


WHAT YOU'LL LEARN
Understand the clinical, economic, and social burden of primary angle closure
Learn the main options for treatment of primary angle closure
Practice techniques for taking patient history and documenting results
Learn gonioscopy essentials
Introduction
Introduction
One of the most common types of patients we see in our offices on a daily basis is the patient with narrow angles. This patient typically falls somewhere on the spectrum of angle closure—they are either on one end of the spectrum as a primary angle closure suspect (PACS), or further along and they have definitive primary angle closure (PAC), or even further along, and have developed primary angle closure glaucoma (PACG). And, hopefully for that patient, the first time you see them isn’t at the farthest end of the spectrum, in acute angle closure crisis (AACC).
A typical patient that we see in our office is a 54-year-old male with high blood pressure who presents for an initial eye exam with the complaint of mild blurry vision at near. Most of his exam is normal, he’s 20/20 with correction at near, his refraction is hyperopic +2.50 OD//+3.00 OS, he has intraocular pressure (IOP) in the high teens, say 18//19 mmHg, and early stage nuclear sclerotic cataracts. On further examination you perform gonioscopy and find an angle with only bare trabecular meshwork seen (Figure 1), and upon compression gonioscopy, no further angle structures are seen. You perform a non-dilated exam of the optic nerves and see a sharp healthy appearing optic nerve. Ultimately, your impression is that this patient has anatomically narrow angles.

Figure 1: Gonioscopy showing bare trabecular meshwork.
The next step is the challenge: what do you do next? Would you monitor this patient at every few month intervals? Would you start them on a topical antihypertensive eyedrop? Would you refer for laser peripheral iridotomy (LPI)? Would you refer for lens extraction?
Now what if the parameters of the case changed, and the patient was of Asian descent? Or female? Or younger—say, 35 years old? What if the patient had retinal pathology like diabetic retinopathy, or a history of a retinal detachment? What if they have a family history of angle closure glaucoma? Would any of these parameters change your plan?
The Big Picture: Disease Effects and Staging
Let’s step back for a minute and learn why it’s important to understand how to diagnose and manage patients on the angle closure spectrum. I like to think of ocular conditions in terms of the condition’s clinical, economic, and social burden to the patient.
In terms of clinical burden: we know that the prevalence of glaucoma on a whole is ever-increasing. In 2014 the global prevalence was reported to be ~3.5% of the global population.2,3 The total number of patients diagnosed with glaucoma, both open and closed angle glaucoma, in 2010 was 60.5 million people, increasing to 79.6 million in 2020, and estimated to be 111.8 million total patients with open and closed angle glaucoma worldwide.2,3 When comparing open angle and closed angle glaucoma, closed angle glaucoma comprises approximately ¼ of the total population of glaucoma worldwide both in 2010 and now in 2020 (Figure 2).2 However, both subgroups have an equal number of patients who go blind, lending to the significant clinical burden of the percentage of the total PACG patients who go blind (Figure 2).2

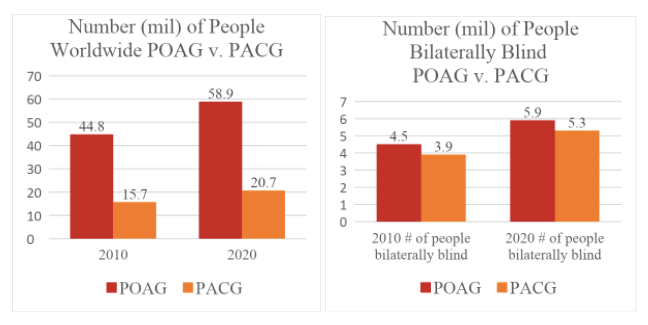
Figure 2: LEFT – total global population of primary open angle glaucoma (POAG) and primary angle closure glaucoma (PACG); RIGHT – number of patients bilaterally blind with POAG and PACG2
Our priority in caring for our patients is the burden that they experience. Typically, the patient burden is three-fold: the decompensation of the quality of life, formal costs such as insurance costs, and informal costs such as homecare aides or visiting nursing services. And all of these affect our efforts to manage their disease.
One study reviewing over 77,000 patient from 1996-2002 reported that even when controlling for other variables like comorbidities and demographics, blindness was found to use an excess of $2000.00, and 4 times the amount of extra days of informal care when compared to visually impaired patients.4 Now if you multiply that over a 10-year span (considering PACG spectrum patients have a chronic condition), this cost can come out to about $20,000$ and 40 times the amount of informal care when compared to a visually impaired patient. They concluded that blindness is the primary driving force in informal care needs for the patient. The goal therefore on a daily basis in clinic is taking this information as a basis of need for appropriate diagnosis and management as to prevent the progression to blindness the best we can.
Once we understand the burden of the disease, screening and diagnosing the condition is the next step. When screening for the disease there are some higher alert groups to look out for when assessing risk factors for the disease. Patient who are at risk for being on the primary angle closure spectrum include those who are: older in age, Asian/Inuit descent (87% of ACG), female (70% of ACG), and hyperopic patients.2,3 And with the increasing aging and diversifying population (especially in our urban centers), we will likely be seeing more patients on the angle closure spectrum in our offices.
Staging
You should also know the definition for the different stages along the spectrum of primary angle closure. The American Academy of Ophthalmology publishes their Preferred Practice Patterns for different ocular conditions every few years. Here they have established a staging guideline for Primary Angle Closure patients (Figure 3).5

