



The topic of narrow angles is not a common one among eyecare providers and can be overlooked on many routine eye exams. Evaluation and management of narrow angle patients can be difficult due to various presentations of the condition and potential sequelae of angle closure and angle closure glaucoma. As many patients can be asymptomatic, a careful examination of angle structures and anatomy is important for patients of all ages. A detailed ocular examination is important to rule out those patients at risk for narrow angles or angle closure.
In this article, we will discuss the anatomy of the anterior chamber angle, relationship between narrow angles and glaucoma, and procedure of referring patients.
Defining a narrow angle
A narrow or occludable angle is defined as an anatomical disposition in which the trabecular meshwork cannot be seen in more than 180 degrees via gonioscopy.7 Angle closure can be categorized into primary angle closure suspect, primary angle closure, and angle closure glaucoma.
Some risk factors4,10 for occludable angles include:
- Gender: Females have a higher predisposition than males.
- Prescriptions: Hyperopes tend to have shorter axial length as compared to emmetropes and myopes.
- Increase in lens thickness: As cataract develops, the lens thickens and pushes the iris forward leading to narrowing of the angle.
- Increased age: Elderly patients have increased risk.
- Ethnicity: Inuit and East Asian populations are at higher risk.
- Family history: Those with family history of occludable angles may be higher risk
- Systemic medications: Use of topiramate, anticholinergics, and sympathomimetics can increase risk.
Types of angle closure
Angle closure4,7 is classified as primary or secondary angle closure, former commonly due to anatomical disposition, later due to known pathology.
- Primary angle closure can be due to:
- Pupillary block where apposition of lens and posterior iris leads to blockage of aqueous outflow.
- Plateau iris where the iris root inserts anteriorly.
- Secondary angle closure is due to pathology. Some conditions include:
- Cataracts.
- Neovascularization.
- Membrane obstruction.
- Developmental abnormality.
Below is a quick cheat sheet for the three most common conditions4,7
1) Angle closure suspect
- Symptoms: patient is usually asymptomatic
- Sign: narrow angles or 180 degrees of iridotrabecular apposition without glaucomatous findings
2) Angle closure4,7
- Etiology: primary vs secondary (as listed above)
- Symptoms: patient may be asymptomatic or have blurry vision
- in acute cases, patient will experience vision loss, pain, nausea and photophobia
- Sign: narrow or closed angle, elevated IOP, corneal edema, fixed dilated pupil, peripheral anterior synechiae (PAS) may be present
3) Angle closure glaucoma4,7
- Symptoms: blurry vision, pain, watery eyes, photophobia, halos around lights, nausea, vomiting
- Signs: corneal edema, fixed dilated pupil, IOP between 50 to 70 mmHg with glaucomatous damage, PAS may or may not be present
Narrow angle patients may be asymptomatic therefore it is important to take a thorough history and examination to identify patients at risk.
Assessment of anterior chamber angle
The iris inserts into the anterior side of the ciliary body and separates the aqueous compartments into the anterior and posterior chamber. Aqueous humor is formed by the ciliary processes, passes from the posterior chamber into the anterior chamber via the pupil, and then leaves the eye through the anterior chamber angle. The anterior chamber is defined as the angle formed by the iris and the cornea.
Shown in Figure 1, the structures of the angle (from posterior and anterior) are as follows:


Figure 1
Figure 2, below, is a gonioscopy view of angle structures.3

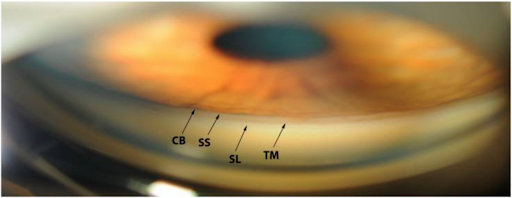
Figure 2
Figure 3 shows a gonioscopy view of an open angle: ciliary body band (purple arrow), scleral spur (blue arrow), trabecular meshwork (red arrow), Schwalbe line (yellow arrow)1

