



From November 18 to 20, 2022, eyecare practitioners from around the world gathered online for Eyes On 2023, a 3 day educational summit offering up to 9 hours of COPE-accredited CE and CME providing the latest innovations in the ophthalmic industry.
Enjoy this presentation from Daniel Epshtein, OD, FAAO, and don't forget to check out our list of future events!
Please note these videos are provided for review only.
Optical coherence tomography angiography (OCT-A) is a noninvasive method to image ocular vasculature without the need for an injectable dye. OCT-A images the same retinal location multiple times and then detects differences between these images. Because the retina doesn’t move within the time frame of image acquisition, any detected movement correlates to blood flow. The blood flow signal is then processed to create a three-dimensional vasculature image called an OCT angiogram.
OCT-A imaging: the basics
When analyzing an OCT angiogram, movement is represented in white, and non-movement is represented in black. Unlike traditional OCT, which is viewed as cross-sections, OCT-A images are analyzed as en face slabs or straight-on, like a slit lamp examination. Many different scan sizes are available, ranging from 3x3 millimeters to 14x14 millimeters. Similar to the Raster scan in a traditional OCT, the smaller the scan size, the higher the image resolution.
Figure 1 highlights three OCT-A images taken at different scan sizes showing a normal blood flow pattern around the retina.

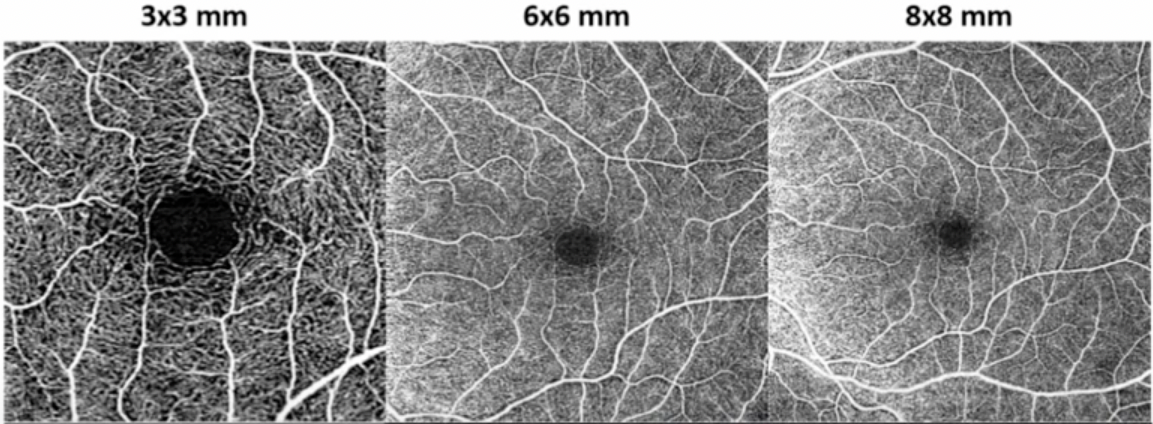
Figure 1: Image courtesy of Daniel Epshtein, OD, FAAO
OCT-A vs. dye-based angiography
When evaluating diabetic retinopathy, fluorescein angiography (FA) remains the gold standard. Currently, OCT-A is considered a noninvasive complementary imaging modality, though some of its unique features may make it preferable to FA in specific cases.
One of the benefits of OCT-A is that it uses red blood cell movement to generate a signal, whereas dye-based angiography relies on a dye that's injected into the blood.
Traditional FAs do not show the depth of signal, so when an irregular vascular area is noted, comparison to color fundus photography, funduscopic examination, or structural OCT imaging is imperative to properly analyze the FA lesion.
Using OCT-A to screen for macular degeneration
In cases of macular degeneration, OCT-A can provide unique information that FA can not. For example, a patient may present with clinically dry age-related macular degeneration (AMD). On a traditional OCT, areas of drusen would be seen, but the OCT-A may uncover neovascularization that has not leaked yet. When this is discovered, the treatment of that patient changes dramatically.
Instead of monitoring the patient every 6 to 12 months, as might be the case with dry AMD, these patients with non-leaking/nonexudative neovascular membranes should be seen every 6 to 8 weeks because these cases are 15 times more likely to convert to exudative AMD.
“From a workflow standpoint, there is a significant amount of time and preparation involved with FA that isn’t required with OCT-A.”
Because OCT-A is quick and non-invasive, it can be used as a screening tool to evaluate ocular vasculature changes. Additionally, since OCT-A relies on the movement of red blood cells, it can not visualize serous fluid. Therefore, in cases such as macular edema or central serous chorioretinopathy, FA must be used.
While OCT-A requires less preparation, if a patient has poor fixation or nystagmus, the OCT-A will show significant artifacts because it will detect fixation errors as movement and generate a blood flow pattern.
Interpreting different slab views in OCT-A
Table 1 compares various OCT-A slab views to their respective anatomic layer, expected vasculature, and indications for potential diagnoses.
| Slab | Anatomic layer | Vasculature | Utility |
|---|---|---|---|
| VRI | Anterior vitreous to ILM | None in a healthy eye | NVE in PDR and vaso-occlusive disease |
| Retina | ILM to 70 microns anterior to RPE | Superficial plexus=branches of CRA/CRV, intermediate capillary plexus, deep capillary plexus | Overview of retinal vasculature, capillary drop out/nonperfusion, foveal avascular zone visualization, microaneurysms, vessel remodeling |
| Superficial | RNFL, GCL, IPL | Superficial plexus=branches of CRA/CRV, intermediate capillary plexus | Capillary drop out/nonperfusion, foveal avascular zone visualization, microaneurysms, vessel remodeling |
| Deep | INL, OPL | Deep capillary plexus | Capillary drop out/nonperfusion, foveal avascular zone visualization, microaneurysms, vessel remodeling |
| Avascular | ONL, ELM, ellipsoid zone | None in a healthy eye | CNV, choroidal disease |
| ORCC | OPL, ONL, ELM, ellipsoid zone, RPE, choriocapillaris | None in a healthy eye | CNV, choroidal disease |
| RPE-RPE fit | Anterior RPE border (interdigitation zone) to posterior RPE border | None in a healthy eye | CNV, choroidal disease |
| Sub-RPE | Sub-RPE space | None in a healthy eye | CNV, choroidal disease |
| Choriocapillaris | Choriocapillaris | Choriocapillaris | CNV, choroidal disease |
| Choroid | Sattler's layer, Haller's layers | Sattler's layer, Haller's layers | CNV, choroidal disease |
Table 1: Image courtesy of Daniel Epshtein, OD, FAAO
Similar to traditional OCT, many of the slab views are pre-coded into the OCT-A, meaning they don’t have to be created by the user. The three most commonly used slabs analyze the retinal vascular structure, the vitreoretinal interface, and the outer retina/choriocapillaris.
Retinal vascular structure slab view
Using the retina slab, the entire vascular system within the retina can be imaged. This is important for patients who have diabetic retinopathy or any patient who is at a higher risk for retinal vascular changes.
Figure 2 shows three slabs from OCT-A highlighting the retinal vascular structure slab view.