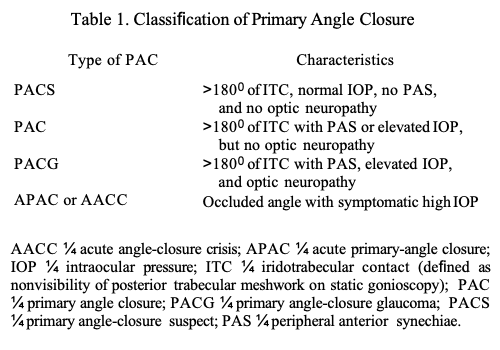
Figure 3: Preferred Practice Patterns of Primary Angle Closure spectrum patients; PACS: primary angle closure suspect, PAC: primary angle closure, PACG: primary angel closure glaucoma, APAC: acute primary angle closure, AACC: acute angle closure crisis, ITC: iridotrabecular contact, PAS: peripheral anterior synechiae.
All patients on the spectrum of angle closure have at least 180° degrees of iridotrabecular contact (ITC). Starting at the lower end of the spectrum being a primary angle closure suspect (PACS) is defined as having at least 180° ITC, but normal IOP, no peripheral anterior synechiae (PAS), and no optic neuropathy (ON). The patient is defined as having primary angle closure (PAC), when the IOP advances and is elevated, or the patient starts to develop PAS, but still has no ON. The patient then becomes a primary angle closure glaucoma (PACG) patient when they have the previous findings but also ON. The patient is in true acute angle closure crisis (AACC) when the high IOP is symptomatic and their angle is completely occluded. Having a consistent way of defining patients along this spectrum helps for universal and standardized diagnosis globally.
Diagnosing Primary Angle Closure
History and Exam
Patient History and Exam
Once you have identified your risk factors in an individual patient, taking a relevant history of present illness and comprehensive exam should be obtained. As we all know patients can range, symptom-wise, anywhere from being asymptomatic to having blurry vision, pain, halos, tearing, and/or intermittent redness. Family history can also be contributory. A comprehensive exam should include refraction, looking for hyperopia. Assessing the patient’s Von Herick’s angle, using a narrow slit beam shone 60° at the limbus can give a gross idea angle narrowing as a possibility (Figure 4).6

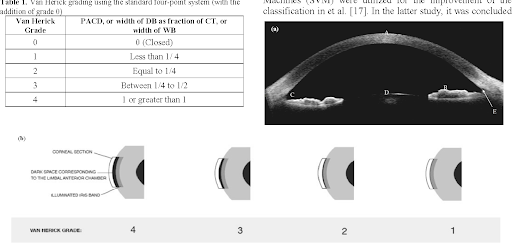
Figure 4: With two parallel light beams shone at a 60° at the limbus with the anterior beam being the corneal section and posterior beam hitting the anterior aspect of the iris. Between these beams is an optically black space. This space when measured in comparison to the width of the corneal section can be graded (Von Herick’s grading). If this band is approximately < ½ section of the corneal band thickness the angle should be further inspected.
Additionally, you should examine the patient’s lens status: whether the patient is phakic, pseudophakic, or aphakic, and how advanced their cataract is, if they have one. An optic nerve exam or retinal exam can potentially be performed non-dilated if you have concern of angle closure presence.
Gonioscopy
Most important in examining a patient with possible angle closure risk is gonioscopy.
Gonioscopy is currently the gold standard, as it is the quickest and most cost-effective screening tool we have for angle diagnoses. In 1907 Dr. Trantas (yes, of Trantas dots) was the first to examine the angle using his finger as a scleral depressor at the limbus while using a direct ophthalmoscope to view the angle. He did this to bypass total internal reflection. The anterior chamber configuration produces total internal reflection of light rays at the tear-air interface, thus disabling us from viewing a patient’s anterior angle with the naked eye.7

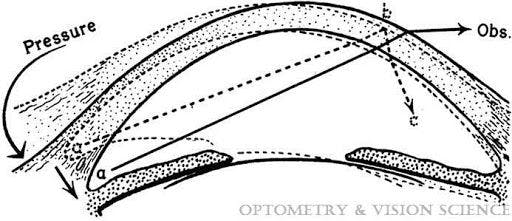
Figure 5: Total internal reflection of the anterior chamber angle.
Direct gonioscopy
There are different types of gonioscopy. One type of gonioscopy is direct gonioscopy, where the angle is viewed directly at the mirror you are viewing. Examples of direct gonioscopy lenses include a Koeppe lens, which is used most commonly used in exams under anesthesia, the Swans-Jacobs lens (Figure 6), is most commonly used to perform angle-based surgeries, and a few others, such as the Barkan, Richards, and Wurst lens.