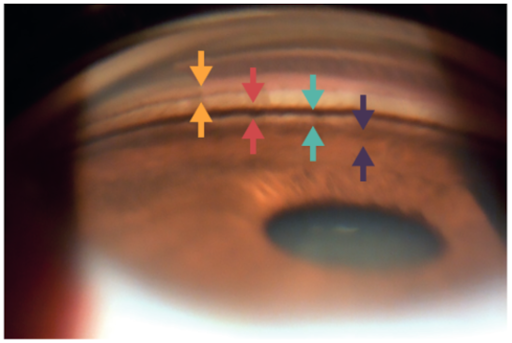
Figure 3
Clinically, it is important to note the structures present superiorly, nasally, inferiorly, and temporally. The inferior angle is usually the deepest and the most pigmented.
Grading of angle/diagnosis
The examination of anterior chamber depth (ACD) should be performed in a dark room with narrow beam of light to minimize pupillary constriction and widening of the angle.6
The Van Herick technique is an easy, non-contact technique to identify the ACD in patients and to identify those with possible occludable angles. With the illumination column of the slit lamp set at 60 degrees, a narrow beam of light is directed at the limbus to measure the ACD.3 There are two common grading scales, formerly known as the Van Herick grading and Shaffer grading scale.
Figure 4 represents the Van Herick vs Shaffer grading scale.6

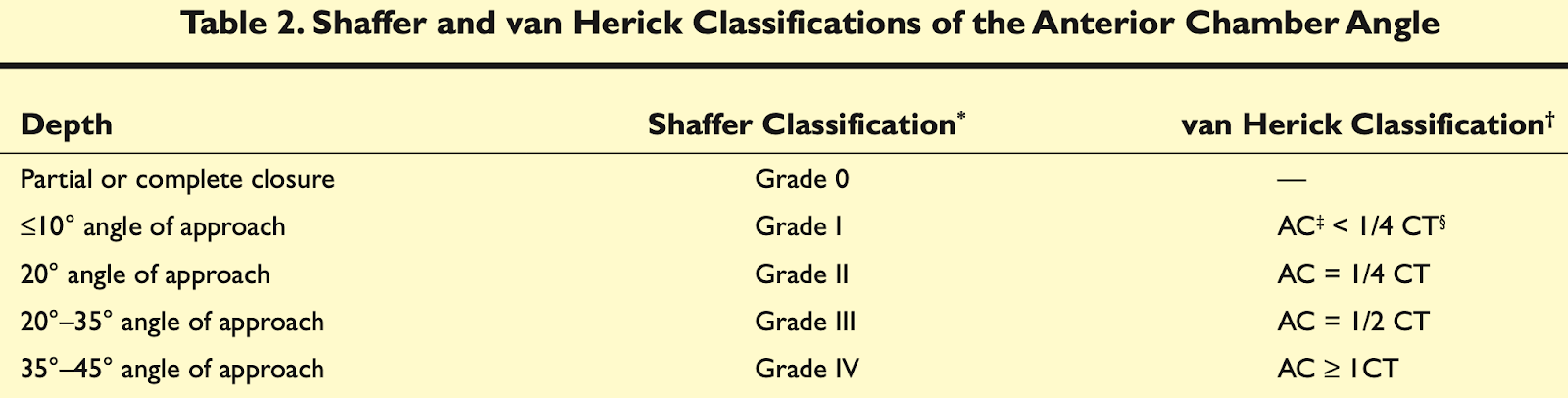
Figure 4
The Van Herick grading scale is a 4-point scale which classifies the ACD as a fraction of the corneal thickness (as mentioned above). The Shaffer classification is based on the angle of approach into the angle.
Figures 5 and 6 display theVan Herick technique.3 In Figure 5, the black band represents the limbal anterior chamber depth.


Figure 5


Figure 6
The Van Herick technique is a valuable tool for quick assessment in cases with limited access to other imaging technologies; however, it is subject to variability, therefore, this technique should not be used as a substitute for gonioscopy.
As recommended by the American Academy of Ophthalmology and the American Optometric Association,gonioscopy remains the golden standard method for evaluation of anterior chamber depth.7 Recent studies, however, show that gonioscopy is underperformed in routine visits.8 Indirect gonioscopy performed with Sussmann 4-mirror can increase the likelihood of correctly diagnosing a patient at risk for angle closure.
Although indirect gonioscopy is the recommended method, there are some instances where it is contraindicated. These include corneal surface disorders, epithelial basement membrane dystrophy, recent hyphema, suspected globe laceration or perforation.5
Ultrasound biomicroscopy (UBM) and anterior segment optical coherence tomography (AS-OCT) are useful adjunct imaging devices and may be particularly useful for patients that are non-cooperative with gonioscopy or where gonioscopy is contraindicated.3
Figure 7 of UBM shows narrow angle (a) and plateau iris (b).3