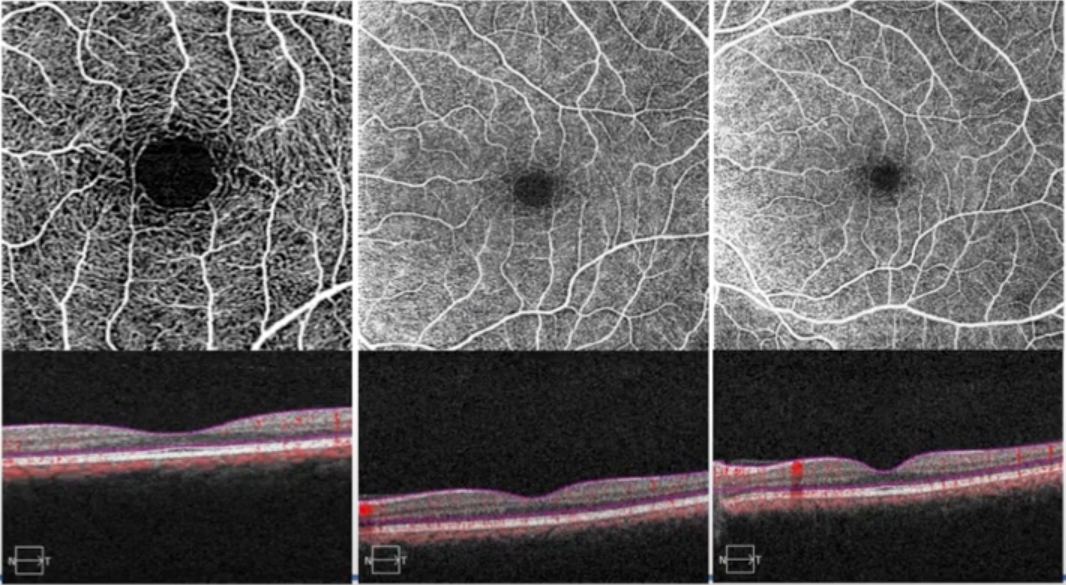
Figure 2: Image courtesy of Daniel Epshtein, OD, FAAO
Vitreoretinal interface slab view
In a normal healthy eye, the vitreoretinal interface slab shows a completely black image, indicating that there are no blood vessels on the retinal surface. Signal in the vitreoretinal slab would indicate signs of superficial neovascularization, making this view particularly valuable for proliferative diabetic patients or patients with retinal vein occlusions.
Figure 3 features OCT-A imaging of a healthy eye, with no blood vessels recorded on the retinal surface.

