



Myopia, the most common refractive error, is characterized by axial elongation. It is estimated that by 2050 ~50% of the world's population will have myopia and 10% will have high myopia.1
High myopia is defined as refractive error ≥ -6.00D or axial length ≥ 26.5mm.2 When high levels of myopia are associated with sight-threatening ocular changes, it is described as pathologic myopia (PM), also known as myopic macular degeneration.
Pathophysiology of PM
PM results from excessive axial elongation, which causes biomechanical stretching and weakening of the sclera, choroid, retinal pigment epithelium (RPE), and retina, leading to progressive and often irreversible vision loss.3 It affects up to 3% of the world’s population.4
The weakening from axial elongation causes the retina to stretch, leading to scleral ectasia known as posterior staphyloma—a hallmark finding in PM. Posterior staphyloma is strongly associated with progressive axial elongation and correlates with increased risk of myopic maculopathy, choroidal neovascularization, and vision-threatening atrophic changes.5
Figure 1: Fundus image of a posterior staphyloma (PS) with borders showing pigment anomalies.


Figure 1: Posterior Staphyloma© Adèle Ehongo. Image used under CC BY-NC 3.0.
Risk factors for pathologic myopia
Risk factors for PM include:4
- Early onset of myopia
- Rapid axial elongation during childhood
- High myopic refractive error (typically > -6.00D)
- Positive family history
In addition, certain ethnicities have a higher predilection, especially those in Asian countries; females also have a higher prevalence.7 Axial length ≥ 24.5mm in children 8 to 11 years old is also considered an early risk factor for myopic progression,8 and progression over -0.50D / year is defined as significant myopic progression.6
Environmental factors such as excessive near work and limited outdoor activity are also linked to its development and progression.9
To learn more about identifying patients at high risk of myopia progression, check out the article Understanding Myopia Risk Factors!
Complications of untreated pathologic myopia
There can be several serious complications resulting from pathologic myopia, including:
- Myopic traction maculopathy (MTM)
- Myopic choroidal neovascularization (mCNV)
- Macular atrophy
- Maculoschisis
- Macular holes
- Retinal detachment
MTM affects 9 to 34% of eyes with high myopia (≥ -6.00D or axial length ≥ 26.5mm) and is caused by tangential tractional forces from the vitreous and posterior staphyloma pulling on the retina.6 It often starts with inner retinal schisis, then progresses to involve the outer retinal layers and can lead to macular detachment or full-thickness macular holes.
Figure 2 demonstrates a dissecting microscope image of a macular hole.

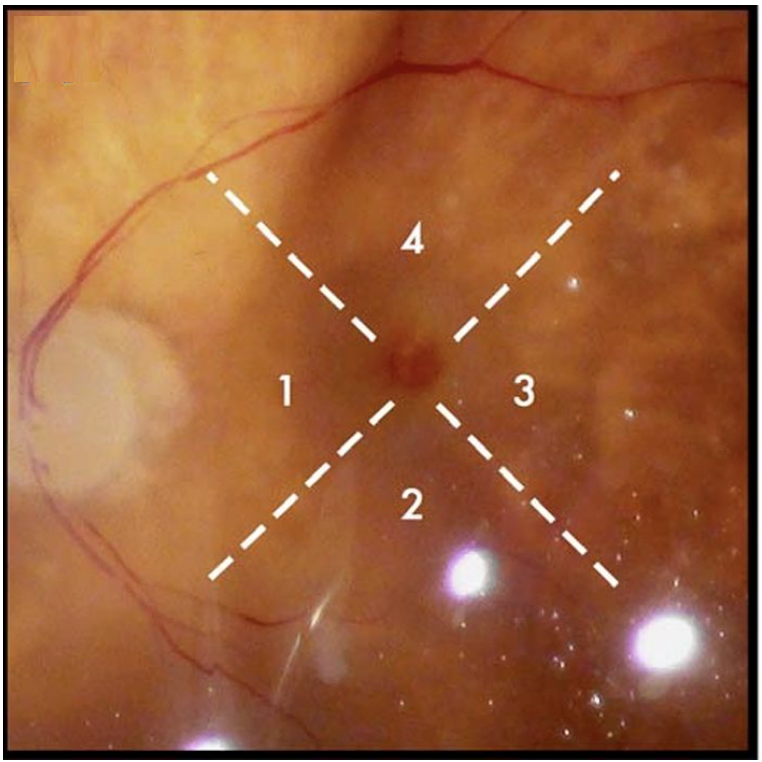
Figure 2: Courtesy of David Almeida, MD.
