


“Doc, does my high blood pressure have anything to do with my eye pressure?” As a glaucoma specialist, this is a question I get on a nearly daily basis. While the answer to that specific question is a little complicated (see below), there is an expansive list of systemic diseases and disorders known to be associated with glaucoma. Eyecare providers should be knowledgeable about these common conditions in order to counsel patients in a holistic fashion, as well as effectively co-manage with specialists in other fields.
What is glaucoma?
Glaucoma is an umbrella term used to encompass a variety of distinct conditions, which result in vision loss due to progressive optic neuropathy. Elevated eye pressure remains the most studied and best understood risk factor for the development of glaucoma, but many other pressure-independent factors exist. Oxidative and inflammatory damage, ischemic insults, mechanical pressure, and anatomic anomalies are among the lesser understood mechanisms for disease progression. In these instances, managing eye pressure alone is sufficient in limiting progression, and the underlying systemic disease must be addressed as well.
Blood pressure and glaucoma
The nuanced relationship between blood pressure (BP) and intraocular pressure (IOP) remains an active area of investigation. At the heart of this interplay between BP and IOP, is the ocular perfusion pressure (OPP), calculated as the difference between mean blood pressure and intraocular pressure. Fluctuations in OPP from high or low BP can lead to unstable ocular blood flow, insufficient oxygen supply, and oxidative stress, all culminating in optic nerve damage.1
A review of the literature yields some modest evidence that elevated BP may be related to IOP.2 A systematic review and meta-analyses by Zhao et al showed that nearly all of the 60 worldwide studies reviewed demonstrated a positive association between BP and IOP.3 The pooled average increase in IOP associated with a 10 mm Hg increase in systolic BP was 0.26 mm Hg, with the average increase associated with a 5 mm Hg increase in diastolic BP corresponding to an increase of 0.17 mm Hg. In other words, an increase of 40 mmHg in systolic BP would be required to raise IOP by 1 mm Hg.
The data regarding the effect of low BP and glaucoma progression is more compelling. Specifically, in normal-tension glaucoma (NTG) population, the evidence supports that nocturnal dips in systolic blood pressure are associated with worsening optic neuropathy and corresponding visual field loss.
While a 10% to 20% drop in systolic BP during sleep has been cited as physiologically normal,4 Bowe et al reported that dips greater than 10% were associated with increased visual field loss in glaucoma patients.5 Pillunat et al actually reported a possible protective effect of daytime elevated BP against nocturnal blood pressure dips, with less visual field loss as compared to patients with normal daytime blood pressure.6
In summary, the effect of elevated BP on glaucoma is modest at best, and the more detrimental impact to the optic nerve appears to come from low BP, particularly while we sleep.
Sleep apnea
Obstructive sleep apnea-hypopnea syndrome is becoming widely accepted as a risk factor for glaucoma. The relationship is thought to be multi-factorial including:7
- Disruptions to optic nerve head blood flow
- Increased oxidative stress and inflammation due to recurrent hypoxia
- Increased IOP and/or ICP at night related to supine position and obesity
The detrimental effect appears to even greater in those with severe disease with an apnea-hypopnea index (AHI) >30, and especially in those with NTG.
Diabetes
The sequence of events beginning with poorly controlled diabetes, retinal ischemia, and neovascularization leading due to glaucoma, is well described. However, the relationship between moderately or even well-controlled diabetes and glaucoma remains controversial, despite multiple mechanistic links connecting the pathophysiology of diabetes and glaucoma.8
Pseudoexfoliation
Pseudoexfoliation syndrome (PXFS) is an age-related systemic disease that mainly affects the anterior structures of the eye, in which exfoliative material is composed of abnormal cross-linked fibrils accumulates progressively in organs such as the heart, blood vessels, lungs, or meninges. In the eye, this exfoliative material accumulates in the trabecular meshwork, increasing resistance to aqueous outflow and resulting in higher IOP and glaucoma.
The exact pathophysiological process still remains unclear, but LOXL1 gene polymorphisms, responsible for the metabolism of some components of elastic fibers and extracellular matrix, have been associated with PXFS. Ophthalmological manifestations of PXFS are commonly bilateral, however often with an asymmetric presentation, and can lead to severe visual impairment and blindness more frequently than in the general population (Images 1 &2).9
Notably, studies have demonstrated higher serum levels of homocysteine in PXFS patients, which have also been associated with Alzheimer’s disease, heart attack, and stroke.10
In image 1, pseudoexfolialative material is seen as a white substance accumulated on the anterior lens capsule.