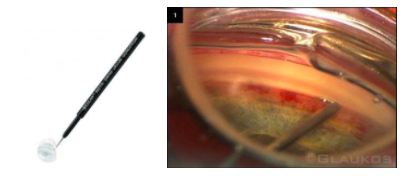
Figure 6: Swans-Jacob’s direct gonioscopy lens; anterior chamber angle viewed through a Swan Jacob’s lens of an iStent device.
The advantages of using direct gonioscopy include providing a larger wide-angle view of the anterior chamber angle, simultaneously viewing of both eyes as when using Koeppe lenses for exams under anesthesia (for example with an infant or noncooperative patient), and for use with angle-based surgery. Some disadvantages include the bulkiness of these lenses requiring an external illuminating source and microscope as well as requiring a coupling agent.
Indirect gonioscopy
Indirect gonioscopy, where the angle is indirectly viewed opposite the mirror in view, is likely more familiar, and the form that is used most often in-office. The different types of lenses include Goldmann, Possner (Figure 7), Zeiss, and Sussman. I personally use the Possner as it feels less bulky, and is easier to manipulate at the slit lamp in my hands.


Figure 7: Possner indirect gonioscopy lens.
Some advantages of indirect gonioscopy include its ability to eliminate internal reflection, as well as eliminate coupling agents (except for the Goldmann lens), and it is easier to incorporate into your slit lamp exam. You can also perform indentation or compression gonioscopy with these lenses as the posterior diameter of these lenses is smaller than the patient’s corneal diameter. Posterior pressure can be used to force open a narrow non-synechiae angle. This can help you distinguish iridocorneal apposition from synechial closure (Figure 8).8 However, if too much pressure is applied Descemet folds can appear, signifying false appreciation of angle structures.

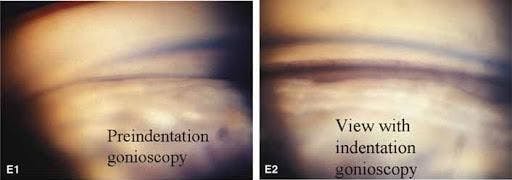
Figure 8: Gonioscopy of an anterior chamber angle preindentation gonioscopy (left) where minimal structures are seen, with indentation gonioscopy (right) where structures down to the ciliary body band are visualized.
Some disadvantages of indirect gonioscopy include not being able to view intraoperatively for angle-based surgery and, most importantly, requiring patient cooperation (which isn’t always the easiest to achieve). As mentioned before, gonioscopy is still the quickest and most cost-effective screening tool for angle diagnoses, and therefore is a very important skill to strengthen.
Gonioscopy grading and essentials
Gonioscopy Grading
There are three different grading systems for gonioscopy: Shaffer, Spaeth, and Scheie. Although not uniform amongst all eye care professionals, Shaffer grading is the most commonly used.
The Shaffer system grades angles from 0 to 4, with 0 being the least open and 4 being the most open. It is done on measures of degrees of the angle open; however, in real-life terms, identifying the structures associated with the degrees is more practical. Grade 4 is essentially open to ciliary body band, grade 3 is at least open to scleral spur, grade 2 is open to pigmented or posterior trabecular meshwork, grade 1 is open to anterior trabecular meshwork maybe, and grade 0 is slit open or no structures visualized.9

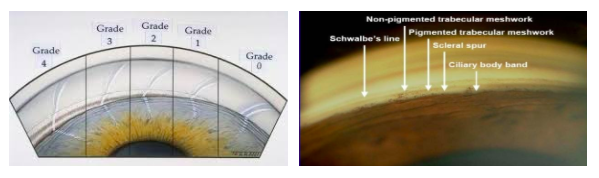
Figure 9: Shaffer gonioscopy grading system (left); anterior chamber angle with labeled angle structures (right).9,10
The Scheie grading system is on a similar scale to Shaffer. However, it is written in Roman numerals and it is reversed with grade 0 being most open and IV being the least open. The Spaeth grading system is a more detailed grading system that describes what the angle looks like with and without indentation gonioscopy, and includes the configuration and insertion of the iris. It is not as commonly used.
Once you have graded each quadrant of each of the patient’s eyes, your method for charting these findings must work for you, but it must also be clear and reproducible. This is to provide clear documentation for the patient’s follow-up appointment or for another provider who sees that patient, so that they can address whether the patient’s angle status is stable or has undergone a change. Using a cross format for charting, as well as documenting the amount of pigment and PAS seen in each quadrant, helps give further detail to the patient’s overall angle status.11

