



Diabetic retinopathy is one of the quintessential ocular diseases. It’s a chronic condition without a simple cure, requires long-term management, and vigilance in patient education to achieve great outcomes. With the increasing prevalence of diabetes, diabetic retinopathy is something that all eyecare practitioners are familiar with. OCT angiography (OCTA) provides a different perspective on diabetic retinopathy, one that may move us from an era of counting hemorrhages to a future where we personalize care based on microvascular changes invisible to our funduscopic examination.
Preclinical diabetic retinopathy
The earliest signs of diabetic retinopathy—pericyte loss and vascular basement membrane thickening—occur on a cellular level. These changes eventually result in retinal vascular nonperfusion and alteration of the foveal avascular zone (FAZ). These pathological abnormalities are considered to be the preclinical signs of diabetic retinopathy because at this stage the clinical examination is completely normal. With very precise measurements of contrast sensitivity, microperimetry, or retino-electrophysiological testing the functional deficits of these preclinical retinal diabetic changes may be assessed.
Preclinical diabetic retinopathy is a relatively new concept, one that is likely to become more important due to the advent of OCTA. Whereas before, angiography was usually reserved for acutely vision-threatening pathology, OCTA allows us to perform angiography without any potential side effects within a few seconds.
Figure 1 demonstrates the power of OCTA, on the left is a normal non-diabetic patient and on the right is a 67-year-old with a 7-year history of moderately well-controlled diabetes (A1C 7.5%). His funduscopic examination is unremarkable and his best-corrected visual acuity is 20/20 in each eye. But looking at his OCTA image we can already visualize irregularity of the FAZ and areas of nonperfusion most prominent in the superior and temporal perifoveal region.
Unfortunately, there are no preferred practice guidelines on how to manage preclinical diabetic retinopathy so cases like this often leave me with more questions than answers.
Currently, images like this provide me another tool with which to convince my patients that they must continue to practice strict blood glucose control. But I believe that in the near future, OCTA data will be included in the expanded clinical classification systems of diabetic retinopathy, one which will help us provide better care for our patients.
Figure 1 shows a normal OCTA on the left and, on the right, a patient without clinical diabetic retinopathy but with OCTA changes.

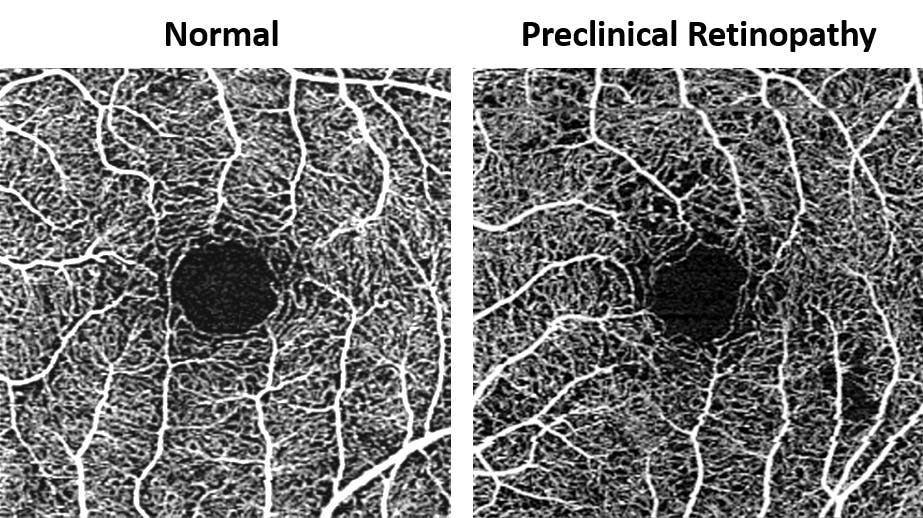
Figure 1
Nonproliferative diabetic retinopathy
The earliest clinical sign of diabetic retinopathy is the formation of focal dilatations of the vascular wall of capillaries, small arterioles, or small venules called microaneurysms. Microaneurysms form in areas of pericyte loss via hemodynamic changes and vascular endothelial proliferation. Clinically, microaneurysms appear as vessel-associated small red dots 25 to 100 μm in diameter within the posterior pole. Early on, microaneurysms are most often noted perifoveally and may have considerable turnover, with cycles of resolution and formation.
Patients with extensive microaneurysm turnover are more prone to the development of diabetic macular edema and may need to be monitored more closely. Microaneurysms can be visualized with OCTA as hyperreflective dilatations of small vessels. Much like with fluorescein angiography, OCTA will often detect more microaneurysms than a clinical exam.
In Figure 2, in a patient with moderate NPDR, note that more microaneurysms are noted with OCTA than in the fundus photograph.

