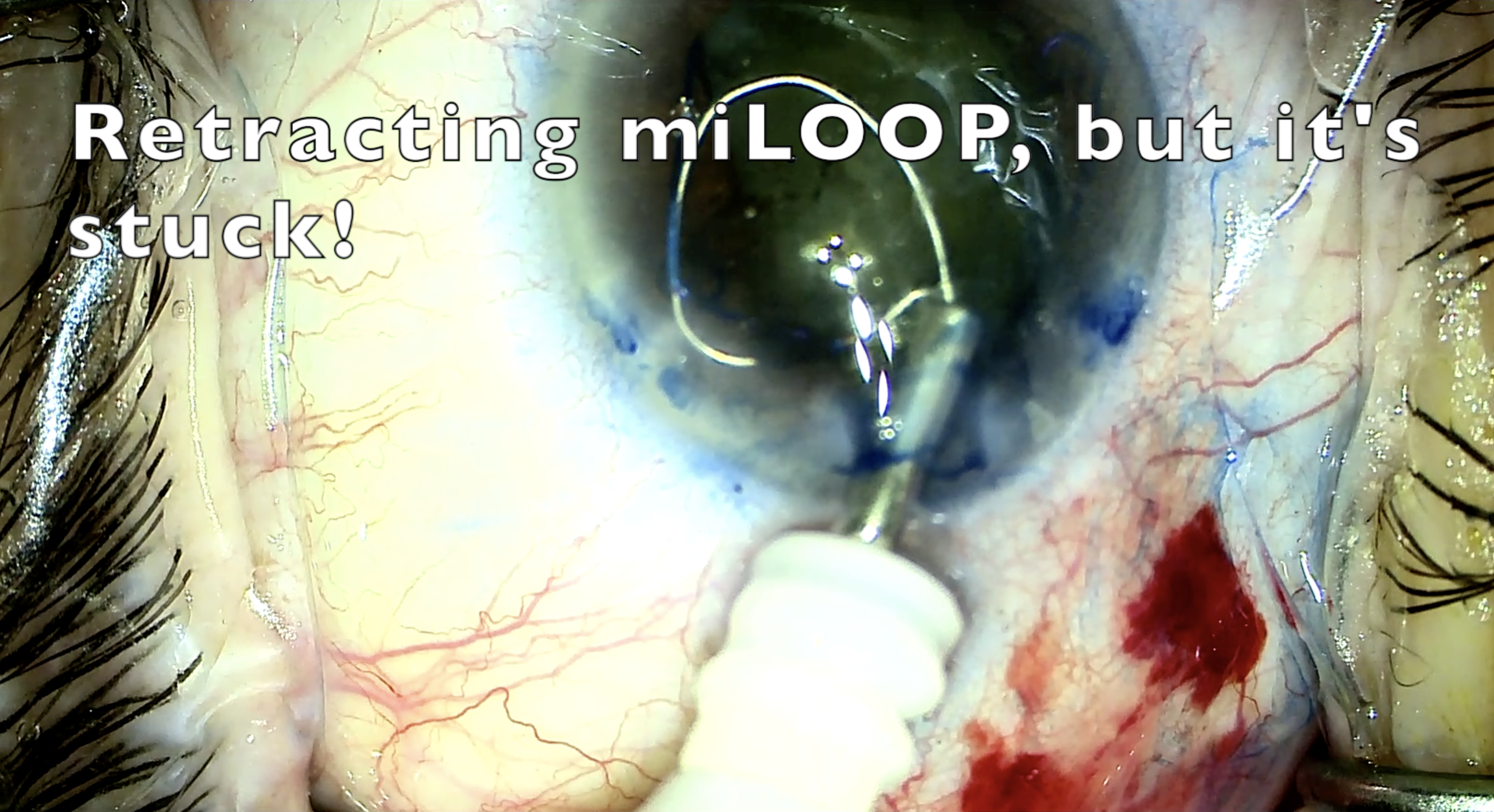
Image 4
This took time, patience, and the help of a second set of eyes (my fellow) to work. If that maneuver had not been successful, I planned to cut the nitinol loop and Malyugin Ring loop with microsurgical scissors. In retrospect, I should have retracted the miLOOP much slower and taken care to keep it far from the Malyugin Ring edge.
At this time, given the unexpected challenges of a miLOOP being in the eye at the same time as a Malyugin Ring, I chose to employ traditional phaco-chop techniques to disassemble the lens nucleus. I re-adjusted the Malyugin Ring and took time to chop the dense nucleus into smaller pieces and emulsify them at the iris plane. Additional viscoelastic was being employed constantly to protect the corneal endothelium and capsular bag.
Image 5 illustrates vertically chopping the dense nucleus.