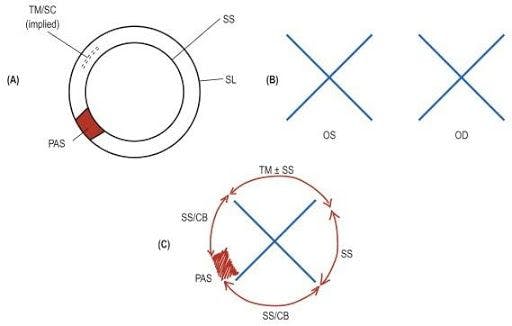
Figure 10: One method for documentation of gonioscopy findings. Cross method of representing the different angle quadrant findings.
Gonioscopy essentials:
- Educate the patient! Explain to them what the test entails and what they can expect. Having something touch their eye or approach their eye can be a daunting thought. They may feel the lens between their eyelashes.
- Administer a drop of topical anesthetic to both eyes.
- Make sure the patient as well as the doctor are seated comfortably.
- Align the patient’s lateral canthus with the black line on the slit lamp bar.
- Using a lens box or another elbow rest is important to prevent floating and instability in the practitioner’s arm.
- Ask the patient to look up or down while pulling the eyelids in the opposite direction, and insert the lens with flat edges flush and parallel to the eyelids.
- The practitioner can rest their fingers or hand on the patient’s cheek for more stability.
- Hold the gonioscopy lens with the handle of the lens, or remove the handle and hold the lens like a 90-diopter lens.
- To get a better view of the angle you are attempting to view, you can ask the patient to look toward the mirror you are visualizing.
One frequently asked question is whether there is still a role for provocation testing to confirm an angle closure diagnosis. Provocation has previously be performed to diagnose an eye for angle closure in patients with prior history of angle closure in the other eye, suspects of intermittent angle closure who may have pigment on anterior capsule of the lens or corneal endothelium, or symptom-free but anatomically narrow angles found on routine exam. A study looking at intraocular pressure (IOP) immediately pre- and post-dark-room prone provocative testing reported that there is a greater increase in IOP in PACS with four quadrants closed vs. two to three quadrants closed, but they as well as other studies have found no real insight into which of these patients with higher IOP post-DRPPT would develop acute or chronic disease over a 6-year follow up.12 And so this test has almost completely fallen out of favor for diagnosis.
Additional testing that can be done to enhance the information found on the anterior chamber angle include ultrasound biomicroscopy (UBM) and/or anterior segment OST (ASOCT). Both of these can give more objective data, such as the angle opening depth or width, corneal thickness, or iris thickness; however, they are still considered secondary tests to the standard of gonioscopy.
Plateau Iris Syndrome
One diagnosis on the angle closure spectrum that should be briefly included in the discussion of angle closure is Plateau Iris Syndrome. It is a form of angle closure where the ciliary body is large and either anteriorly positioned or rotated, physically pushing the iris up and bunching into and blocking the trabecular meshwork. It is typically found in younger patients. On gonioscopy you can see an “S-shape” of the iris, or “double-hump” sign.13 Definitive diagnosis is with failure of configuration change post laser peripheral iridotomy.
Patients with plateau iris can be monitored or observed, or can be referred for argon laser peripheral iridoplasty where laser is applied 360 in large spot sizes to thin the peripheral iris thus thinning and pulling the iris from blocking the anterior chamber able.14

