



Even a brief look at the statistics on myopia prevalence proves why diagnosing this disease, accurately gauging its rate of progression, and then managing it accordingly is so incredibly important.
Currently, the rate of myopia in North America is 40 to 45%, while in Asian countries abroad, it is a staggering 80 to 95%. Worldwide the prevalence is 22%, but on the rise—it is estimated this number will double to approximately 45 to 50% by 2050.1-3
This means there will be five billion people with myopia across the globe, with one billion of those suffering from pathologic myopia.
What is pathologic myopia?
We define pathogenic—or degenerative—myopia as myopia structural changes to the eye due to elongation, typically occurring in those having an axial length >26mm and a refractive error >6 diopters (D), but which can occur with any degree of myopia.4
With high myopia, as opposed to low or non-myopia, the odds ratio for acquiring a number of these pathologic changes increases, as is represented in the table below. Similarly, with escalating myopia, we're naturally going to see corresponding numbers in this pathology, which makes monitoring and early management paramount.
Table 1 outlines the odds ratio increase associated with myopic refractive error.
| Condition | Refractive Error (D) | Odds Ratio |
|---|---|---|
| Cataract | -3.00 to -6.00D, -6.00 to -10.00D, >-10.00D | 1.56, 2.55, 4.55 |
| Retinal detachment & retinoschisis | -3.00 to -6.00D, -6.00 to -10.00D, >-10.00D | 3.29/3.15, 5.37/8.74, 40.56/12.62 |
| Glaucoma | -0.50 to -3.00D, >-3.00D | 1.59, 2.92 |
| Myopic macular degeneration | -3.00 to -6.00D, -6.00 to -10.00D, >-10.00D | 13.57, 72.74, 845.08 |
| Myopic choroidal neovascularization (CNV) | -3.00 to -6.00D, -6.00 to -10.00D, >-10.00D | 3.14, 17.0, 70.60 |
| Choroidal atrophy (and neovascularization) | -3.00 to -6.00D, -6.00 to -10.00D, >-10.00D | 3.48, 11.66, 74.08 |
Table 1: Data from Leveziel et al. and Haarman et al.
Monitoring myopia and calculating risk
Three questions I ask in my day-to-day myopia assessments are:
- What is the patient’s current myopia stage?
- What is their risk for more severe progression in the future?
- What types of treatments are available that could potentially slow this progression?
Current myopia stage
When seeing a patient, we are going to assess the risk factors for the development of myopia, test to determine axial length, and look at the likely rate of progression based on these findings.
Four primary factors come into play when calculating the risk for myopic progression:
- Age of onset: Younger age of onset is its own risk factor, independent of sex, ethnicity, school, reading time, and myopic parents.7
- Genetics: A patient with two myopic parents has a three to five times greater risk.7-11
- Environment: Outdoor time, near work, electronics, and light levels all play a role.7,11,12
- Ethnicity: Asians have a greater risk of myopia and progress more than individuals of European or African descent.2,13
Once a thorough history has been taken and risk calculated, it is time for testing. Knowing the axial length and refractive norms is key to setting baseline expectations.
Table 2 features the norms for refractive error and axial length according to current data on pediatric patients.14,15
| Age (years of age=yo) | Axial Length (mm) | Refractive Error (D) |
|---|---|---|
| Infants (0 to 3 years) | 19 to 21mm | +2.00D |
| 3 to 5 yo | 21 to 22mm | Emmetropization+1 at 5 yo |
| 6 yo | 22 to 22.75mm | |
| 6 to 16 yo | Slight myopic shift |
Table 2: Data from Mayer et al. and Bach et al.
Obviously, having both axial length and refractive error measurement gives you more data to evaluate the risk level to determine appropriate treatment. However, if you only choose to use one means of measurement, axial testing is preferred, as a direct measure of eye length is more objective and direct. With axial length measurements, keep in mind machines typically measure from the cornea to the front of the choroid, not outside the scleral shell.
Pearl: Axial length is the preferred measurement for tracking myopia progression. However, if only measuring refraction, make certain it is a cycloplegic refraction to ensure you have the most objective data possible to follow from year to year.
Measuring axial length
When measuring axial length, there are two types of instrumentation: ultrasound and interferometry. Both of these offer repeatable and precise results, but each has pros and cons.
Ultrasound devices are lower cost and can be portable; however, they have a longer acquisition time and make direct contact with the eye. Interferometer comes in at a higher cost but offers quicker acquisition times and measures length without any direct contact with the eye. For those with myopia as a primary focus, there are a range of new technologies available.