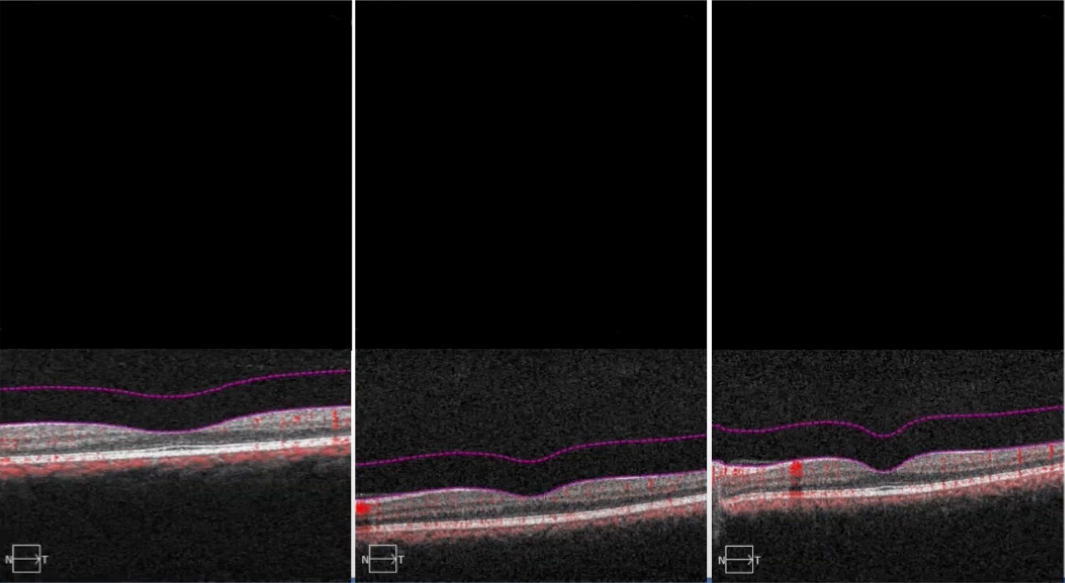
Figure 3: Image courtesy of Daniel Epshtein, OD, FAAO
Outer retina to choriocapillaris slab view
The outer retina to choriocapillaris (ORCC) slab visualizes the outer retina and choriocapillaris vasculature. This slab is valuable for patients with AMD, central serous chorioretinopathy, or any time there is a concern about neovascularization of the outer retina. This view can capture choroidal neovascularization that a basic retinal slab would miss.
Figure 4 shows the ORCC slab of a patient, highlighting choroidal neovascularization.

