


Axial length
Wang-Koch adjustment formula
Axial length is considered to be the most important factor in calculating the proper intraocular lens (IOL) power, and mistakenly using an incorrect axial length can cause a “hyperopic surprise.” All optical biometers use a single index of refraction for all eyes to calculate the axial length. They all have the same intrinsic error, which increases in a linear fashion as the axial length increases; consequently, longer myopic eyes possess the largest error.
For eyes with an axial length greater than 26.00 mm, the error becomes significant and, if not adjusted, the wrong IOL implant is chosen for an eye that optically appears longer than it actually is.
Image 1, below, represents +7.00 IOL chosen Pre-Wang-Koch adjustment.

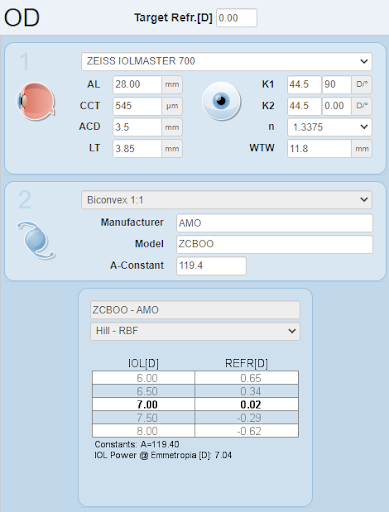
Image 1
The Wang-Koch (W-K) formula adjusts the axial length to personalize the IOL calculation. The W-K formula determines axial length (AxL) according to the following:
(measured Axial Length x 0.8289) + 4.2663
In turn, this calculation reduces the axial length to an accurate measurement. For example, when calculating an IOL for a patient with a measured axial length of 28.00 mm, the adjusted value of 27.47 is used instead.
Image 2 depicts Wang-Koch adjusted value. Note the 1.50 diopter difference between lenses calculated with and without the adjustment. A + 8.50 IOL is now chosen.

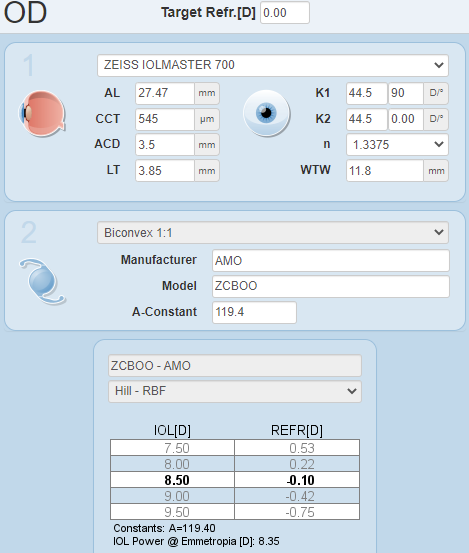
Image 2
It is important to be cognizant of the exception to the Wang-Koch formula, in that it was developed for optical biometry measurements. Alternatively, if a Wavetec ORA is used on a high myope, the W-K adjusted axial length is not used. Moreover, to achieve a precise outcome, we recommend using a capsular tension ring (CTR) in all eyes with an axial length >26.00 mm. We believe the CTR stabilizes the lens bag complex in its Effective Lens Position (EPL) making IOL calculations more accurate.
Keratometry
Discontinue contact lenses
Corneal curvature is considered second only to axial length as the most important factor in calculating the proper IOL power. Accurate results depend on a healthy and natural ocular surface. We often see cataract patients who are still wearing contact lenses; these corneas are usually flatter than their natural corneal curvature and, to obtain the proper keratometry, contacts have to be discontinued prior to IOL calculation. Soft lenses are discontinued for 7 days and toric lenses for 14 days. For rigid gas permeable (RGP) lenses, an initial topography is done then repeated at 14 and 21 days until stability is confirmed.
Keratitis and aqueous deficiency dry eye
Aqueous deficiency dry eye with secondary keratitis can result in inaccurate keratometry. Schirmer testing with anesthetic should be done to determine the true basal aqueous tear output. We use 0.5% proparacaine, wipe the fornix to start at zero mm, and read the results after five minutes. More than 10 mm wetting is normal, less than 5 mm is abnormal, and 5–10 mm is low but, without keratitis, is considered normal enough for a cataract work-up.
When checking for keratitis, we use rose bengal or lissamine green vital dyes to uncover devitalized and degenerate epithelial cells. Fluorescein permeates into the epithelial intercellular space to uncover cell disruption. All keratitis must be treated before accurate keratometry can be obtained for IOL calculation.
Blepharitis and lipid deficiency dry eye
Blepharitis and meibomian gland dysfunction (MGD) will harbor an abnormally high bacterial count with a poor tear lipid component. A serrated lid margin with scruff, collarettes, and cylinder around the lash base suggests an infestation of Demodex folliculorum in the subcutaneous eyelash shaft. A Rapid Tear Break-Up Time (RTBUT) of less than five seconds is consistent with lipid-deficient dry eye and probable MGD.
Demodex mites die after only a few weeks and their decomposing bodies deposit bacterial flora onto the lid margin, which migrates into the meibomian glands and the glands of Zeis, reducing lipid production. This affects the ocular surface causing keratitis. All blepharitis must be treated preoperatively to obtain accurate keratometry and also to reduce the threat of bacterial endophthalmitis.
Sources of hyperopic surprise
Prior unreported keratorefractive surgery
Always question cataract patients directly about any previous keratorefractive surgery. Patients may forget to report this in their office intake form, but previous corneal refractive surgery will result in an IOL power hyperopic surprise. Although post radial keratotomy (RK), automated lamellar keratoplasty (ALK), and laser-assisted in-situ keratomileusis (LASIK) corneas can be easily identified at the slit lamp, photorefractive keratectomy (PRK) corneas often appear untouched and clear.
Topography and tomographies (in our office, we use Pentacam) are done for all our cataract consultations. An unusually flat or steep cornea will reveal previous corneal surgery not mentioned by the patient. We then calculate the IOL with the Haigis and the American Society of Cataract & Refractive Surgeons (ASCRS) calculators. Then (with one exception), we always confirm the IOL power with intraoperative aberrometry (e.g., Wavetec ORA, Alcon, Fort Worth TX).
The exception is post-RK where we consider Wavetec ORA results inaccurate.
The rise and fall of the IOP during cataract surgery often opens the radial incisions, creating an irregular flattening and making WaveTec readings unreliable. The incisions eventually close over four to six weeks, but intraoperatively the reading is inaccurate. For this reason, we do not use the WaveTec ORA on any post-RK patients.
Radial keratotomy (RK)
RK has been in the US since the early 1980s, and now many post-op RK patients have developed cataracts. IOL programs on RK patients will result in a hyperopic surprise, unless the proper adjustments are performed. The ASCRS calculator does well for post RK IOL calculations.
Image 3 shows splayed RK incisions, five weeks post-op.