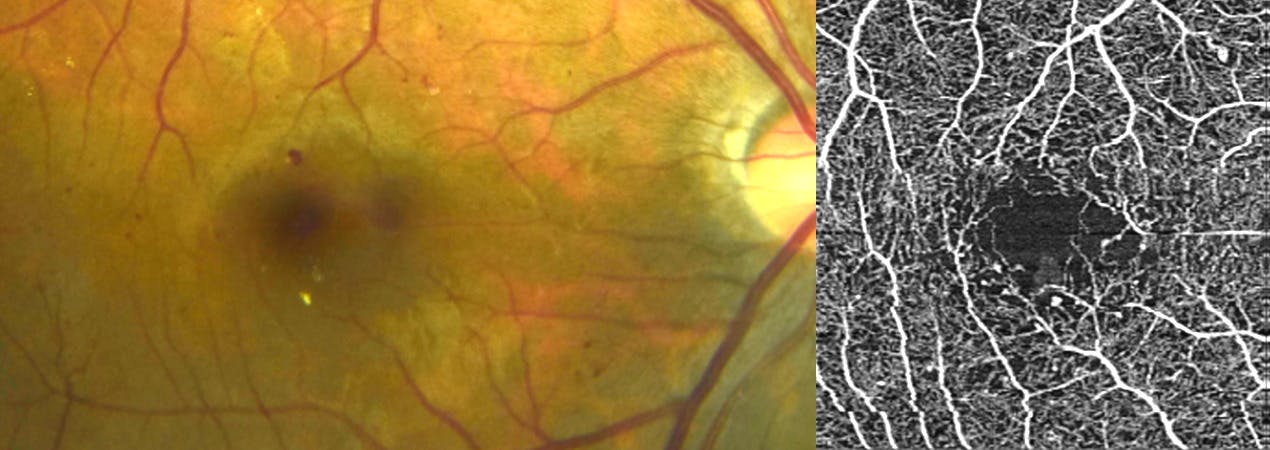
Figure 2
The FAZ will be enlarged and more eccentric in diabetic patients with NPDR than in those without retinopathy. These changes in the FAZ represent diabetic retinal degeneration and may correlate with decreased contrast sensitivity or suggest the need for tighter glycemic control. If there is significant alteration of the FAZ, patients will develop reduced visual acuity and macular atrophy (see below for diabetic macular ischemia).
Further diabetic microvascular damage leads to worsening vaso-obliteration, vascular remodeling, and hemorrhages. Intraretinal hemorrhages are usually the result of ruptured microaneurysms or leaking intraretinal microvascular abnormalities and capillaries. In cases with significant hemorrhaging, OCTA can be useful in distinguishing intraretinal hemorrhaging from neovascularization.
Figure 3 illustrates a spectrum of perifoveal OCTA findings. Note the increasing size and irregularity of the foveal avascular zone.