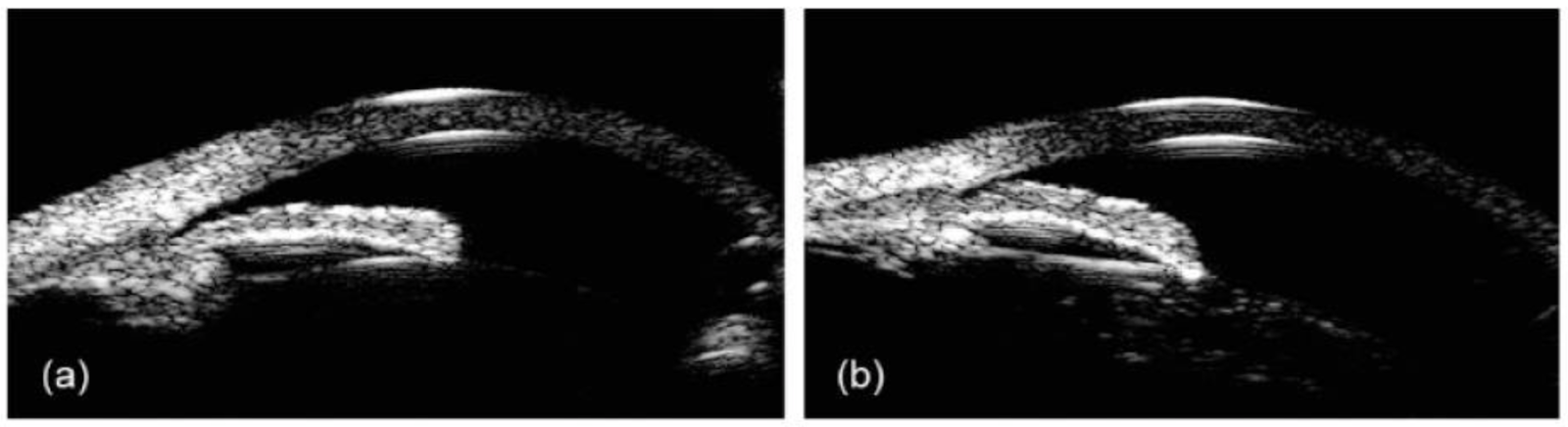
Figure 7
The AS-OCT image in Figure 8 demonstrates open angle (A) vs narrow angle (B)10

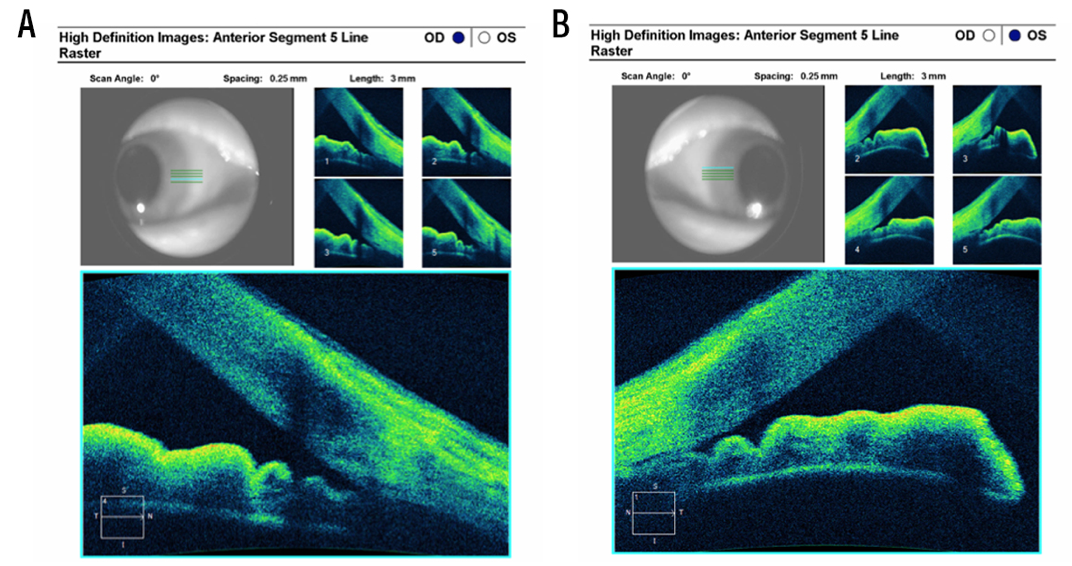
Figure 8
If gonioscopy is performed during a routine eye exam, it should be documented in notation form as shown below. Each corner of the X represents an angle, one should document the most posterior structure seen in each angle followed by the amount of pigmentation in the trabecular meshwork along with any iris abnormalities (ex: synechiae, iris approach).4,5,7 It should be noted that the inferior angle is usually most pigmented.
Figure 9 represents a notation of gonio with each angle's posterior most structure.5