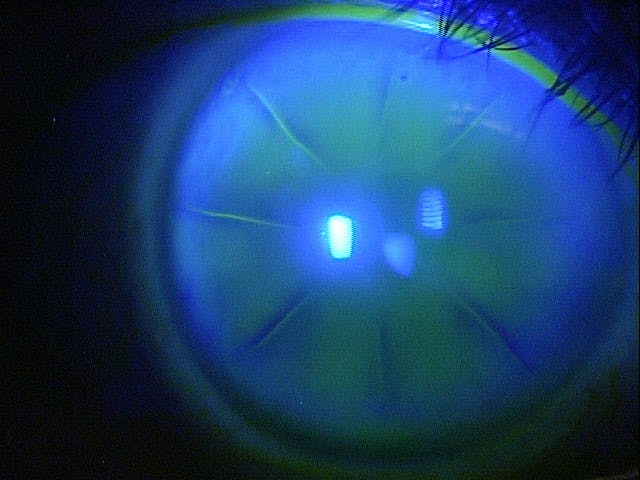
Image 3
It should be noted that, when planning for a plano result, my rule of thumb is to calculate the IOL for a -0.50D result if the keratometry is greater than 41.00D. If the keratometry is less than 41.00D, calculate for a postoperative result of -0.75D. The RK incisions are easy to identify during slit-lamp examination and, as mentioned above, can splay open during anterior segment surgery causing an immediate flattening and transient hyperopic outcome, which regresses over four to six weeks.
Toric IOLs
Astigmatic correction is very rewarding to cataract patients. With current technology, good outcomes are achievable, but great results are more difficult. Without a Callisto system, there are two things we can do to improve precision. First, overcorrect the against-the-rule (ATR) astigmatic component of the IOL. Second, consider the posterior corneal curvature as part of the toric calculation.
Overcorrecting ATR astigmatic component of the toric IOL
To achieve the planned astigmatic correction, the IOL needs to be exactly in line with corneal astigmatism. Unavoidable small misalignments are intrinsic to astigmatic lens orientation because limbal marking is inexact. Ink marks are generally too wide, not precise, and span over 5 degrees.
If the IOL is positioned off-axis, the spherical power remains the same but the astigmatic power decreases by 3% for every one degree of misalignment. A 5-degree off-axis placement reduces the astigmatic power by 15 % which can be significant for an intended correction of 2.00D or more. For example, a 2.25D toric lens placed off-axis by five degrees loses 0.33D of astigmatic correction, and a 3.50 diopter toric lens loses 0.52D of astigmatic correction.
With handheld toric markers, a 5-degree axis deviation is very conservative. For ATR astigmatism, we found increasing the astigmatic component of the IOL to the next higher cylinder power can compensate for any unavoidable off-axis positioning. For ATR astigmatism, if the toric IOL program says to use a +2.25D toric IOL, we prefer to choose a +3.00D toric lens. If the program calls for a +3.00D, we use a +3.75D, etc. With-the-rule (WTR) corrections generally do not need to be changed.
Considering posterior astigmatism in the toric IOL calculation
Unless both the anterior and posterior corneal surfaces are measured, the total astigmatic corneal refractive power may not be accounted for. For standard IOL calculations, the cornea is assumed to be a perfect sphere with a fixed anterior to posterior curvature ratio of 1:1.
Actually, the posterior curvature is not the same as the anterior and, with age, the anterior curvature drifts towards ATR while the posterior curvature remains unchanged. If the posterior astigmatism axis is in line with the measured anterior astigmatic axis, then the posterior curvature reduces the measured anterior astigmatism.
If a toric IOL is based on the anterior curvature, only then with WTR astigmatism a calculation overcorrection can result. If the posterior astigmatism axis is 90 degrees away from the anterior astigmatism, then the astigmatism measured from the anterior surface is less than the true total corneal astigmatism. In that case, an under-correction will result. This would be more significant for ATR corrections.
In Image 4, Pentacam imaging reveals a significant difference between the measured surface keratometry (0.80) and the total keratometry (2.60 ) which includes the posterior curvature in a post-LASIK patient.

