



Among the myriad of ocular conditions, there are some that are diagnostically distinct. Coats disease is a unilateral retinal disorder that is characterized by abnormal retinal vasculature formation, where aneurysms, telangiectasia, and neovascularization leads to extensive exudative retinopathy and vision loss.
Nearly all cases of Coats disease are unilateral and typically present in young males. The effect of physiological damage to capillaries, which may be due to improper development, leads to vascular malfunction. Compromise to this physiologic function can lead to abnormal vascular permeability. The affected retinal areas then broaden and bring about wide-spread exudation; consequences can be detrimental to ocular health and therefore subsequent visual outcomes.
Genetic components and risk factors
Although the etiology is unknown, there is likely no genetic predisposition. There is a theory looking into an X-chromosomal gene mutation on NDP, which has possible roles in retinal vasculature formation.1 Other genes being researched are CRB1 and PANK2. Otherwise, general discrepancies were of note in chromosome 3 and 13.2
Potential pathogenesis
The blood-retinal barrier (BRB) is a critical area that modulates how nutrients and solutes move to and from the choroid. Its breakdown can cause engorgements, weak vessels, and lipid leakage.
Studies indicate that in Coats disease, there are physiological alterations in the BRB, primarily due to damaged tight junctions and capillary endothelial cells in the inner retinal layers. Pericyte depletion also leaves room for aneurysms to develop. The following inflammation may be associated with macrophage activity in the inner layers.3
Diagnosing Coats disease
Patient population
Considering the profile of Coats disease patients, its clinical presentation (especially the vascular anomalies) tends to mimic that of diabetic retinopathy.
Although it predominantly affects males (85%) ages 18 months to 18 years old, diagnosis is usually made later, around 8 to 16 years old. Few cases appear in adulthood.
In regards to prevalence, it is a rare disorder with an incidence of 0.09 per 100,000 persons.4
Signs and symptoms
We know the importance of a comprehensive eye exam for children, but a certain indication is unilateral painless severely reduced BCVA. In fact, many Coats disease diagnoses are identified upon routine eye exams.
Clinically hallmark signs of light bulb aneurysms, telangiectasia, and massive exudation are recognizable in Coats disease presentation. Younger patients with significant progression can display leukocoria with strabismus or amblyopia.3,5
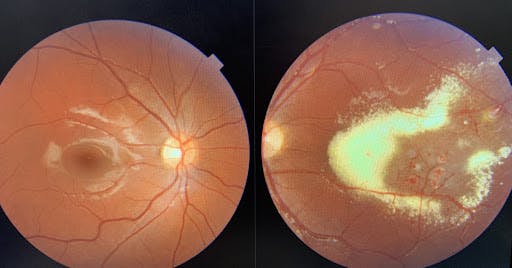
Figure 1 represents Stage 2 Coats disease with foveal exudation in a 12-year-old male presenting for a routine eye exam. The left eye exhibits large central exudation spanning to the temporal periphery with venous beading, telangiectasia, outpouching, and fusiform arteriolar dilatation.

Pertinent diagnostic findings
Early to moderate disease
Early vascular abnormalities such as tortuosity, outpouching, and capillary dropout reflect poor perfusion, interrupting how nutrients and oxygen flow to the retina. Findings such as light bulb aneurysms, telangiectasia, and venous sheathing can be found, often in the temporal quadrants.
In Stage 2, the presence of exudation increases the risk of permanent vision impairment. Its location can be intraretinal, subretinal or sub-RPE, but associated foveal edema will certainly decline visual acuity.
Severe disease
The likelihood of serous retinal detachments increases as fluid accumulates and spans to a larger magnitude. In addition, compounding vitreous hemorrhages can occur due to retinal neovasculation. Monitoring for tractional detachment is critical in these cases. Retinal fibrosis may be observed moving forward as well.
In advanced disease, total retinal detachments are detected, and secondary glaucomatous diseases can precipitate. Total irreversible blindness is classified as the end stage, where the goal is to maintain a painless, comfortable eye.
Differential diagnosis
Some retinal vascular anomalies with telanetasic nature are Leber’s miliary aneurysm, idiopathic macular telangiectasia (IMT), and familial exudative vitreoretinopathy (FEVR). Leber’s miliary aneurysm is a milder variant of Coats disease, with no (or rarely seen) fluid leakage localized to a quadrant.
Additional differentials to consider are those for younger patients with leukocoria: retinoblastoma, persistent fetal vasculature, FEVR, retinopathy of prematurity, and toxocariasis.1
Special testing considerations
For newborns and babies, the occlusion technique can convey visual acuity disparities. In all pediatric cases, a direct ophthalmoscope can reveal leukocoria, and assessing ocular alignment with the Hirschberg test is useful. When possible, checking for amsler grid defects and eccentric viewing is also beneficial.
The dilated fundus exam can provide insight on classifying the stage and severity of Coats disease. Additional testing is required for assessing the necessity and type of treatment indicated. OCT and fluorescein angiography can highlight precise exudative damage for close management by hyperfluresing abnormalities.
