





Retinoblastoma is the most common intraocular cancer amongst the pediatric population, with an estimated incidence between 1 in 14,000 to 1 in 20,000 live births worldwide. In the United States, there are between 250 to 350 cases per year, almost exclusively in patients under 5. Treatment survival rates in developed nations exceed 95%; however, high mortality rates remain in untreated cases. In the latter, cases are often found in lower-income countries and commonly present late in the disease course.
Risk factors for retinoblastoma include age and genetics. Most children diagnosed are under the age of 3, with heritable retinoblastoma often diagnosed in the first year of life. In contrast, non-heritable retinoblastoma tends to be diagnosed in the 1 to 2 year age range. Genetics is another risk factor, as the risk of developing retinoblastoma is higher in children with a parent who had heritable retinoblastoma.
Other potential risk factors have been proposed, such as older age of fathers, exposure of fathers to radiation, exposure to toxic chemicals during pregnancy, and diets low in fruits and vegetables during pregnancy.
Retinoblastoma classically presents with leukocoria, or white color of the pupil when light is shone in the eye (as opposed to the normal red reflex).
Retinoblastomacan also present with the following:
- Strabismus
- Poor visual acuity
- Conjunctival injection
- Proptosis
- Pseudohypopyon
- Secondary glaucoma
- Iris neovascularization
- Iris heterochromia
- Ocular pain
Retinoblastoma can also masquerade as endophthalmitis, uveitis, hemorrhage, or orbital cellulitis. If there is systemic involvement or spread, patients can present with non-specific constitutional symptoms such as headache, vomiting, unintentional weight loss.
Diagnostic criteria and tools
Screening is the first line of diagnosis. The American Academy of Pediatrics recommends screening for all neonates and infants before discharge from the nursery and routine health checkups. An abnormal red reflex (e.g., leukocoria) should prompt an urgent referral to a pediatric ophthalmologist.
Figure 1 illustrates leukocoria.


Figure 1: (Step2 Medbullets)
Genetic testing and counseling are recommended in families with a history of retinoblastoma. A dilated fundus exam is critical. An exam under anesthesia should be done in some cases to allow for an appropriate and comprehensive examination with scleral depression to confirm diagnosis and grade/stage.
On fundus exam, retinoblastoma classically appears as one or multiple nodular white/creamy elevated masses with increased vascularization. The endophytic retinoblastoma grows anteriorly into the vitreous, causing a vitreous haze. This anterior growth can reach the extent that it involves the anterior chamber causing inflammation and secondary glaucoma. The exophytic type demonstrates a posterior growth pattern, leading to subretinal disruption and exudative retinal detachments.
Ultrasound will demonstrate a hyperechoic mass with hyperreflective foci and posterior shadowing. This appearance is diagnostic for retinoblastoma in children. Ultrasound can also assess height, thickness, calcification and the presence of a retinal detachment. MRI imaging is preferred over CT scan imaging and can help assess for extraocular involvement including concurrent CNS involvement such as the presence of primitive neuroectodermal tumor in trilateral retinoblastoma.
To this end, lumbar puncture and bone marrow can also be examined to assess for metastases for which the prognosis is much more dismal.
Optical coherence tomography (OCT) provides another diagnostic tool to help localize retinoblastoma location and monitor for subclinical recurrences. Fluorescein angiography (FA) has value in the work up of retinoblastoma in its ability to help distinguish between Coats disease.
Although both feature tortuous vessels, microaneurysms, and nonperfusion areas, vessel abnormalities at multiple levels on FA is more characteristic of retinoblastoma as vessels overlying and intrinsic to the tumor are involved. Coats disease most commonly shows focal telangiectasias and light bulb aneurysms with subretinal space leakage in late phases.
Other alternative differential diagnoses to consider for retinoblastoma may include:
- Persistent fetal vasculature
- Ocular toxocariasis
- Retinopathy of prematurity
- Choroidal coloboma
- Vitreous hemorrhage
- Myelinated nerve fiber layer
- Astrocytic hamartoma