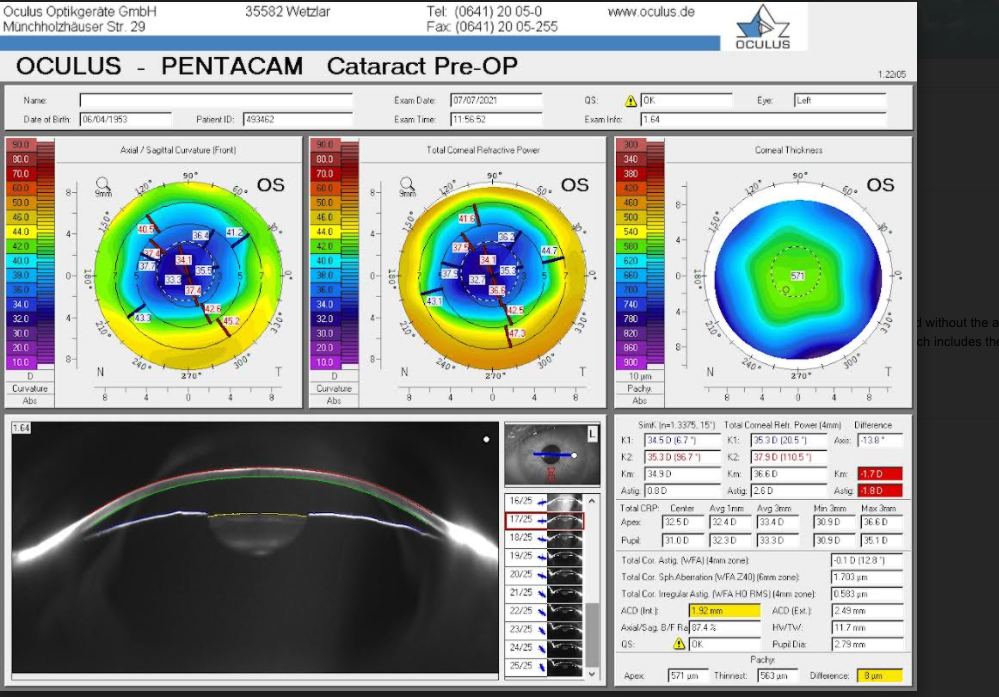
Image 4
For toric lenses, the posterior astigmatic values should be considered before deciding on a proper astigmatic IOL power. Usually, there’s only a slight difference between anterior and posterior astigmatism (0.33 diopters) but occasionally it can be significant resulting in astigmatic under-corrections or overcorrections.
We arbitrarily use greater than a one diopter anterior-posterior astigmatic difference as a cutoff for including the posterior curvature value in deciding which toric power to use.
Multifocal premium IOLs
As a general pearl, whatever time you spend with your patient during your preoperative cataract consultation, double it when discussing premium IOLs. It’s most important to understand your patients’ expectations and be sure these expectations are realistic and achievable.
Examine patients for ocular surface disease, pseudoexfoliation, and macular disease (e.g., drusen). Be sure total corneal irregular astigmatism is less than 0.300um. All premium lenses are aspheric to control chromatic aberration, so be sure the respective total corneal spherical aberration is between 1.00um and 3.00um. These features minutely affect the quality of vision but can add to ghosting, glare, halos, and overall patient dissatisfaction.
Finally, without correction, myopes are able to read and perform near-activities well. Premium lenses do not provide the same uncorrected near vision they’re accustomed to, and these myopic patients may complain that “I read better before the surgery without my glasses than I can now.” For this reason, we discourage premium IOLs in low-to-moderate myopes with a low-grade cataract; similarly, due to the added risk of postoperative peripheral retinopathy, we never offer young myopic patients multifocal clear lensectomy surgery.
On the other hand, uncorrected hyperopes are significantly less difficult to satisfy. Hyperopic uncorrected distance vision is poor and near is worse so overall, they’re easier to please. Multifocal implant lenses can be very rewarding when used in the appropriate patient. So, for a premium lens consultation, we always ensure the right premium IOL is selected for the right patient.
