






Characterized by progressive corneal thinning and conical protrusion, keratoconus is an ectatic corneal disorder. Early diagnosis is crucial, as keratoconus can present complications for vision—including myopia and irregular astigmatism—and surgical outcomes.
In this article—with a free downloadable Corneal Crime Scene Report—we’ll go over the dos and don’ts of early keratoconus detection, diagnostic tips, treatment options, and clinical pearls so you can catch the curve.
What is keratoconus?
Keratoconus (KC) is a bilateral but often asymmetrical biomechanical weakness leading to distortion of corneal shape, resulting in myopia, astigmatism, higher-order aberrations, and loss of best spectacle correction.
Noninflammatory thinning, abnormal posterior elevation (ectasia), and corneal thickness distribution measured using tomography are diagnostic requirements.1 Keratoconus and pellucid marginal degeneration (PMD) are manifestations of the same disorder and are differentiated by the thinning location and spatial distribution pattern.1
Risk factors for keratoconus include:1
- Family history of ectasia
- Atopy
- Connective tissue disorders
- Eye rubbing
- Down syndrome
- Asian and Arabian ethnicity
Familial inheritance is primarily autosomal dominant with incomplete penetrance.2,3 The highest incidence is in young adults between 20 and 30 years of age,1 but it may be identified in children and teenagers.
Keratoconus was historically identified by excessive keratometry values and loss of best corrected vision, and managed using gas permeable (GP) contacts until a corneal transplant was required. This resulted in a significant reduction of quality of life.4,5
Get the download with tips for diagnosing keratoconus!

Corneal Crime Scene Report
Download this detective-themed cheat sheet to learn which clues to follow to diagnose keratoconus with different imaging modalities.

Case report: Tracy Schroeder Swartz, OD, MS, FAAO
A 26-year-old male was referred by a local optometrist for a keratoconus evaluation. He presented for a glasses exam when “his good eye became blurry.” The optometrist found mild astigmatism OD (PL -0.25 x 120, 20/25-2) and mild myopia with severe astigmatism OS (-1.75-6.00 x 145, 20/100). The referring optometrist was concerned about keratoconus due to a scissor reflex OS during retinoscopy.
Figure 1: Corneal topography imaging of the patient OD and OS.


Figure 1: Courtesy of Tracy Schroeder Swartz, OD, MS, FAAO.
The topography revealed significant inferior steepening with an I-S value of 3.6D OD and 12.2D OS. Based on the Placido topography, we referred the patient to our main clinic for a Pentacam. This test revealed severe posterior elevation with abnormal thinning spatial distribution.
Since the patient did not have a history of prescribed vision correction, we assumed he was progressing and referred him for corneal collagen cross-linking (CXL).
More on identifying keratoconus and early intervention strategies
Elevation-based tomography enables identification of ectasia at an earlier stage, affecting prevalence and accounting for the increase in studies performed using this technology. The prevalence of keratoconus varies depending on the country, location, and technology used. Higher prevalence has been reported in Middle Eastern countries, India, and China, with lower prevalence in northern Europe, the United States, and Japan.1,6
Keratoconus progresses more quickly in children,7,8 making early detection critical. The cone is typically more centrally located in children, causing less irregular astigmatism. This, combined with the masking effect of high accommodative power in younger patients, may result in more severe disease at initial diagnosis.9
Modern management has evolved significantly, prioritizing early detection, close monitoring, and timely intervention through cross-linking. This approach is followed by visual rehabilitation and ongoing monitoring for disease progression, establishing a new standard of care. However, early intervention presents challenges, which are discussed herein.
How do clinicians diagnose keratoconus?
A clinical evaluation can reveal a plethora of clues leading to a diagnosis of keratoconus. During the early stages, a careful case history is essential. Questions regarding family history, asthma, eczema, ocular allergies, and eye rubbing should be asked.
Atopy has been found to be a significant risk factor for keratoconus, present in 85% of patients under 18 years.10 During intake, also ask about quality of vision and glare or starbursts at night, as corneal ectatic changes may lead to higher-order aberrations.11
When conducting testing, autorefractor / autokeratometer results offer excellent clues on abnormal astigmatism, keratometry (K) values, and ocular asymmetry. Red flags include inconsistent readings, oblique axes, K-values greater than 47D, and asymmetry in refractive errors and K-values between the eyes.12
Retinoscopy may reveal a scissoring reflex, which is a sensitive test when screening for keratoconus.13 On refraction, look for unexpected myopia progression or new astigmatism development. It may be difficult to obtain strong endpoints and crisp vision due to irregular astigmatism.
At the slit lamp, early keratoconus changes are hard to detect. Only with progression might one observe Fleischer’s ring, central striae, ectasia, thinning, or scarring on the cornea. Eyelid evaluation offers meaningful clues on allergies and floppy eyelid syndrome. Papillae, associated with allergic conjunctivitis, can be seen on the palpebral conjunctiva in individuals with keratoconus.
Eyelid laxity and easy lid eversion are features of floppy eyelid syndrome, also commonly found with keratoconus.14 This may put the patient at risk for unintended “eye rubbing” while sleeping on their side, as eyelid eversion may allow the cornea to rub against bedding.
Case report: Gloria Chiu, OD, FAAO, FSLS
A 31-year-old Middle Eastern male had been diagnosed with keratoconus in 2022. At that time, he reported progressively decreasing vision in glasses for 1 year prior, along with eye rubbing.
Incoming uncorrected visual acuity (VA) was 20/40 OD and 20/50 OS, as glasses “didn’t work.” Slit lamp evaluation revealed corneal steepening OU. Ultrasound pachymetry showed thinning at 478μm OD and 442μm OS.
Figures 2 and 3: K-values were 47.66 / 46.57D OD and 48.96 / 48.45D OS, and corneal topography confirmed ectasia with Placido ring distortion OU.