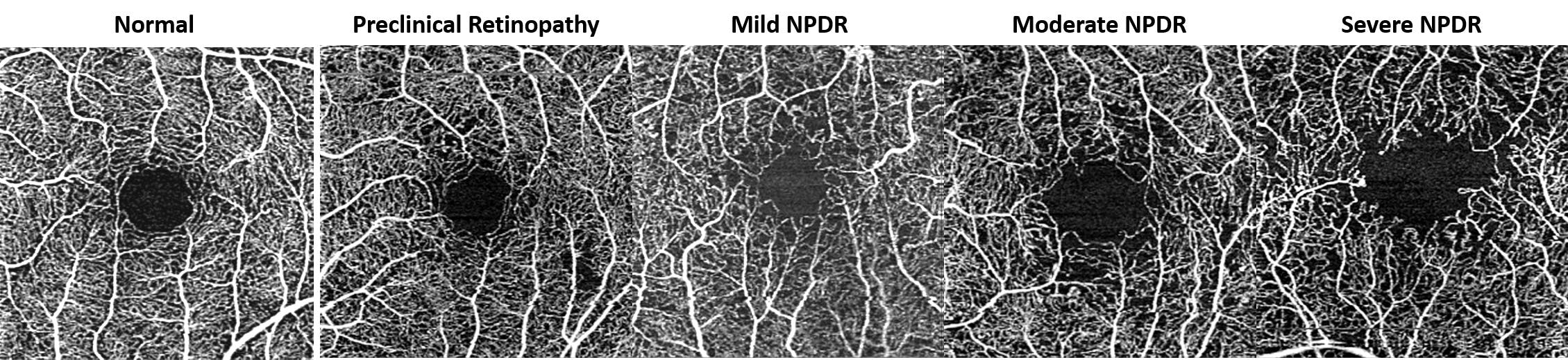
Figure 3
Proliferative diabetic retinopathy
Progressive retinal ischemia can lead to vasoproliferation on the retinal surface, optic nerve head, or anterior uvea via the release of angiogenic factors such as VEGF and platelet-derived growth factor. These highly permeable new vessels often grow on the border of perfused and non-perfused retina where they tend to hemorrhage or leak. It is important to identify these new vessels early and refer for treatment to prevent vision-threatening disease. Neovascularization of the retinal surface can be easily differentiated from hemorrhages or intraretinal vasculature by the OCTA slab in which it is detected.
Any vasculature anterior to the internal limiting membrane is considered neovascularization and immediately puts the patient in the proliferative diabetic retinopathy category. With the CIRRUS Angioplex module the vitreoretinal interface layer, which is normally black and void of signal, will have a hyperreflective lacy lesion corresponding to any neovascularization on the retinal surface. This same technique can be used for the assessment of neovascularization of the optic nerve head.
Below is one of my favorite cases ever: This is a patient with a history of proliferative diabetic retinopathy, focal laser, and intravitreal Avastin OS. The patient had not received any treatment for several years as she was deemed to have no proliferative changes. My clinical examination was exactly as the fundus photos below, a few dot blot hemorrhages but no significant signs of macular edema or neovascularization.
The patient’s vision was 20/20 OD and 20/25 OS. For this reason, I decided to order an OCT (and OCTA because why not?) to ensure I didn’t miss any diabetic macular edema or other macular pathology.
To my surprise, I noted a small hyper-reflective lesion (red circle below) in the vitreoretinal interface of the left eye. I decided to get a higher resolution of that area and was stunned to realize that what I thought was a blot hemorrhage was actually a small tuft of neovascularization elsewhere. The two almost identical blot-like red lesions in each eye seemed clinically identical to me, but with OCTA the true nature of these lesions was elucidated, altering the patient’s clinical management.
In Figure 4, we see the right eye and left eye of a patient with proliferative diabetic retinopathy in the left eye. Clinically, she seems to have dot blot hemorrhages OU as noted on fundus photography but with OCTA the blot-like red lesion in the left eye is actually a tuft of neovascularization elsewhere.