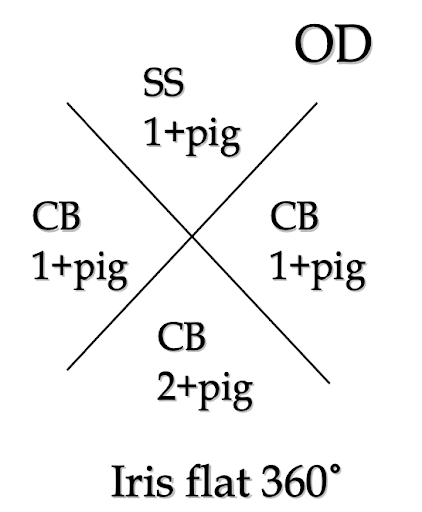
Figure 9
The relationship of narrow angles to glaucoma
The World Health Organization (WHO) ranks glaucoma as the leading cause of irreversible blindness worldwide, of which angle closure comprises half of cases.9 Primary angle closure glaucoma (PACG) is the leading cause of bilateral blindness worldwide and will affect 34 million people by 2040.9
If an angle is deemed narrow, the aqueous outflow between the anterior and posterior chamber is obstructed, leading to increased intraocular pressure. If the IOP remains elevated for an extended period, glaucoma may develop.
Clinical examination with gonioscopy is crucial to diagnose those with narrow angles or at risk of angle closure. Explaining the relationship to glaucoma enables development of trust between the clinician and the patient and helps the patient understand the importance of referral to ophthalmology if it is deemed necessary.
Referral to ophthalmology
A referral to ophthalmology is common, especially in cases where the clinician has limited access to imaging resources. Most clinicians use the Van Herick technique for quick assessment and then perform gonioscopy to ensure diagnosis before referring to ophthalmology for treatment. The referral time frame is dependent on urgency of the condition. If the patient is in acute angle closure attack, urgent referral is necessary to limit the chances of glaucomatous damage.
The consequences of not referring a patient within a given time frame may be catastrophic in certain circumstances. If the angle closure attack is not stopped, it may lead to glaucomatous damage which is irreversible. It is important to communicate all medical findings to patients to help them understand the importance of the referral to ophthalmology.
Download our FREE referral letter template!

Download our FREE referral letter template!
Make a copy of this customizable Google Doc referral letter template for easy and efficient ophthalmology referral.

Treatment & management
If angle closure attack is suspected, the first line of treatment is to reduce the intraocular pressure (IOP) to prevent glaucomatous optic neuropathy.7 Once the IOP is under control, then a laser peripheral iridotomy (LPI) can be performed. It is an in-office procedure with low risk of serious complications. In this procedure, a laser is used to create a hole at the iris in order to facilitate aqueous outflow between the posterior and anterior chambers.11 Although there is no criteria to determine whether a patient with narrow angles is high risk to perform the procedure, LPI is often performed as a preventative measure to prevent development of glaucoma.
In most states, this procedure is performed by an ophthalmologist, however, more recently laws allow optometrists in certain states to operate lasers. Listed below are the states in which optometrists can manage narrow angles using laser peripheral iridotomy:15 Alaska, Arkansas, Indiana, Kentucky, Louisiana, Mississippi, Oklahoma, and Wyoming
Another method commonly used for management of the condition is intraocular lens extraction.10 Thickening of the intraocular lens is common once cataracts develop and removal of the intraocular lens can successfully deepen the anterior chamber of the patient especially in those with angle closure or angle closure glaucoma.
In conclusion
A detailed eye examination can identify patients at risk of narrow angles or those with angle closure or angle closure glaucoma. Gonioscopy is the recommended technique for detailed examination of the anterior chamber depth; however, other imaging technologies, including ultrasound biomicroscopy and anterior segment optical coherence tomography, can be useful when gonioscopy is contraindicated.
Referral to an ophthalmologist, when necessary, should be completed promptly to prevent glaucomatous damage. Treatment usually involves laser peripheral iridotomy or intraocular lens extraction. Early detection of at risk individuals with narrow angles and preventative LPI is crucial in decreasing the possibility of glaucomatous damage from angle closure attacks.