Listed below are the capabilities of some of the current machines on the market:
- Myopia Master: Refraction, pupil diameter, axial length, corneal curvatures, risk calculator, and patient report
- Pentacam AXL: Standard Pentacam features (e.g., corneal topography, keratoconus classification), axial length, intraocular lens (IOL) calculator
- Tomey OA 2000: Axial length, pupillometry, keratometer, biometer (axial length), pachymeter
- IOL Master 700: Axial length, keratometry, refraction calculations
Pearl: When measuring central axial length, occlude the eye not being tested and take at least five measurements to average for the final value.
Risk for progression
Calculating the risk for progression is critical in determining how to manage the patient best. Once you have your axial length and refractive error, there are several available tools that show the estimated progression under different treatment scenarios.
The Singapore and the American Optometric Associations, along with the American Academy of Optometry and industry partner Johnson & Johnson, released the guide Managing Myopia: A Clinical Response to a Growing Epidemic, which contains this helpful table of mean progression.
Table 3 compares the mean progression for myopic axial length in Asian and non-Asian pediatric patients by axial length and refractive error.
| Age | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|
| Axial length (mm) | Asian | 0.52 | 0.46 | 0.41 | 0.36 | 0.32 | 0.28 |
| Non-Asian | 0.35 | 0.31 | 0.28 | 0.25 | 0.22 | 0.20 | |
| Refractive error (D) | Asian | -1.12 | -0.94 | -0.78 | -0.66 | -0.56 | -0.50 |
| Non-Asian | -0.98 | -0.82 | -0.69 | -0.56 | -0.45 | -0.35 |
Table 3: Courtesy of the Singapore Optometric Association, American Optometric Association, American Academy of Optometry, and Johnson & Johnson.
The Brian Holden Vision Institute's Global Myopia Center Calculator is another invaluable tool for assessing risk and formulating treatment. It allows you to enter the patient’s ethnicity, age, and refractive error to calculate what the rate of progression will be based on no treatment or the various myopia management options. Both of these resources also serve as an excellent tool for educating parents.
Measuring myopia progression on follow-up
At the follow-up visit, recommended every 6 months but variable depending on the needs and status of the child, reevaluate the patient using the same testing method/s as before for consistency and accuracy.16
Compare the new axial length and refractive error to the original to determine if the rate of progression has sufficiently slowed. If it has not, alter the treatment based on the rapidity of progression, risk factors, and overall level of concern from both OD and family.16
Case report #1
Case 1 is an Asian female with two myopic parents who first presented at age 7 with a spherical equivalent myopic refraction of -2.25D OU with axial lengths of 23.37mm OD and 23.38mm OS. She started myopia control treatment immediately with distance center concentric circle multifocal soft contact lenses. The final prescribed lenses were -3.00D sphere OU powered with a +2.50 add.
After 1 year of treatment, refraction was -3.75D OD and -4.00D OS with axial lengths of 23.80mm and 23.82mm, respectively; per year axial elongation progression rate was calculated as 0.52mm/year OU (natural progression for this age/race is about 0.46mm/year).
Due to the high risk for future progression, treatment was switched to custom soft multifocal lenses with a -4.00D center distance power and a +4.00D peripheral add, OU. Then, 1 year later, the per year progression rates were calculated as 0.56D and 0.19D refractive progression and 0.26mm and 0.23mm axial elongation OD and OS, respectively.
This represented a slowing of progression by about 50% compared to the previous year. Due to continued parent concern in this young patient, atropine drops (0.05%) were added QPM OU, and the soft multifocal contact lenses were continued at the same power.
After initiating atropine drops, progression slowed to a rate of 0.30D/0.16mm OD and 0.10D/0.13mm OS. The myopia control methods were considered effective. The patient is currently 15 years old, -4.75D OU, with an axial length of 24.94mm OD and 24.84mm OS; the progression is considered under control.
This case provides a good example of using custom soft lenses with higher than customary add powers, as well as dual treatments, to achieve myopia control success.
Case report #2
Case 2 is an Asian male with two myopic parents who first presented at age 7 with a spherical equivalent myopic refraction of -1.75D OD and -1.50D OS with axial lengths of 24.03mm OD and 24.13mm OS.
He started myopia control treatment immediately with rigid orthokeratology (ortho-k) lenses with the following parameters:
- OD: 8.4 base curve (BC), 0.525 return zone depth (RZD), -36 landing zone angle (LZA), 10.5mm diameter
- OS: 8.4 BC, 0.525 RZD, -35 LZA, 10.5mm diameter
At the next annual exam, axial lengths were 24.72mm OD and 24.79mm OS, respectively. The per year axial elongation progression rate was calculated as 0.52mm OD and 0.49mm OS per year (the natural progression for this age/race is about 0.46mm per year).