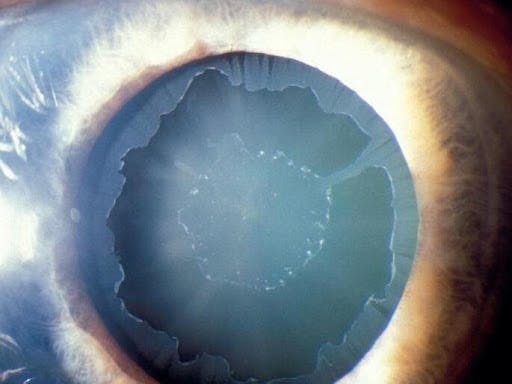
Image 1
Image 2 illustrates a characteristic heavily pigmented trabecular meshwork (White arrows) can be commonly seen in PXFS. Pigmentation anterior to the trabecular meshwork can also be seen and is referred to as a “Sampaolesi line” (Black arrows). The elevated IOP in PXFS is likely secondary to deposits of fibrillar material in the aqueous outflow drainage pathways.


Image 2
Inflammatory and infectious
Ocular inflammation and infection are important causes of increased IOP and resultant glaucoma (Table 1). Systemic inflammatory and autoimmune syndromes can commonly involve ocular structures, making a detailed medical history important in all glaucoma evaluations. The accepted mechanism of the disease involves trabecular meshwork obstruction from an accumulation of inflammatory and immune-mediated debris, leading to elevated IOP. Persistent ocular inflammation can also result in secondary angle-closure glaucoma, due to both anterior synechiae as well as iris bombe/pupillary block from posterior synechiae.
| Inflammatory | Infectious |
|---|---|
| Behcet's Disease | AIDS |
| HLA B27 related uveitis | Lyme Disease |
| Juvenile idiopathic arthritis-associated uveitis | Cytomegalovirus |
| Sarcoidosis | Onchocerciasis |
| Vogt-Koyanagi-Harada syndrome | Congenital Rubella |
| Syphilis | |
| Disseminated meningococcemia | |
| Toxocariasis | |
| Leprosy | |
| Toxoplasmosis | |
| Herpes virus-associated uveitis |
Congenital syndromes
A variety of genetic syndromes have been associated with elevated IOP and glaucoma. Glaucoma associated with these syndromes typically presents in childhood and may be more difficult to treat relative to glaucoma in adults. Given the younger age of presentation in these patients, a careful exam under anesthesia may be required to establish a diagnosis.
Any of the classic triad of “photophobia, epiphora, or blepharospasm” may indicate congenital glaucoma, and an urgent referral to a specialist should be made. Early surgical intervention is often required for these patients, as they typically do not respond well to medical treatment alone.
Congenital systemic disorders that can cause glaucoma:
- Axenfeld-Reiger syndrome
- Crouzon syndrome
- Patau syndrome
- Edward syndrome
- Down’s syndrome
- Turner syndrome
- Juvenile Hypothyroidism
- Cystinosis
- Goldenhar’s syndrome
- Diamond-Blackfan syndrome
- Ehlers-Danlos syndrome
- Lowe syndrome
- Marfan syndrome
- Mucopolysaccharoidosis
- Neurofibromatosis
- Oculodermal melanocytosis
- PHACES syndrome
- Pierre Robin syndrome
- Prader-Willi syndrome
- Stickler syndrome
- Treacher Collins syndrome
- Von Hippel-Lindau syndrome
- Weil-Marchesani syndrome
- Zellweger syndrome
Medication induced
With increasing life span, the prevalence of chronic systemic disease requiring treatment is increasing. Two-thirds of all US adults aged 49-64 and 90% of individuals 65 or older have been prescribed five or medications at a time.11 Several classes of medications are thought to increase glaucoma risk, both through IOP and IOP independent mechanisms (Table 3).
Of particular importance is the well-established effect of corticosteroids in raising IOP and precipitating glaucoma in a fraction of patients who require chronic systemic or topical steroid use, including oral steroids, nasal sprays for allergies or pulmonary conditions, and steroid creams for skin conditions like eczema and psoriasis.
Medications known to increase the risk of acute angle-closure glaucoma include anticholinergics (most commonly contained in over-the-counter antihistamines and decongestants), adrenergics, sulfonamides, and anti-depressants. These medications can result in a sudden rise in eye pressure to dangerous levels, resulting in pain, blurry vision, and possible permanent optic nerve damage if not treated emergently.12
Beta-blockers, commonly used in the treatment of blood pressure and arrhythmias, have been demonstrated to lower IOP and possibly offer a protective effect against glaucoma.13 Additional mixed evidence exists, demonstrating possible protective effects of metformin, statins, and calcium channel blockers.14
Systemic medications that may increase risk of glaucoma:
- Corticosteroids
- Anticholinergics
- Adrenergics
- Cholingergics
- Sulfonamides
Management
While the mainstay of glaucoma treatment remains controlling IOP, both medically and surgery, in instances of underlying systemic disease, this must also be addressed. While I recommend patients work with their primary care provider or other specialists to improve their blood pressure control, there is still no clear evidence that blood pressure treatment alone can slow down the progression of glaucoma.