Of note, mCNV develops in about 10% of patients with pathologic myopia and is the second most common cause of CNV after age-related macular degeneration (AMD), as well as the most common cause in patients under 50.10
Macular atrophy is advanced degeneration of the RPE and choriocapillaris, often following mCNV, causing permanent vision loss.2 Maculoschisis is caused by the splitting of the inner retinal layers at the outer plexiform layer from perpendicular tractional forces, which can progress to macular holes and even retinal detachment if left untreated.6
Macular holes are full-thickness defects in the macula caused by chronic traction and often present alongside schisis or detachment in these eyes.6 Retinal detachment is another serious complication, as peripheral retinal thinning, lattice degeneration, and posterior staphyloma can increase the risk of detachment up to 10 times more than in non-myopic eyes.4
High myopia vs. pathologic myopia
It is important to distinguish between high myopia and pathologic myopia. High myopia is a quantitative diagnosis, defined by axial length and refractive error.
Figure 3: Fundus photographs of peripapillary atrophy and high myopia.

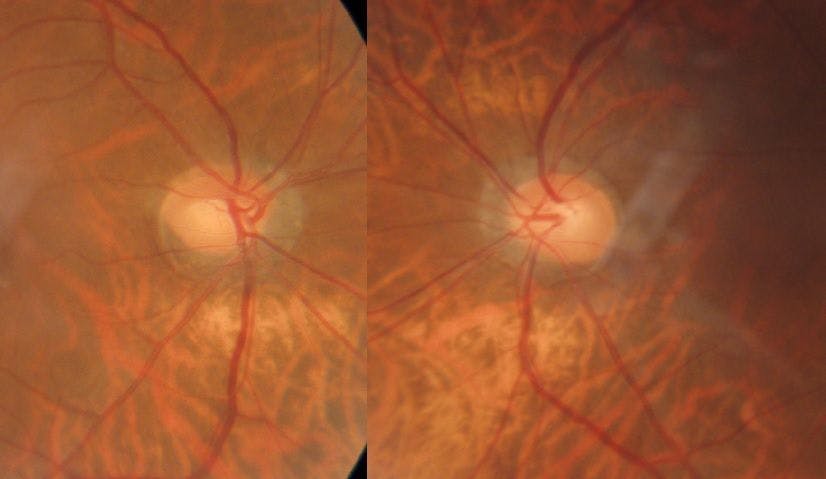
Figure 3: Courtesy of Kevin Cornwell, OD, FAAO.
Pathologic myopia, on the other hand, is both quantitative and qualitative—it is high myopia but with progressive structural changes, such as chorioretinal atrophy, lacquer cracks, or posterior staphyloma, that can lead to vision-threatening complications.
Pathologic myopia was first defined by Duke-Elder in the 1970s as progressive myopia with degenerative changes involving the sclera, choroid, retina, and vitreous. Since then, advances in imaging have improved the ability to detect complications, such as posterior staphyloma, mCNV, maculoschisis, and macular atrophy.
A deeper understanding of the underlying biomechanical mechanisms has also shaped current perspectives. This culminated in the 2015 META-PM Study, which introduced a standardized classification system for myopic maculopathy.11
Classification of pathologic myopia
The 2015 study by Ohno-Matsui and colleagues was conducted to establish a standardized classification and grading system for myopic maculopathy.
The system includes five categories based on fundus appearance:11
- Category 0: No maculopathy
- Category 1: Tessellated fundus
- Category 2: Diffuse atrophy
- Category 3: Patchy atrophy
- Category 4: Macular atrophy
In addition, “plus” lesions—such as lacquer cracks, myopic CNV, and Fuchs spots—were identified as significant vision-threatening features. According to this system, a diagnosis of pathologic myopia is made when Category 2 or higher maculopathy and/or any plus lesion is present. This classification provides a consistent framework for diagnosing, staging, and monitoring progression in eyes with high myopia.11
Table 1: Myopic maculopathy classification system from the META-PM study.11
| Category | Findings | Definitions |
|---|---|---|
| 0 | No myopic macular lesions | |
| 1 | Tessellated fundus only | RPE appears thinned with reduced pigment; choroidal vessels are more visible due to choroidal thinning |
| 2 | Diffuse choroidal atrophy | Pale, yellowish-white discoloration around the optic disc and macula due to widespread atrophy of the choroid |
| 3 | Patchy chorioretinal atrophy | Localized, sharply bordered grey-white lesions indicating focal degeneration of the retina and choroid |
| 4 | Macular atrophy | Central retinal thinning and cell loss at the macula, associated with significant vision loss |
| Plus lesions | Lacquer cracks, CNV, Fuchs spots | Additional findings that can develop at any stage; lacquer cracks are breaks in Bruch’s membrane, CNV represents abnormal vessel growth, and Fuchs spots are pigmented scars from past CNV |
Table 1: Adapted from Ohno-Matsui et al.