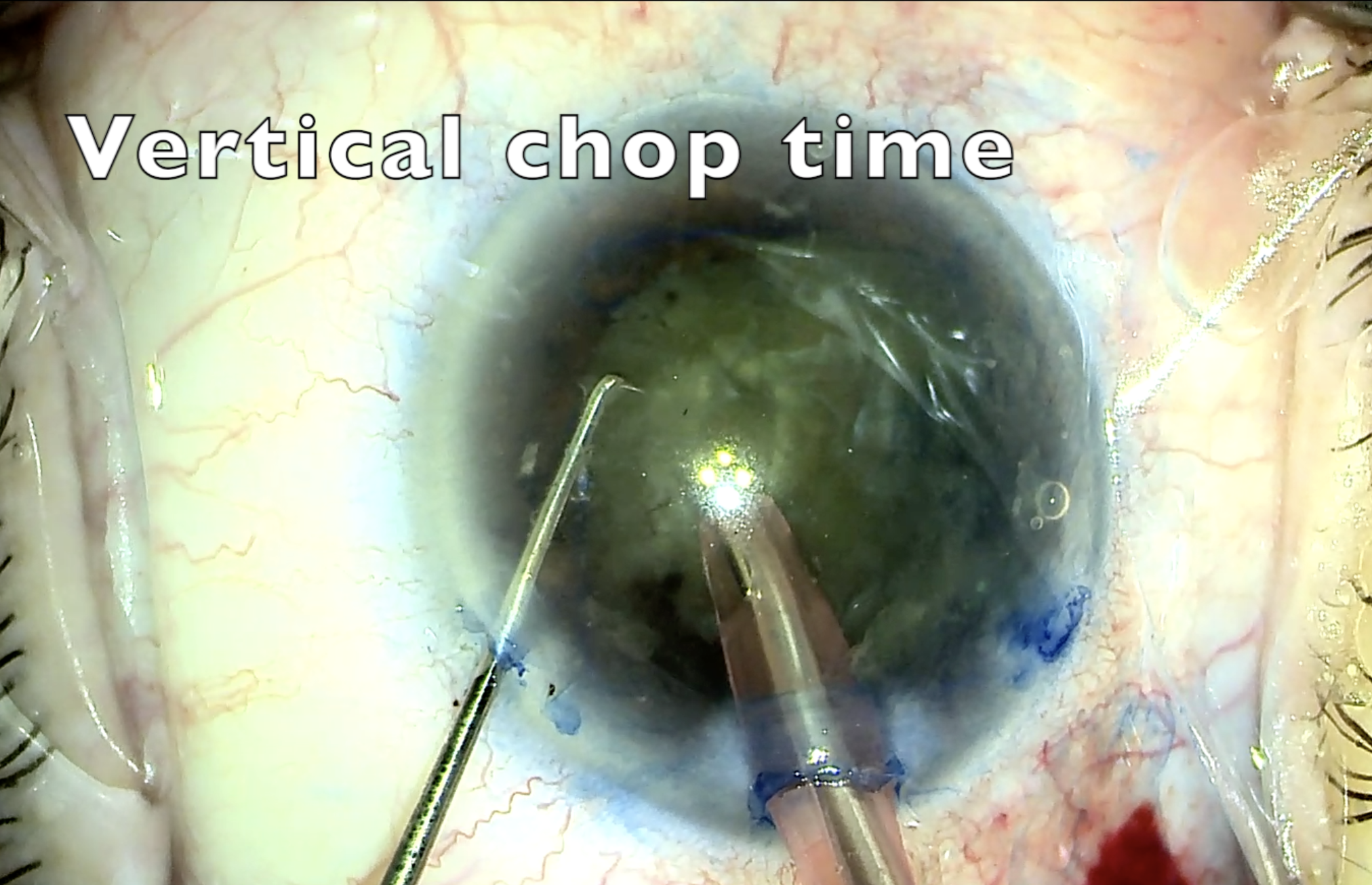
Image 5
At the end of the case, the capsular bag was noted to be intact, and a one-piece intraocular lens was placed in the bag. The Malyugin Ring was removed and all wounds were sealed at the end of the case. The patient had corneal edema postoperatively, but her vision improved steadily over 4 weeks.
Clinical pearls and takeaways
The key learning points from this case were that in eyes with small pupils, it may be wise to consider deferring the use of a miLOOP if you suspect zonulopathy or challenges deploying the miLOOP due to the large size of the lens nucleus concerning the small size of pupillary dilation.
If you do choose to use the miLOOP, take care to elevate the edge of the lens capsule with viscoelastic, visualize the miLOOP during every step of deployment, and be slow and calculated as you retract the instrument to ensure it does not entangle with an iris expansion device. It may be easier to use a miLOOP with iris hooks for iris expansion as there are no ring eyelets that the miLOOP device can get caught on.
Ultimately, safe and controlled surgery and reduction of excessive phacoemulsification energy in the eye can help patients achieve improved visual outcomes. In the patient’s fellow eye, I chose to forgo a miLOOP and was able to remove the cataract with standard phacoemulsification techniques in an uncomplicated manner.