At this visit, it was observed that there was decentration of the orthokeratology lens OD and a central island, indicating inadequate lens depth OS.
As a result, a washout was done, and new lenses with the following parameters were fitted (Figure 1):
- OD: 8.7 BC, 0.525/0.575 toric RZD, -33 LZA, 10.5mm diameter
- OS: 8.8 BC, 0.525/0.575 toric RZD, -33 LZA, 10.5mm diameter
Subsequently, 3 years after being re-fitted with these lenses, the axial length was 25.33mm OD and 25.54mm OS, and the calculated per-year progression rate was 0.09mm OD and 0.14mm OS in the patient, who was now 11 years old.
This case provides a good example of using dual-axis orthokeratology lenses to improve the fit of ortho-K lenses, which then resulted in a better myopia control effect for this patient.
Figure 1 features the topographical difference map after 6 months in the redesigned dual-axis lenses. Both eyes look well-centered, with good treatment zones and peripheral defocusing zones.

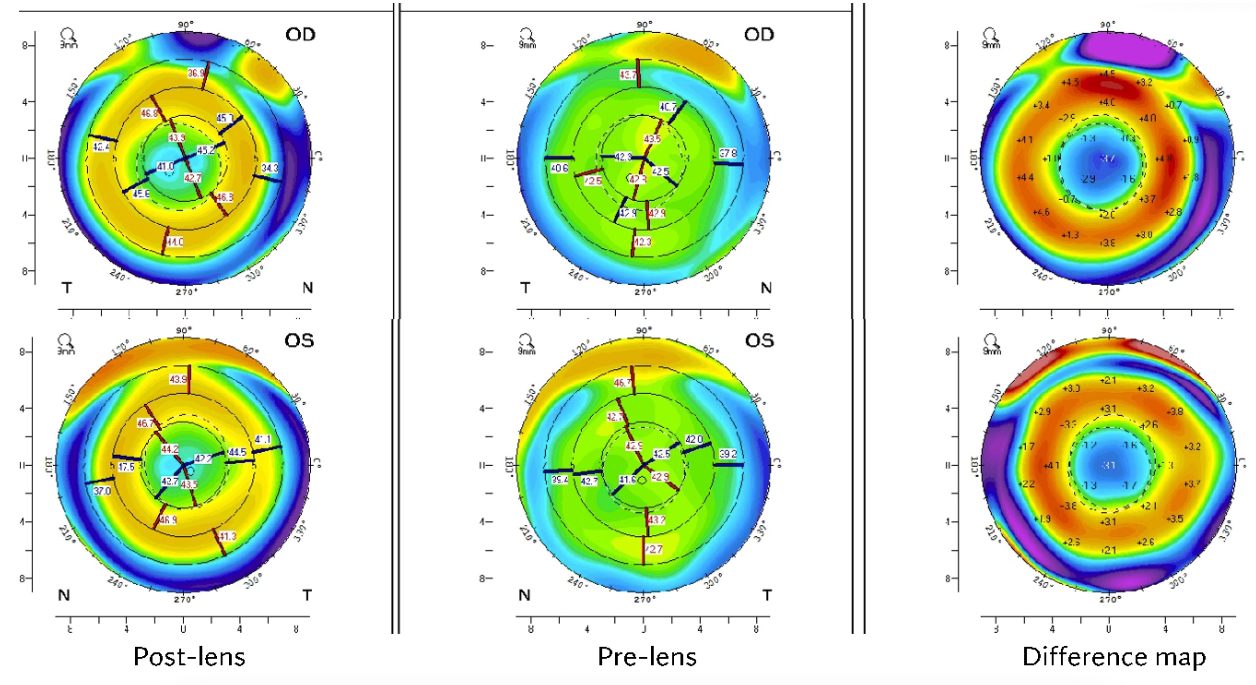
Figure 1: Courtesy of Maria Walker, OD, PhD, FAAO, FSLS.
Key takeaways
With innovations in testing and treatment, this is an exciting time to manage myopia. Further, as the numbers show, myopia management will continue to become a larger and larger part of most practices.
So, in closing, I would like to leave you with a few pearls.
Top pearls for assessing myopia progression
- If you are only using one measurement, opt for axial length: take the average of a minimum of five measurements.
- If you choose to measure refractive error, utilize cycloplegic wet refraction.
- Remember, refractive data cannot be directly translated to axial length.
Bonus treatment pearls
- In terms of atropine, a 0.05% concentration at bedtime is best.
- To more effectively slow progression, use higher add power in soft contact lenses.
- Be flexible and willing to change up or add treatments to achieve optimal results.