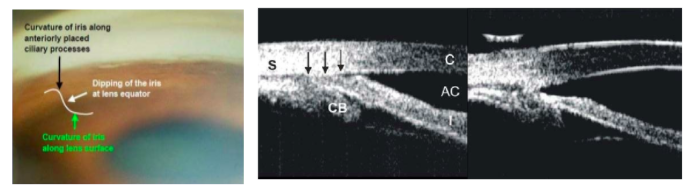
Figure 11: Gonioscopy of a patient with plateau iris syndrome showing the classic S-shaped or double hump sign (left); UBM of a patient with plateau iris syndrome prior to argon laser peripheral iridoplasty (ALPI) with the iris flush to the angle (black arrows) (central photo) and post ALPI with thinning of the iris and separation from the angle (right photo).
Treatment Options
Next steps
Once you diagnose your patient, what do you do next?
Different staging and treatment algorithms have been debated for patients within the PAC spectrum. Before you decide what to do next, you should first and foremost speak with your patient. Too often, practitioners spend a short amount of time actually sitting with patients and discussing their condition, quality of life, and treatment options and regimens.15 Given that primary angle closure is a chronic condition that will require frequent follow up regardless of management choice, forming a team between practitioner and patient by educating the patient and discussing the pros and cons of each treatment versus the observation option will develop a rapport and encourage follow up, compliance, and patient understanding of their condition.
Option 1: Observation
One option is to observe these patients at appropriate intervals with follow up visits, with no escalation in medical, laser or surgical management. According to the American Academy of Ophthalmology, some smaller observational studies suggest that a majority PACS will not develop PAC or PACG. Monitoring patients with grade 2-3 on gonioscopy for 6 month intervals with appropriate IOP management should IOP increase or escalation to referral for treatment with laser or surgery, is a reasonable approach.
If we look back at the pivotal glaucoma trials (AGIS, EMGT, OHTS, CNTGS, GLS, etc.), regardless of the treatment arm vs. observation arm in those trials, a percentage of patients, even if only a minority, lost vision. Therefore, although observation of these patients is a reasonable choice, close follow-up and being open to change in management for your patients might be advantageous. A thorough discussion with your patients and understanding of possible risks of management of observation vs. treatment is key.
Option 2: Laser Peripheral Iridotomy
The second option is referring the patient for a laser peripheral iridotomy (LPI). LPI as a management option for angle closure spectrum patients has been available since the 1980s, but its role is still debated. Some of the issues for this debate include a limited amount of prospective randomized control studies. Additionally, the studies that are available feature a lack of heterogeneity of subjects who span spectrum of angle closure in their ethnicity, degree of angle closure, and stage of glaucoma (if present).
The biggest advantage to performing a LPI is reducing the risk of advancing to acute angle closure or advancing to angle closure glaucoma.
Pro #1 of LPI: Reducing risk of progression to attack or glaucoma
The risk of progressing from angle closure suspect to angle closure attacks has been reported to range anywhere from 0-6.2%.16-18 Smaller studies reporting a smaller percentage of patients that are at risk for developing AACC; however, larger studies report up to 1.2-6.2% of patients at risk.17,18
There is an additional risk of progressing from angle closure suspect to angle closure glaucoma. A study published in 2003 from India found that 1 in 5 of the primary angle closure suspects went on to develop angle closure, and 1 in 4 of those patients went on to develop angle closure glaucoma. Over 5 years, the incidence of angle closure was reported at 22%. They also found that those who did progress to angle closure glaucoma were angle closure suspects bilaterally. Although the incidence of developing closure in this study was quite high, limitations of this study and similar studies were the small number of patients sampled, and thus these studies are not generalizable given their lack of diversity of ethnicities and stages of disease.
A pivotal randomized control trial published in 2019 known as the ZAP trial (Zhongshan Angle Closure Prevention) reported findings on 899 primary angle closure suspect patients. These patients had > 180º of appositional angle closure, without IOP elevation, PAS, or optic neuropathy. Followed over 72 months, each eye was randomized to either laser peripheral iridotomy or observation. The end point was angle closure defined as IOP >24 mm Hg on 2 occasions or development of >1 clock-hour of PAS, or an episode of AACC. They found that patients that had a LPI had a 47% reduction in event rate of AACC. They saw the number of eyes treated with LPI who developed PAC were about half those untreated (4.19/1000 eyes compared to 7.97/1000 eyes). This was a clinically modest but statistically significant benefit of LPI in patients with high risk findings such as 4 quadrants of angle closure. The strengths of this study included the large number of patients, the use of control eyes, and long follow up. The limitation is that this patient population was, again, a homogenous population (here all Chinese patients), and therefore it is hard to compare 1:1 to our diverse patient population in the US. This study gives a strong defense in performing a LPI, reducing the risk of AACC in PACS by almost ½.
Pro #2 of LPI: Reducing mechanism of pupillary block
The theory of how LPI reduces the risk of crisis or glaucoma, is by reducing the mechanism of pupillary block. A LPI allows aqueous to flow from posterior to anterior chamber via its opening, thus reducing intermittent shallowing or narrowing episodes when the patient’s eye is physiologically dilated. In turn the reduction of narrowing reduces the amount of intermittent IOP fluctuations overtime, which has been known to be one of the risk factors for developing glaucoma (fluctuations in IOP).
Pro #3 of LPI: Reducing risk of attack in those with retinal pathology
Another advantage to performing a LPI is reducing the risk of angle closure in patients that require frequent dilations, such as a patient with retinal pathology like diabetic retinopathy or a history of retinal detachment. Some small studies show these patients are at risk of not developing attacks, however some larger studies report the risk from 0.64-1.3%. This is approximately 1/100 patients, which is clinically significant if you can avoid AACC in even one patient.
Pro #4 of LPI: Reduce production of PAS
Performing a LPI reduces the amount of iridotrabecular contact that occurs on intermittent physiologic dilation. It has been reported that performing a LPI can increase the angle-opening depth anywhere from 47-110% increase.20 This decrease in ITC reduces the risk of PAS formation. It has been reported that, even in eyes with baseline PAS, no increase in PAS occurs after a LPI for up to one year.21 PAS, if developed 360, concludes in a completely occluded angle and increased risk of elevated IOP, crisis, and glaucoma. Therefore, performing a LPI can be preventative.