In my own practice, particularly for my NTG patients who seem to be progressing despite well-controlled IOP, I send them for both a sleep study as well as ambulatory/nocturnal blood pressure monitoring. Interventions such as changing the timing of blood pressure medication dosing to avoid nocturnal dips, as well as the use of CPAP for sleep apnea treatment, represent a holistic approach to treating a difficult disease.
For my PXFS glaucoma patients, I am careful to ask about risk factors for heart disease and stroke, as PXFS in itself increases those risks, and I will encourage them to work with their other doctors to optimize those risk factors.
In patients with underlying inflammatory or infectious disease, working with uveitis, rheumatology, and infectious disease specialists is crucial for an integrated treatment approach. These patients are at particularly high risk for a superimposed steroid responsive glaucoma, and close monitoring of IOP and frequent glaucoma testing is necessary particularly if long-term steroids are required. In instances where patients are actively losing vision, exploration of steroid-sparing therapy may be important and can be guided by rheumatology.
In instances where systemic mediations appear to be worsening a patient’s glaucoma, communicating your concerns to the patient’s other doctors are important, and often alternate medications may be an option.
Conclusions
While treatment of IOP remains the primary modifiable risk factor in glaucoma, a variety of underlying systemic diseases as well as systemic medications, have been demonstrated to play a role in worsening glaucomatous optic neuropathy. Recognizing and addressing these underlying factors, with the help of primary care providers and specialists in other fields, is imperative for optimal glaucoma treatment.
I encourage all eyecare professionals to take the time to review all of their patient’s medical history and be proactive in helping educate patients on the interplay between their systemic conditions and their eye health.
Understanding how your front-line colleagues approach glaucoma is more important than ever. Download Eyes On Eyecare's free 2024 Glaucoma Report to see how your colleagues diagnose, treat, and manage this condition!
References
- Flammer J, Konieczka K, Bruno RM, Virdis A, Flammer AJ, Taddei S. The eye and the heart.Eur Heart J. 2013; 34:1270–1278. doi: 10.1093/eurheartj/eht023
- Leeman M, Kestelyn P. Glaucoma and Blood Pressure. Hypertension. 2019;73:944–950
- Zhao D, Cho J, Kim MH, Guallar E. The association of blood pressure and primary open-angle glaucoma: a meta-analysis.Am J Ophthalmol. 2014; 158:615.e9–27.e9. doi: 10.1016/j.ajo.2014.05.029
- World J Cardiol. 2015 Jul 26; 7(7): 373–376. Published online 2015 Jul 26. doi: 10.4330/wjc.v7.i7.373
- Bowe A, Grünig M, Schubert J, Demir M, Hoffmann V, Kütting F, Pelc A, Steffen HM. Circadian variation in arterial blood pressure and glaucomatous optic neuropathy–A systematic review and meta-analysis.Am J Hypertens. 2015; 28:1077–1082. doi: 10.1093/ajh/hpv016
- Pillunat KR, Spoerl E, Jasper C, Furashova O, Hermann C, Borrmann A, Passauer J, Middeke M, Pillunat LE. Nocturnal blood pressure in primary open-angle glaucoma.Acta Ophthalmol. 2015; 93:e621–e626. doi: 10.1111/aos.12740
- Pérez-Rico, C., Gutiérrez-Díaz, E., Mencía-Gutiérrez, E. et al. Obstructive sleep apnea–hypopnea syndrome (OSAHS) and glaucomatous optic neuropathy. Graefes Arch Clin Exp Ophthalmol 252, 1345–1357 (2014). https://doi.org/10.1007/s00417-014-2669-4
- Li Y, Mitchell W, Elze T, Zebardast N. Association Between Diabetes, Diabetic Retinopathy, and Glaucoma. Curr Diab Rep. 2021 Sep 8;21(10):38. doi: 10.1007/s11892-021-01404-5. PMID: 34495413.
- Courtesy of Wallace L.M. Alward, MD. From the Iowa Glaucoma Curriculum [curriculum.iowaglaucoma.org]. © The University of Iowa.
- Leibovitch I, Kurtz S, Shemesh G et al. Hyperhomecystinemia in pseudoexfoliation glaucoma. J Glaucoma 2003; 12:36-39.
- Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in prescription drugs use among adults in the United States from 1999-2012. JAMA. 2015;314:1818-31.
- Wu A, Khawaja AP, Pasquale LR, Stein JD. A review of systemic medications that may modulate the risk of glaucoma. The Royal College of Ophthalmologists.2020;34:12-28
- Muskens RP, de Voogd S, Wolfs RC, et al. Systemic anti-hypertensive medication and incident open-angle glaucoma. Ophthalmology. 2007;114:2221-6.
- Wu A, Khawaja AP, Pasquale LR, Stein JD. A review of systemic medications that may modulate the risk of glaucoma. The Royal College of Ophthalmologists.2020;34:12-28