Clinical exam guidelines for PM
Assessing for pathologic myopia requires a thorough medical history and retinal exam accompanied by imaging.
Medical history
A focused and thorough history is essential when evaluating patients with pathologic myopia. Key points to ask in medical history include the age of myopia onset and rate of progression. Any family history of high myopia, retinal detachment, macular holes, or traction-related pathology should be documented, as well as prior ocular procedures such as laser photocoagulation or intravitreal anti-VEGF injections.
In patients with a history of refractive surgery, it is important to ask about their pre-operative prescription. Additionally, patients should also be asked about visual symptoms—blurred vision or metamorphopsia may suggest macular involvement, while flashes, floaters, or a curtain-like shadow may indicate vitreoretinal traction, retinal tears, or detachment.12
Retinal exam
A comprehensive dilated fundus examination is critical and should include slit lamp biomicroscopy and binocular indirect ophthalmoscopy with scleral indentation.
Several clinical signs may point to pathologic myopia. These include a tessellated fundus appearance from choroidal thinning, obliquely inserted optic nerves with peripapillary atrophy, and the presence of posterior staphyloma—a hallmark finding.5
Additional findings may include lacquer cracks, Fuchs spots, areas of chorioretinal atrophy, and signs of vitreomacular traction or maculoschisis. In the periphery, retinal thinning, lattice degeneration, and retinal holes or tears may also be observed.
Retinal imaging
Advancements in ocular imaging have improved the early detection, documentation, and monitoring of complications in pathologic myopia, including:
- Ultra-widefield imaging systems such as Optos and Eidon provide detailed views of peripheral retinal degeneration and breaks.
- Measuring axial length is crucial; devices like the Optopol Revo and Topcon Aladdin offer axial length measurements alongside other metrics.13
- A-scan ultrasonography remains another method to measure axial length. Spectral-domain OCT allows high-resolution visualization of vitreomacular interface abnormalities, schisis cavities, macular holes, and myopic CNV.
- Enhanced depth imaging (EDI-OCT), such as with Spectralis, enables assessment of choroidal thinning.13
- Fundus autofluorescence can detect areas of RPE atrophy.
- Posterior staphyloma can be evaluated with B-scan ultrasonography, which also provides axial length data.5
- OCT angiography allows noninvasive visualization of the choriocapillaris and neovascular membranes without dye to assess for CNV.
Figure 4: OCT angiography scan of a myopic patient.


Figure 4: Courtesy of Leanne Liddicoat, OD, FCOVD.
Treatment and management of PM
Treatment and management of pathologic myopia requires a comprehensive and multimodal approach, focusing on both preventing progression and addressing complications.
Lifestyle modifications
Lifestyle changes should be encouraged in all patients, especially pediatric patients. Sustained near work has been shown to contribute to myopia progression—patients should be advised to take frequent breaks and work under proper lighting conditions.
Increased outdoor activity is a proven protective factor; even 1 to 2 hours a day can reduce the risk of myopia onset and slow axial elongation by enhancing dopamine release and modulating retinal signaling.9
Refractive treatment
Parents should be counseled on the importance of early intervention with myopia control, especially in children with a strong family history of myopia. Myopia control options include Stellest or MiyoSmart spectacle lenses (currently not available in the US but are in Canada) and MiSight daily disposable contact lenses.
Orthokeratology lenses or low dose atropine are also effective options. All glasses should be made with polycarbonate lenses to protect against ocular trauma, which is a greater concern in high myopes due to the risk of retinal complications.14
Contact lenses often offer better visual quality than spectacles in high myopia due to reduced minification and improved optics. Biofinity XR, a silicone hydrogel option, is available in extended parameters up to –20.00D and provides excellent oxygen permeability for daily wear.
While refractive surgery such as LASIK or PRK can be considered in stable high myopes (typically up to –12.00D), it is generally avoided in pathologic myopia due to the increased risk of ectasia, progressive degenerative changes, and retinal detachment.15
Implantable collamer lenses (ICLs) may be a safer alternative in select cases and are especially useful in patients with refractive errors beyond LASIK or PRK limits who do not have advanced signs of PM.
Anti-VEGF treatment
For patients with mCNV, the standard of care is anti-VEGF injections. Both ranibizumab and aflibercept have been shown to improve or stabilize vision by reducing CNV activity.
The RADIANCE trial demonstrated that ranibizumab led to rapid visual improvement, while the MYRROR study showed similar benefits with aflibercept, particularly in Asian populations.16,17
Pars plana vitrectomy
Pars plana vitrectomy (PPV) is indicated in cases of myopic traction maculopathy, especially when there is macular schisis, detachment, or full-thickness macular hole. The goal of PPV is to relieve both tangential and perpendicular traction, reattach the retina, and restore macular contour.