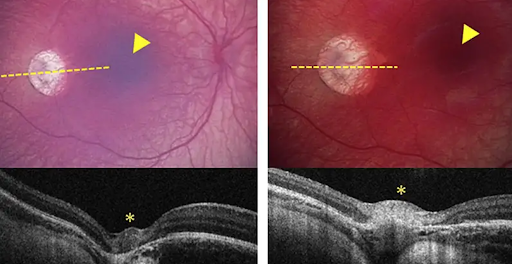
Figure 2: OCT of retinoblastoma (AAO)
Biopsies are a central part of diagnosing many cancers, but in the case of retinoblastoma this is more challenging as direct biopsy can cause relapse or spread of the disease to outside of the eye. One new development, biopsy of the aqueous humor, provides a promising and advantageous method of diagnosis compared to blood biopsies as they can localize tumor characteristics to a specific eye in the case of bilateral disease.
Aqueous biopsy provides a safe and effective way to work up retinoblastoma and provides a framework for developing more targeted therapies and providing superior prognostication. The tumor biomarker 6p gain, for example, has been found as an indicator of more aggressive disease.
The International Classification of Retinoblastoma (ICRB) classification breaks down retinoblastoma into five groups (A through E):
- Group A represents tumors less than 3 mm and away from the fovea and optic disc
- Group B tumors are greater than 3 mm located at the macular/peripapillary region or with subretinal fluid
- Group C tumors are those with focal vitreous or subretinal seeds within 3 mm of the tumor
- Group D are tumors with diffuse vitreous or subretinal seeds > 3 mm away from the tumor
- Group E are those tumors covering > 50% of the globe with or without neovascular glaucoma, hemorrhage or extension to the optic nerve or anterior chamber
Classification becomes important when providing counseling and planning treatment.
Novel screening tools for retinoblastoma
Arclight
Screening is critical, as a delay in diagnosis leads to increased morbidity and mortality. Several new and exciting tools have been developed to screen for retinoblastoma. The Arclight is a handheld device that can be used as an attachment on loupes, or an otoscope or ophthalmoscope and has been shown to have a 93% sensitivity in screening for media opacities. This tool can be utilized in low-resource settings and is powered by a solar panel.


Figure 3: Arclight (Community Eye Health Journal)
PEEK
The portable eye examination kit, or “PEEK”, can be used with a mobile phone to capture retina images without formal training and has shown promise in under-resourced settings, with a sensitivity of 90% in screening for media opacities.
iCam
Optovue has developed a portable fundus camera called the iCam that captures retinal photos that can be viewed on large displays such as television and computer screens, with a sensitivity of 98% in screening for media opacities. Although these devices can be utilized by minimally trained support staff for general patients, a trained ophthalmic nurse is needed in the case of children.
RetinaScope
The RetinaScope is a clip-on smartphone attachment that can be used for fundus imaging however requires a trained staff member to acquire photos. The RetinaScope has been studied as a screening tool for children for various pathologies including retinoblastoma.
Smartphone-based apps
MDEye Detector and CRADLE are two smartphone based applications that do not require a skilled staff member to capture a scan. The MDEye Detector has superior detection rates as compared to the CRADLE app, however the MDEye Detector requires interpretation by the user while the CRADLE app provides an automated response of “normal” or “white.”
Treatment of retinoblastoma
Retinoblastoma usually requires intervention to preserve life, the globe, and visual acuity. Spontaneous regression is rare. Side effects of treatment options and laterality of disease should be considered when deciding on treatment. While enucleation represents definitive treatment of intraocular retinoblastoma, there are many treatment options aimed at globe salvation, including chemotherapy, intra-arterial chemotherapy, radiation, and focal destructive therapy such as cryopexy, laser, hyperthermia, and plaque irradiation.
Older therapies, such as external beam radiation, have fallen out of favor due to the association with secondary malignancy.
In cases of advanced bilateral retinoblastoma, the severely affected eye is typically enucleated while the other is treated with a chemoreductive approach. Chemoreduction describes combining systemic chemotherapy with focal consolidative treatment such as thermal, cryo- or laser- therapy to shrink tumor size and salvage the globe. However, in some cases, unilateral disease may require enucleation if there is a threat of spread, especially in poor baseline visual acuity.
Intra-arterial chemotherapy
Localized chemotherapy allows the benefit of avoiding systemic side effects. One such localized approach is to deliver triple or tandem therapy within the ophthalmic artery. Side effects include occlusive choroidopathy and the risk of stroke.
Intravitreal chemotherapy
Intravitreal chemotherapy has shown promise in treating refractory vitreous seeds in patients already receiving systemic or intra-arterial chemotherapy. Before injection, freeze-thaw therapy to the injection site must be done to prevent the spread of retinoblastoma cells. Risks include those typically associated with intravitreal injections such as cataract, bleeding, retinal detachment and infection, with higher rates of each when delivering higher doses of chemotherapeutic agents.
Radiation
When retinoblastoma remains uncontrolled despite the above-targeted interventions alone or in combination, external beam and plaque radiotherapy are viable options. Risks with radiation include secondary malignancy, orbital hypoplasia, and radiation retinopathy.
Figure 4 depicts intraoperative plaque insertion for planned radiation therapy.