Figure 12: anterior chamber angle with PAS
Pro #5 of LPI: Benign, in-office
And, finally, we know that performing a LPI is performed in-office at a slit lamp with low risk to the patient.
Con #1 of LPI: Dysphotopsias
One of the most frequently discussed cons is that performing a LPI can cause dysphotopsias. About 2.7% (13/480) of patients who undergo LPI report monocular blurring or seeing a colored line post-LPI.23 Other studies have found similar percentages, although they do report that a majority of these dysphotopsias dissipate over time. Wientraub et al reported that linear dysphotopsias in the inferior hemifield (so after a superior LPI) even with full coverage of the upper eyelid, can produce dysphotopsias.24 Ike Ahmed et al further report that new-onset linear dysphotopsias were dependent more on the location of the LPI. They report that a superior LPI produced linear dysphotopsias 10.7% of the time vs. temporal LPI produce these dysphotopsias only 2.4% of the time.25 They suggest this because of a base-up prism effect of the tear meniscus at the upper eyelid margin redirecting light to the retina (Figure 13).25
Despite these percentages, it is important to remember that these dysphotopsias do improve over time, and if persistent there are options for symptomatic relief such as offering colored contact lens or even performing corneal tattooing.

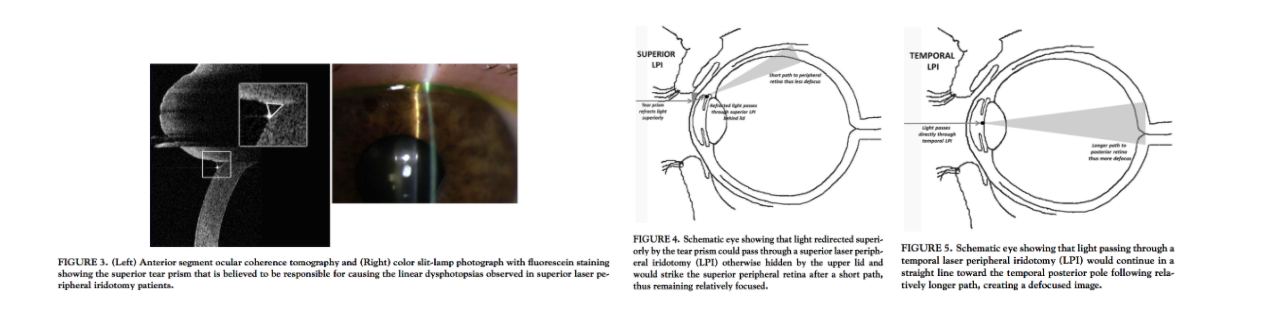
Figure 13: Base up prism effect of the tear meniscus at a superior LPI (left), superior vs. temporal LPI with respect to lid coverage and light reflection off the retina (middle, right).
Con #2 of LPI: post-procedure IOP spikes, post-procedure iritis, and posterior synechiae
IOP spikes have been reported as a consequence immediately after LPI. A review of prior studies looking at post LPI complications reported that and IOP increase (measured as 8- 17 mmHg) from baseline to immediately after LPI occurred between 6-10 % of patients (regardless of brimonidine drop administration pre-procedure) (Figure 14).20 The debate of whether to use brimonidine or an alpha agonist pre-procedure is therefore debatable. Typically, the IOP stabilizes before the patient leaves the clinic.


Figure 14: a review of IOP spike post LPI in different studies.
Post- LPI iritis can be seen in a percentage of patients who undergo LPI. The EAGLE study reported inflammation after LPI in 0.5% (1/211 eyes); the severity and duration of inflammation were not specified. Ahmadi et al reported grate 2+ uveitis in 69% (208/300 eyes), but also reported that most cases resolved within 48 - 72 hours, with topical corticosteroid treatment.26 Therefore, most specialists will give a short course of topical steroid post LPI to avoid this consequence.
And finally, post procedure posterior synechiae can form given the patent iridotomy, allowing aqueous flow to be altered flowing from the posterior to anterior chamber through this opening. The iris and anterior lens capsule can be then approximated closer to each other allowing frequent intermittent adherence and posterior synechiae formation over time.
Con #3 of LPI: Endothelial Cell Loss
It is controversial and therefore will be listed with the cons—however, endothelial cell loss after LPI is debatable. Endothelial cell density has been reported to decrease from baseline to 3 years after LPI in both treated (2%) and control eyes (0.9%).27 We know that over time endothelial cell count can decrease as aging occurs, so the question of whether the endothelial cell density decrease with LPI is significant enough to be a consideration.
Con #4 of LPI: Induction of Cataract
Finally, performing a LPI has been reported to increase the rate of cataract progression because of the alteration of aqueous flow. The aqueous contains lens proteins that bathe the lens, and by altering its path it can cause inherent loss of nutrients and appropriate flow over the lens leading to faster cataract induction. The Chennai Eye Disease Incidence Study reported a significant risk of cataract progression of 39% in LPI over 23% in no LPI.28 So, although cataract progression is inevitable with aging itself, performing a LPI will speed this process up. This is important when assessing a patient and explaining the advantages and risks of a LPI, especially in a young patient.
There are numerous aspects to consider when deciding whether to perform a LPI or not. It is important to think of all the above pros and cons as well as consider the patient’s social risk factors, such as their other medical conditions, their access to medical care, and their reliability for follow up and compliance with the observation vs. treatment option.
Option 3: Lens Extraction
Another option in the management of patients on the angle closure spectrum is phacoemulsification, or lens extraction. By debulking the anterior chamber, physical opening or widening of the anterior chamber angle can occur. Of course, this treatment option, although beneficial in many regards, can also have its risks.
Lens Extraction: Remove Pupillary Block