In some patients with early tractional changes, prophylactic vitrectomy may be considered to prevent progression to more severe complications such as macular detachment.18
Differential diagnoses for pathologic myopia
When evaluating pathologic myopia, it is important to differentiate it from other retinal and choroidal conditions that may appear similar to avoid misdiagnosis. AMD, central serous retinopathy (CSR), and inherited retinal dystrophies can share overlapping features such as chorioretinal atrophy, pigmentary changes, or subretinal fluid.19
AMD can present with macular atrophy and CNV, but patients are typically older and show other signs such as drusen. CSR may resemble myopic schisis or CNV but is characterized by serous retinal detachment and a thickened choroid, unlike the thin choroid seen in pathologic myopia.19
Diabetic macular edema and Irvine-Gass syndrome may cause macular thickening but are associated with systemic diabetes or recent intraocular surgery and lack features such as posterior staphyloma or lacquer cracks.
Other causes of CNV—including presumed ocular histoplasmosis, Best disease, polypoidal choroidal vasculopathy, choroidal rupture, and angioid streaks should also be considered in the differential diagnoses.
Patient education on pathologic myopia
Educating patients is also fundamental in managing pathologic myopia—not only to inform them of their condition but also to monitor for early symptoms and prevent further complications.
Patients should have annual dilated fundus exams with retinal imaging and shorter intervals are recommended for those with high-risk features such as posterior staphyloma, lacquer cracks, or prior CNV.20
While each follow-up interval should be individualized for each case, the following intervals can serve as general clinical recommendations for high-risk features of myopic maculopathy:
- Posterior staphyloma: 6 to 12 months
- Lacquer cracks: 6 months
- Inactive myopic CNV: 3 to 6 months
- Active myopic CNV: Co-manage with retinal specialist, every 4 to 6 weeks typically
- Myopic traction: 3 to 6 months, depending on foveal involvement
Because of the family history component, first-degree relatives should be encouraged to be evaluated. Children of highly myopic parents should be monitored from an early age and educated on the risk of progression to pathologic myopia—this is also an ideal opportunity to introduce myopia control.
Additional PM pearls for patients
Myopia control should be an early goal in order to prevent PM complications later in life. Public health education should stress the importance of outdoor time—ideally 90 to 120 minutes daily—and reducing prolonged near work, especially screen time.21
Proper lighting during near tasks should also be emphasized. These simple interventions carry long-term therapeutic benefits beyond the eyes and are especially important given the rising global burden of myopia.
Patients should also be educated on symptoms like new-onset floaters, flashes of light (which may signal retinal breaks), or central distortion (which can be indicative of macular involvement). Those with signs of myopic maculopathy should be given home Amsler grids to monitor for central scotomas or metamorphopsia and advised to return promptly if changes are noted.
Showing patients their imaging, such as fundus photos, OCT scans, or axial length measurements, is also a helpful way to educate and improve understanding.
Clinical trials and research on pathologic myopia
Following the rise in pathologic myopia worldwide, recent studies have shifted focus toward novel treatment strategies and preventative approaches.
The POYANG trial is currently recruiting and is investigating faricimab, a novel bispecific antibody that targets both VEGF-A and angiopoietin-2 pathways for the treatment of myopic CNV.22 Its dual mechanism of action may offer superior vascular stability compared to traditional anti-VEGF agents like ranibizumab or aflibercept.
Scleral cross-linking, modeled after corneal cross-linking in keratoconus, is another area of interest. Agents such as genipin have demonstrated biomechanical strengthening of the posterior sclera in animal models and have shown potential to slow axial elongation.23
Posterior segment–targeted therapies that aim to modulate choroidal thickness are also being explored as a way to modulate axial growth. Structural reinforcement approaches, such as posterior scleral reinforcement, involve mechanically supporting the posterior pole and have shown promise in stabilizing progressive axial elongation in clinical studies.
Surgical interventions like macular buckling for perpendicular tractional forces and prophylactic PPV for both tangential and perpendicular tractional forces are also being studied for their role in managing MTM.10 These procedures may help prevent progression to macular detachment or full-thickness macular holes.
As research evolves, combining biomechanical, pharmacologic, and surgical treatments may offer a more effective and individualized approach to managing pathologic myopia.
Conclusion
As the global prevalence of myopia continues to rise, pathologic myopia represents a growing threat to vision. Early identification, patient education, and consistent monitoring are essential.
Advances in imaging, treatment modalities, and myopia control strategies offer hope in slowing progression and preserving vision. A multidisciplinary, preventative approach—rooted in early intervention and informed patient care—will be key in addressing the pathologic myopia burden.