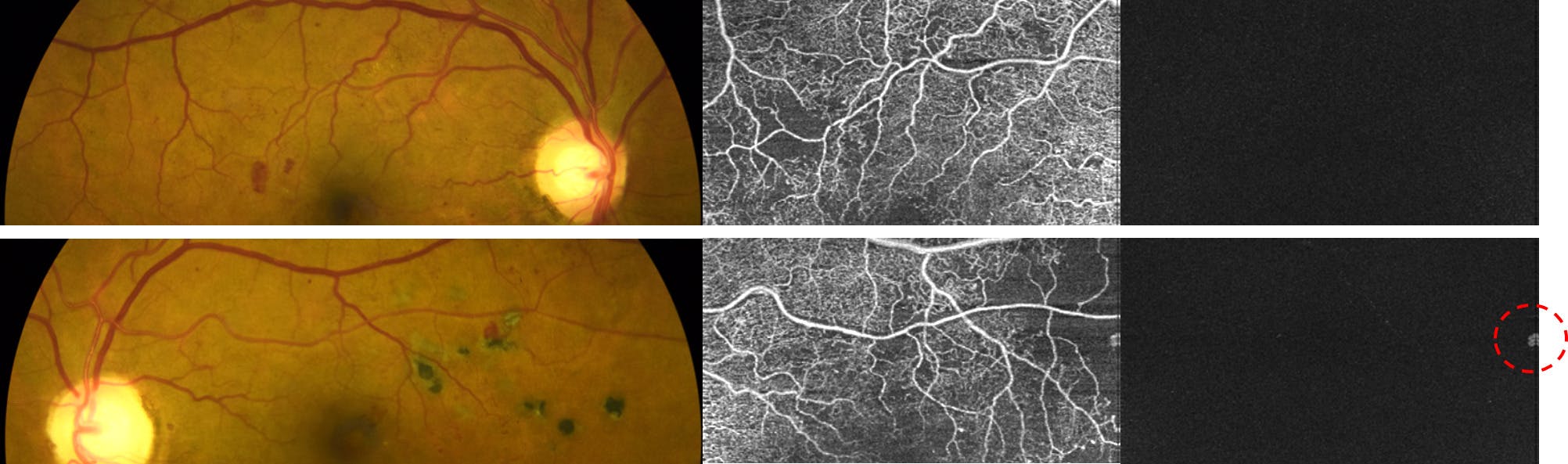


Figure 4
Diabetic macular ischemia
Patients with quiescent PDR will often present will reduced visual acuity but without active retinopathy and the visual acuity deficit will be out of proportion to the amount of macular atrophy. Structural OCT imaging might reveal diffuse macular atrophy without edema or exudation. OCTA imaging is incredibly useful in these patients because it will reveal significant macular ischemia and irregularity of the FAZ. Unfortunately, there is no treatment for macular ischemia but the identification of macular ischemia is helpful in patient education and for prognostic purposes.
Figure 5 represents a 78-year-old female with a history of proliferative diabetic retinopathy status post mild panretinal photocoagulation. She currently does not have any active retinopathy. Visual acuity in this eye is 20/40. The OCTA image reveals significant enlargement of the FAZ and the structural OCT reveals macular thinning.

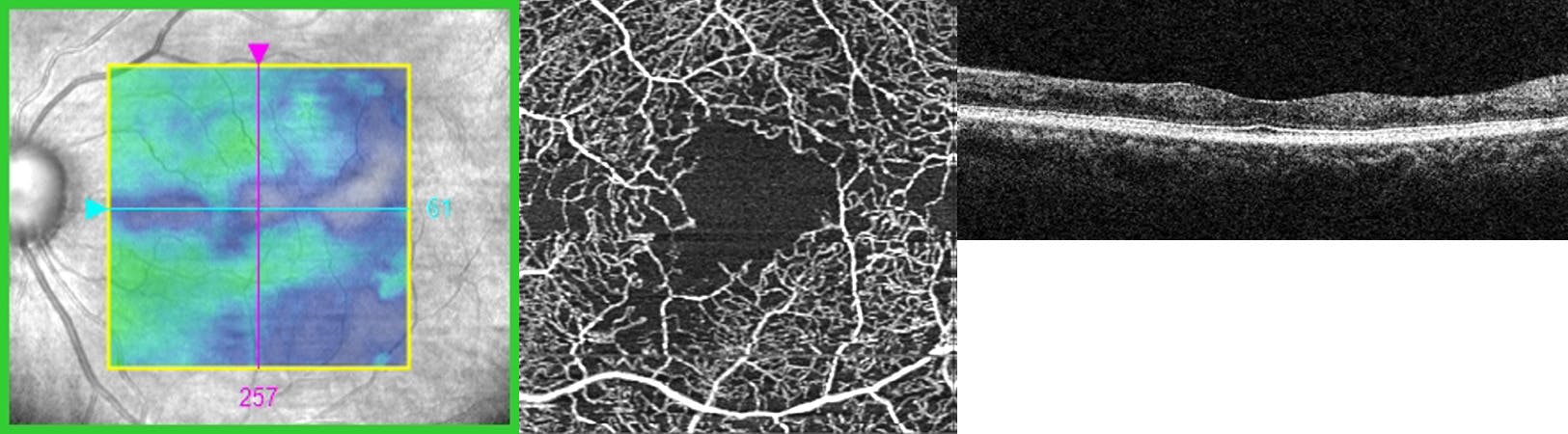
Figure 5
Conclusion
Currently, our ocular management of diabetic patients is based on risk associations between clinical findings such as the amount of hemorrhaging and the risk for vision loss from diabetic macular edema or proliferative diabetic retinopathy. Though we have done a pretty good job of implementing these clinical associations to prevent vision loss, clinical findings are not the primary insult in diabetic retinopathy.OCTA gets us closer to visualizing the primary pathology process in diabetic retinopathy, one that will hopefully allow us to better manage our patients and reduce diabetic vision loss.
We have a direct partnership with ZEISS!