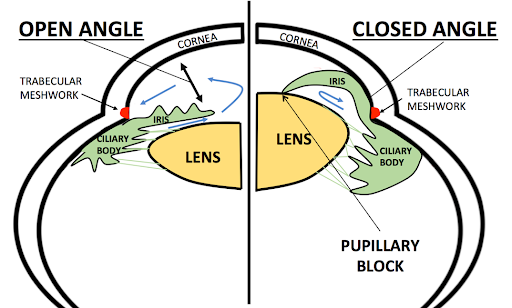
Figure 15: Enlarged lens (right) adding bulk to the anterior chamber leading to narrowing of the angle vs. small lens/IOL (left) debulking the anterior chamber leading to opening of the angle.29
The biggest argument for lens extraction is removing the main mechanism of angle closure, which is pupillary block. By removing the lens, the configuration of the anterior chamber angle structures opens beneficially. The EAGLE study reported that in newly diagnosed PAC and PACG patients the mean health status score (using the European Quality of Life -5 D Questionnaire) of patients who underwent lens extraction was higher than those who were randomized to the laser peripheral iridotomy plus medication group. They also found that mean IOP at 3 years was 1.18 mmHg lower in the lens extraction group compared to the LPI and medications group. Incremental cost-effectiveness favored lens extraction over the LPI and medication group. In addition, the study found that fewer of the lens extraction subjects (21%) needed further treatment or glaucoma medications to control IOP compared to the LPI plus topical medications group (61%).30
Pro #1 of Lens Extraction: IOP Lowering
The advantage, discussed briefly above, with removing the lens is that it has been shown to be more effective than LPI and topical medications for the prevention of long-term IOP rise. It has been reported that Mean IOP is 1 mm Hg lower in the lens extraction group over 3-year period.30
Although 1mmHg seems low, we know based on the EMGT and OHTS trials that this can reduce risk of glaucoma by 10%. Studies also report that pre-surgical IOP is the strongest predictor in the amount of IOP decrease post-operatively.31 This can help in determining which patients may benefit more from this management option.
Pro #2 of Lens Extraction: Improve Vision
One of the biggest benefits of this surgery, as we know, is that it can improve vision, contrast sensitivity, and quality of life. Looking at the patient’s lens status and cataract grading can help in identifying which patients may benefit most from this procedure.
Con #1 of Lens Extraction: Loss of Accommodation
One disadvantage of lens extraction, especially in younger patients on the angle closure spectrum is loss of their ability to accommodate. Loss of this conformation of the lens when focusing on near material (reading, fine artwork, etc.) can be a challenging prospect to adjust to. A discussion with the patient and a true understanding of what that means to the patient’s activities of daily living is key to determining if this will be the best option for the patient.