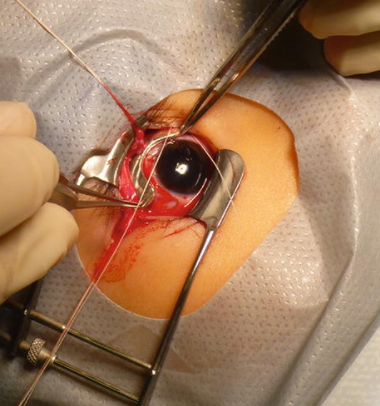
Figure 4: Murakami et al
Surgical treatment
In patients with group D or E disease the concern of extraocular and involvement and metastasis necessitates more aggressive intervention with primary enucleation. A secondary goal with enucleation in this setting is removing as much of the optic nerve as possible. It is also critical to send the specimen to pathology as there are several risk factors associated with extraocular spread such as scleral or choroidal invasion, post laminar invasion of the optic nerve and/or involvement of the anterior chamber. In these high risk settings the decision to perform adjuvant chemotherapy is recommended. Close followup is needed to assess for recurrence, spread and for optimizing aesthetics.
Medical management is beyond the scope of this paper; however, extraocular blastoma is addressed with neoadjuvant chemotherapy, stem cell rescue, surgical debulking, and post-operative chemotherapy and radiation as needed with low but steadily improving survival rates.
Trilateral retinoblastoma provides another clinical dilemma of choosing between chemotherapy versus radiation. Regardless of the treatment approach (eye sparing versus enucleation, systemic versus localized), frequent and consistent follow-up is needed to monitor for recurrence and resolution due to the high risk of developing a secondary malignancy.
While there have been significant advances in retinoblastoma screening, detection, and treatment, there remains a considerable disparity in outcomes for high-income versus mid to low-income nations. Screening represents a frontier through which these disparities and gaps can be mitigated, with new and easy-to-use screening tools as well as novel techniques to diagnose, such as anterior chamber taps providing promise moving forward.
In terms of management, globe salvage therapies provide an alternative to aggressive enucleation for group A through C retinoblastomas, with more advanced group retinoblastomas or those with extraocular spread and metastasis still posing clinical challenges with the need for more aggressive surgical and medical management.
References
- Children's Hospital Los Angeles. "Eye on research: A new way to detect and study retinoblastoma: Novel way to biopsy an aggressive childhood cancer." ScienceDaily. ScienceDaily, 4 November 2019. <www.sciencedaily.com/releases/2019/11/191104155710.htm>.
- Jesse L. Berry, Liya Xu, Ashley Polski, Rima Jubran, Peter Kuhn, Jonathan W. Kim, James Hicks. Aqueous Humor is Superior to Blood as a Liquid Biopsy for Retinoblastoma. Ophthalmology, 2019; DOI: 10.1016/j.ophtha.2019.10.026
- Hurwitz RL, Shields CL, Shields JA, et al. Chapter 27: Retinoblastoma. In: Pizzo PA, Poplack DG, eds. Principles and Practice of Pediatric Oncology. 7th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2016.
- Kaufman PL, Kim J, Berry JL. Retinoblastoma: Clinical presentation, evaluation, and diagnosis. UpToDate. Accessed at www.uptodate.com/contents/retinoblastoma-clinical-presentation-evaluation-and-diagnosis on September 18, 2018.
- National Cancer Institute. Retinoblastoma Treatment (PDQ®). 2018. Accessed at www.cancer.gov/types/retinoblastoma/hp/retinoblastoma-treatment-pdq on September 18, 2018.
- Rodriguez-Galindo C, Orbach DB, VanderVeen D. Retinoblastoma. Pediatr Clin North Am. 2015;62(1):201-223.
- Vempuluru, Vijitha S. MD; Kaliki, Swathi MD Screening for Retinoblastoma: A Systematic Review of Current Strategies, Asia-Pacific Journal of Ophthalmology: March-April 2021 - Volume 10 - Issue 2 - p 192-199 doi: 10.1097/APO.0000000000000378
- Murakami N., Suzuki S., Itami J. (2019) Ocular Plaque Brachytherapy for Uveal Melanoma and Retinoblastoma. In: Yoshioka Y., Itami J., Oguchi M., Nakano T. (eds) Brachytherapy. Springer, Singapore. https://doi.org/10.1007/978-981-13-0490-3_19
- Schefler AC, Kim RS. Recent advancements in the management of retinoblastoma and uveal melanoma. Fac Rev. 2021;10:51. Published 2021 May 28. doi:10.12703/r/10-51