If a dense cataract is present, a B-SCAN ultrasound can be used to assess the posterior ocular structures. These specialty tests help guide the next steps as you refer to a pediatric ophthalmologist and/or retinal specialist for treatment.
Classifying Coats disease stages
The extent of damage depends on the stage of the condition, where progression escalates in severity. Starting with telangiectasia, the upcoming findings are exudates which penetrate foveal structions and expand in range. When left untreated or unmanaged, other more advanced conditions may arise and cause severe vision loss.
| Stages of Coats Disease | |
|---|---|
| Stage 1 | Retinal telangiectasia Retinal aneurysm Venous beading |
| Stage 2 | Telangiectasia + extrafoveal exudation Telangiectasia + foveal exudation |
| Stage 3 | Subtotal exudative retinal detachment Total exudative retinal detachment |
| Stage 4 | Total exudative retinal detachment + secondary glaucoma |
| Stage 5 | Advanced end-stage disease |
Halting or delaying additional progression is inherently the priority to diminish chances of reaching end-stage disease with irreversible vision loss.
Treatment options
In Stage 1 early detection and close monitoring is key to avoid severe ocular complications. Whether the patient is symptomatic or not, diagnosing patients at Stage 1 of the disease is uncommon. Moreover, children may not be able to articulate or understand their symptoms.
At this point, intraretinal microvascular abnormalities (IRMA) can be treated with thermal laser photocoagulation to shrink and eradicate growth of abnormal vessels. Adjunct anti-VEGF injections are also an option to diminish leakage. If the severity of presentation disqualifies laser treatment, cryotherapy would be an alternate option. With treatment, it is possible to alleviate some vision changes during these early stages.
Surgery is typically necessary in the presence of exudative retinal detachment or if secondary glaucoma is progressing. Other ocular complications can include neovascularization of anterior segment, neovascular glaucoma, cataract, uveitis, or phthisis bulbi.1 Acutely severe cases may call for enucleation to relieve a blind, painful eye.
Prognosis
By analyzing various factors, we can construct a fairly objective prognosis for the patient. Naturally, there is a poor prognosis for more advanced stages of disease. The age at diagnosis, as well as initial presentation typically determine the chances of retaining visual function and ocular integrity. What is the BCVA? Is foveal anatomy compromised? Are there pending retinal detachments?
Early detection does allow us to limit damage as promptly as needed. Nonetheless, diagnoses in older kids tend to be milder cases. While cases with younger patients tend to progress more aggressively.
In all scenarios, when reaching Stage 4, visual prognosis is not good. Sustaining a comfortable, painless eye that retains its structure is the main treatment priority.
Key takeaways
What is Coats disease?
A unilateral retinal disorder in young males cause by abnormal retinal vasculature that leads to extensive exudative retinopathy and vision loss.
Is Coats disease reversible?
In early stages, treatment can alleviate some vision changes by reducing leakage, primarily macular edema. In moderate to severe disease, most vision loss is permanent and the goal is to maintain residual vision and delay progression.
Is Coats disease inherited?
Although the etiology is unknown, it seems non-hereditary.
So, you suspect Coats disease. What next?
It is important to educate the patient that Coats disease is likely non-hereditary, but discuss the importance of routine exams for family members. There are no associated links to systemic conditions, but explain the value of routine blood work due to the gravity of possible underlying vascular dysfunction.
Further research is necessary to offer a better understanding of Coats disease and its etiologies. Although it is yet to be discovered, the retinal condition itself is unique and distinguishable, particularly due to the substantial lipid leakage.
Therein, when a significant exudative response presents in any condition, it is called a “Coats response,” which has occurrences in Turner Syndrome and retinitis pigmentosa among others.1
Conclusion
Coats disease may be a rare retinal condition, but its diagnosis is essential to preventing pathological deterioration and progressive vision loss. This highlights the significance of comprehensive eye exams in that they provide ocular health screening in your pediatric patients.
As stated above, many of these cases are noted upon a routine eye care visit, which was the case for my patient. Pediatric patients may be asymptomatic or unaware of the gravity of severe unilateral blurry vision.
It is essential to monitor and manage Coats disease closely; co-management with ophthalmology and low vision specialties is vital. Eye care practitioners should be informative and sympathetic when sharing their assessment and next steps for the patient and their family.
References
- Bagheri N, Baid S, Gregori NZ. Characteristics and management of Coats disease. American Academy of Ophthalmology. https://www.aao.org/eyenet/article/characteristics-management-of-coats-disease. Published August 2017. Accessed May 10, 2022.
- Tsakiris KX. Coats disease. EyeWiki. https://eyewiki.aao.org/Coats_Disease. Published November 22, 2021. Accessed May 13, 2022.
- Sowka, Joseph. Retinal Vascular Abnormalities. lecture presented: 2018.
- Morris B, Foot B, Mulvihill A. A population-based study of Coats Disease in the United Kingdom I: Epidemiology and clinical features at diagnosis. Eye. 2010;24(12):1797-1801. doi:10.1038/eye.2010.126
- Coats disease. NORD (National Organization for Rare Disorders). https://rarediseases.org/rare-diseases/coats-disease/. Published June 26, 2017. Accessed May 15, 2022.