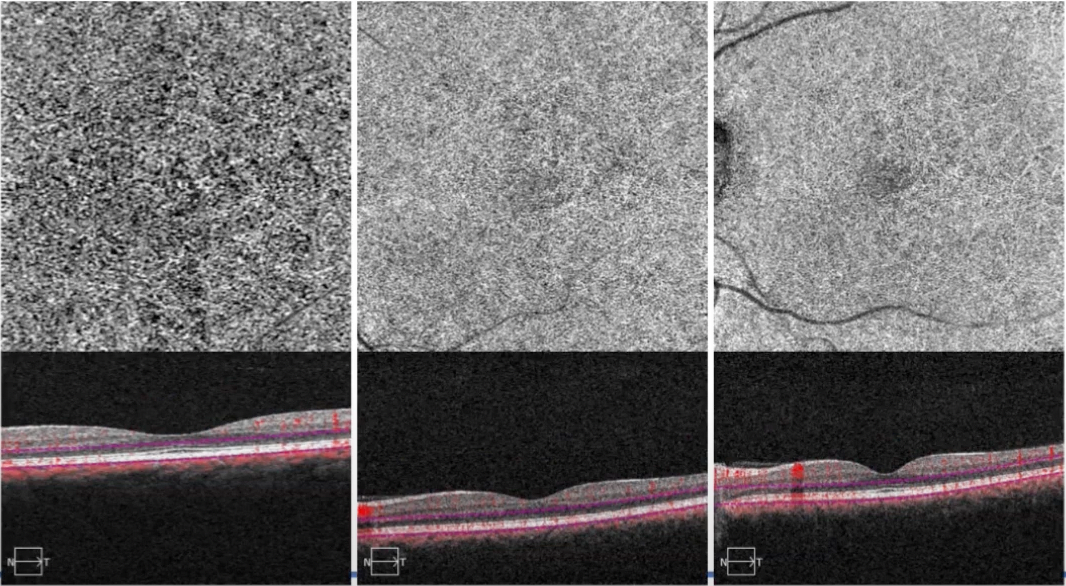
Figure 4: Image courtesy of Daniel Epshtein, OD, FAAO
Using OCT-A to screen for diabetes
One unique quality of OCT-A is that it can quantify the vascular density and foveal vascular zone, making it extremely valuable when treating diabetic patients. The retina slab can be used to quickly screen for vascular remodeling, microaneurysms, or changes in the foveal avascular zone.
“More than 3.5 times the amount of microaneurysms can be visualized on the OCT angiogram than could be seen by a traditional fundus examination.”
Enlargement and increase in non-circularity of the foveal avascular zone is a sign of worsening diabetic disease and may correlate with a reduction in contrast sensitivity. By using both the 3x3mm and the 8x8mm protocols, clinicians can visualize both high-resolution foveal changes and more widespread vascular changes.
Identifying non-proliferative diabetic retinopathy with OCT-A
OCT-A shows changes in the foveal vascular zone before there is clinical evidence of non-proliferative diabetic retinopathy (NPDR). These patients are likely at a higher risk of developing clinical NPDR in the future, but due to how new the technology is, more research is necessary to determine what preclinical diabetic retinopathy truly represents.
As OCT-A is further incorporated into treatment practices, these findings may become important biomarkers for future diabetic retinopathy classification systems and management protocols. In the future, diabetic eye disease will no longer be classified simply by the number of retinal hemorrhages that we can count but by a more comprehensive analysis of ocular vasculature with OCT-A.
Figure 5 compares OCT-A imaging of a normal retina to OCT-A imaging of progressive degeneration of the fovial avascular zone caused by non-proliferative diabetic retinopathy.


Figure 5: Image courtesy of Daniel Epshtein, OD, FAAO
Using OCT-A to screen for glaucoma
OCT-A is able to measure the vessels that nourish the nerve fiber layer, providing complementary information to traditional retinal nerve fiber layer (RNFL) thickness measurements. Though the structure-function correlation between OCT RNFL thickness measurements and visual field loss is often poor, studies have revealed that OCT-A vessel densities correlate better with visual field testing. This means that OCT-A measurements might be able to provide an objective measurement of visual function to complement visual field testing.
Glaucoma and OCT-A RNFL thickness measurements
Glaucoma is a disease of progression, and just like with structural OCT measurements, OCT-A data can also be analyzed for progression. Changes in vessel density can be detected by comparing two different OCT-A scans. While OCT RNFL thickness measurements are known to be less useful in advanced glaucoma due to the floor effect, where the patient continues to lose vision, the RNFL thickness measurements do not change.
Studies have shown that OCT-A measurements have a lower floor effect than OCT RNFL thickness measurements, possibly providing an objective measurement that can be used even in advanced stages of glaucoma.
Figure 6 features two line graphs and scatter plots, one showing the correlation between OCT-A vessel density and visual field deviation and the other showing the correlation between RNFL thickness and visual field mean deviation.

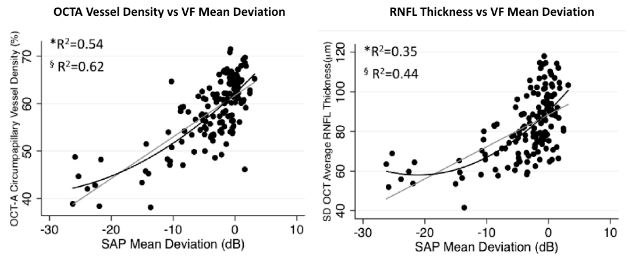
Figure 6: Image is taken from https://pubmed.ncbi.nlm.nih.gov/27726964/
Although using OCT-A measurements in glaucoma management seems to be the new frontier, it is unclear if vascular changes detected with OCT-A occur before, during, or after OCT RNFL changes. Until this is determined, it’s unknown where OCT-A will fit into protocol and glaucoma management.
Conclusion
It is important to remember that OCT-A technology is still in its infancy. A tremendous amount of data is being collected, but the best way to utilize this data is still being determined. OCT-A has already found multiple use cases in retinal and optic nerve disease. Still, it will take time until our management protocols catch up to this new frontier in ocular vasculature imaging.