Figure 16: Accommodation of the phakic lens.32
Con #2 of Lens Extraction: Surgical Risk Factors
And, of course, a disadvantage of lens extraction includes the surgical risks factors of cataract surgery. These risks include bleeding, infection, worsening vision, loss of vision, and/or need for further surgery. However, cataract surgery on a whole is a very safe and common procedure, so these risks are in the cons category, but are more or less uncommon.
Performing lens extraction for patients on the primary angle closure spectrum has its benefits, yet its cons need to be weighed on a patient by patient basis as it is a more aggressive option.
Conclusion and References
Conclusion
Circling back to our 54-year-old Caucasian male patient with hypertension and narrow angles, what would we do next? Really, there is no correct answer. The answer is actually to discuss the options of observation, LPI, and/or lens extraction with the patient. Determine what are the patient’s risk factors and their likelihood to be compliant with follow up. We know that PACS can progress to PAC and PACG and we know that PACG can progress to bilateral irreversible blindness.
Knowing the information we know, and the possibility we have in our hands to prevent that blindness if treated appropriately, we have in our ability to help these patients with tools in our hands and it is up to a joint discussion with the patient to make the best decision for each patient that we see.
To be successful in caring for, diagnosing, and managing our patients on the primary angle closure spectrum, it is key to take a relevant history, complete a comprehensive eye exam including gonioscopy, and most importantly to have a thorough discussion with our patients about their condition. When choosing to observe or monitor a patient, forming a good rapport is essential for monitoring at appropriate intervals and escalating to appropriate referral for those who you believe may need further treatment such as a LPI or lens extraction.
References
- Figure 1: McWherter I, Mangan R. https://www.reviewofoptometry.com/article/angle-closure-a-bad-connection. 2016.
- Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006;90:262–267.
- Tham YC, Li W, Wong TY, et al. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040. Ophthalmology 2014;121(11):2081–2090.
- Frick KD, Gower EW, Kempen JH et al. Economic Impact of Visual Impairment and Blindness in the United States. Arch Ophthalmol. 2007;125: 544-550.
- Figure 3: Radhakrishnan S, Chen PP, Junk AK, et al. Laser Peripheral Iridotomy in Primary Angle Closure. Ophthalmology 2018. 125(7): 1110-1120.
- Figure 4: Adrakani S, Kongprawechnon W, Theeramunkong T, et al. Parameterization of Limbus Distance in Van Herick method’s angle closure glaucoma diagnosis. 2016. 7th International Conference of Information and Communication Technology for Embedded Systems (IC-ICTES)
- Figure 5: Alward WLM, Longmuir RA. Principles of Gonioscopy. 2017
- Figure 8: Spaeth GL, Fellman RL. Duanes Clinical Ophthalmology. Chapter 44 Vol 3: Gonioscopy.
- Figure 9: Salmon JF. Gonioscopy. In Shaarawy TM, Sherwood MB, Hitchings RA, Crowston JG, ed. Glaucoma. 2nd ed. London: Elsevier Inc., 2015. p169-178
- Figure 9: USC Roski Eye Institute (photo right).
- Figure 10: https://entokey.com/clinical-interpretation-of-gonioscopic-findings/
- Friedman DS, Chang DST, Jiang Y. Darkroom prone provocative testing in primary angle closure suspects and those with open angles. British Journal of Ophthalmology. 2019;103(12).
- Figure 11: Slide share Dr. Ashish Gupta and Dr. Tiwari.
- Figure 11: Dorairaj S, Tsai JC, Grippo TM. Changing Trends of Imaging in Angle Closure Evaluation.
- Friedman DS, Chang DST, Jiang Y. Darkroom prone provocative testing in primary angle closure suspects and those with open angles. British Journal of Ophthalmology. 2019;103(12).
- Thomas R, George R, Parikh R, et al. Five year risk of progression of primary angle closure suspects to primary angle closure: A population based study. Br J Ophthalmol 2003;87:450.
- Ye T, Yu Q, Peng S, et al. [Six year follow-up of suspects of primary angle-closure glaucoma]. Zhonghua Yan Ke Za Zhi 1998;34:167.
- 7. Wilensky JT, Kaufman PL, Frohlichstein D, et al. Followup of angle-closure glaucoma suspects. Am J Ophthalmol 1993;115:338.
- He M, Jiang Y, Huang S, et al. Laser peripheral iridotomy for the prevention of angle closure: a single center, randomized controlled trial. Lancet 2019; 393:1609-18.
- Radhakrishnan S, Chen PP, Junk AK, et al. Laser Peripheral Iridotomy in Primary Angle Closure. Ophthalmology 2018. 125(7): 1110-1120.
- Lim LS, Aung T, Husain R, et al. Acute primary angle closure: configuration of the drainage angle in the first year after laser peripheral iridotomy. Ophthalmology. 2004;111:1470-1474
- Figure 12: Courtesy of Steven T. Simmons, MD.
- Murphy, P.H., Trope, G.E. Monocular blurring. A complication of YAG laser iridotomy. Ophthalmology. 1991;98:1539–1542
- Weintraub, J., Berke, S.J. Blurring after iridotomy. Ophthalmology. 1992;99:479–480
- Ahmed IK, et al. Dysphotopsia after temporal versus superior laser peripheral iridotomy: a prospective randomized paired eye trial. Am J Ophthalmol. 2014 May;157(5):929-35
- Ahmadi M, Naderi Beni Z, Naderi Beni A, Kianersi F. Efficacy of neodymium-doped yttrium aluminum garnet laser iridotomies in primary angle-closure diseases: superior peripheral iridotomy versus inferior peripheral iridotomy. Curr Med Res Opin. 2017;33:687-692.
- Kumar RS, Baskaran M, Friedman DS, et al. Effect of prophylactic laser iridotomy on corneal endothelial cell density over 3 years in primary angle closure suspects. Br J Ophthalmol. 2013;97:258e26
- Vijaya L, Asokan R, Panday M, George R. Is prophylactic laser peripheral iridotomy for primary angle closure suspects a risk factor for cataract progression? The Chennai Eye Disease Incidence Study. Br J Ophthalmol 2017;101:5:665-670
- Figure 15: University of Utah
- Azuara-Blanco A, Burr J, Ramsay C, et al, EAGLE Study Group. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomized controlled trial. Lancet. 2016;388:1389-1397.
- Thomas R, Walland M, Thomas A, Mengersen K. Lowering of intraocular pressure after phacoemulsification in primary open-angle and angle-closure glaucoma: a Bayesian analysis. Asia Pac J Ophthalmol (Phila) 2016; 5:79–84
- Figure 16: Tim Root