Figures 2 and 3: Courtesy of Gloria Chiu, OD, FAAO, FSLS.
Given the progressive changes, the patient underwent epi-off CXL OU within a month of diagnosis. Although manifest refraction and vision continued to evolve for several months during corneal remodeling, vision eventually stabilized. K-values remained stable over time.
Given the progressive changes, the patient underwent epi-off CXL OU within a month of diagnosis. Although manifest refraction and vision continued to evolve for several months during corneal remodeling, vision eventually stabilized. K-values remained stable over time.
Current manifest refraction:
- Plano -1.00 x 060 20/20
- -0.75 -2.75 x 125 20/20-
His keratoconus is stable, and he has good vision in glasses and soft toric contact lenses.
Using imaging to diagnose keratoconus
Imaging is imperative for identifying the most subtle clues. Corneal topography may reveal distorted Placido rings and inferior steepening on the corneal surface, despite having normal K-values.
Corneal tomography further delineates abnormal corneal steepening, corneal thickness values, anterior and posterior elevation data, and indices assessing keratoconic risk. Early keratoconus often impacts the posterior cornea first,15,16 so tomography offers the best chance to detect changes early.
Imaging can also help to differentiate regular astigmatism from abnormal ectasias and pellucid marginal degeneration.
Don't forget to check out the Corneal Crime Scene Report!
What are the common management strategies for keratoconus?
There are a few management options for keratoconus, higher amounts of myopia and astigmatism or irregular astigmatism that reduce spectacle acuity may require contact lenses for functional vision.
Contact lens options included soft toric, gas permeable, hybrid, and scleral lenses.
Contact lenses for keratoconus
Today’s contact lens designs are better than ever. It’s important to promptly fit our keratoconus patients after diagnosis to provide optimal vision, preventing decreased productivity at work or school.
Traditional soft contact lenses can provide some correction for mild stages of keratoconus,17 but typically do not provide better visual acuity than spectacles. Thicker, keratoconus-specific soft lens designs may provide increased acuity.18,19 However, the utility of any soft toric lens diminishes as the disease progresses and the patient’s astigmatism becomes irregular.17
GP contact lenses are the standard of care for keratoconus. The smooth anterior surface of the lens and the lacrimal lens that fills in the corneal irregularities combine to reduce the optical distortion caused by the condition.
Initially, standard corneal GP lenses work well, but for moderate conditions, a special keratoconus design better aligns with the curvatures of the eye. Hybrid contact lenses with a gas permeable center and soft skirt are suitable for mild to moderate keratoconus. Still, they are less effective for advanced keratoconus, as their parameters are limited and the soft skirt can complicate lens removal.
Unlike small-diameter GP lenses, which can easily decenter or dislodge with the blink, scleral lenses tuck underneath the eyelids, staying in position. The patient will not feel the edges upon blinking, enhancing comfort.
Because the lens rests gently on the sclera/conjunctiva, the patient views through the optical center of the lens, maximizing vision. Due to their increased sagittal depth, they can also correct advanced keratoconus.
Figure 4: Ample corneal clearance with a scleral contact lens fit for early KC.


Figure 4: Courtesy of Susan J. Gromacki, OD, MS, FAAO, FSLS.
Although they are more difficult to fit and more expensive, they are a popular choice—even for early keratoconus patients. A piggyback system (corneal GP on top of a soft CL) is utilized rarely due to limited oxygen to the cornea, expense, and the challenge of caring for both soft and GP lenses.
Case report: Susan Gromacki, OD, MS, FAAO, FSLS
A 21-year-old male college student noticed blurred vision OD. He saw two different eye doctors (one optometrist and one ophthalmologist) a total of seven times. They diagnosed dry eye and prescribed Restasis and artificial tears. But nothing helped his vision. He presented to the office during a school break.
He presented with uncorrected VAs of 20/25 OD and 20/20 OS. Autorefraction showed 2.00 diopters of cylinder (DC) with an 8/10 confidence score for the right eye. Refraction was +1.00-1.25 x 007, 20/20.
Topography showed a red-colored, round area of steepening just inferior to the optical center of the eye, pathognomonic for keratoconus, and a Tkeratoconus of 2.
Figure 5: Corneal topography OD illustrating inferior corneal steepening.

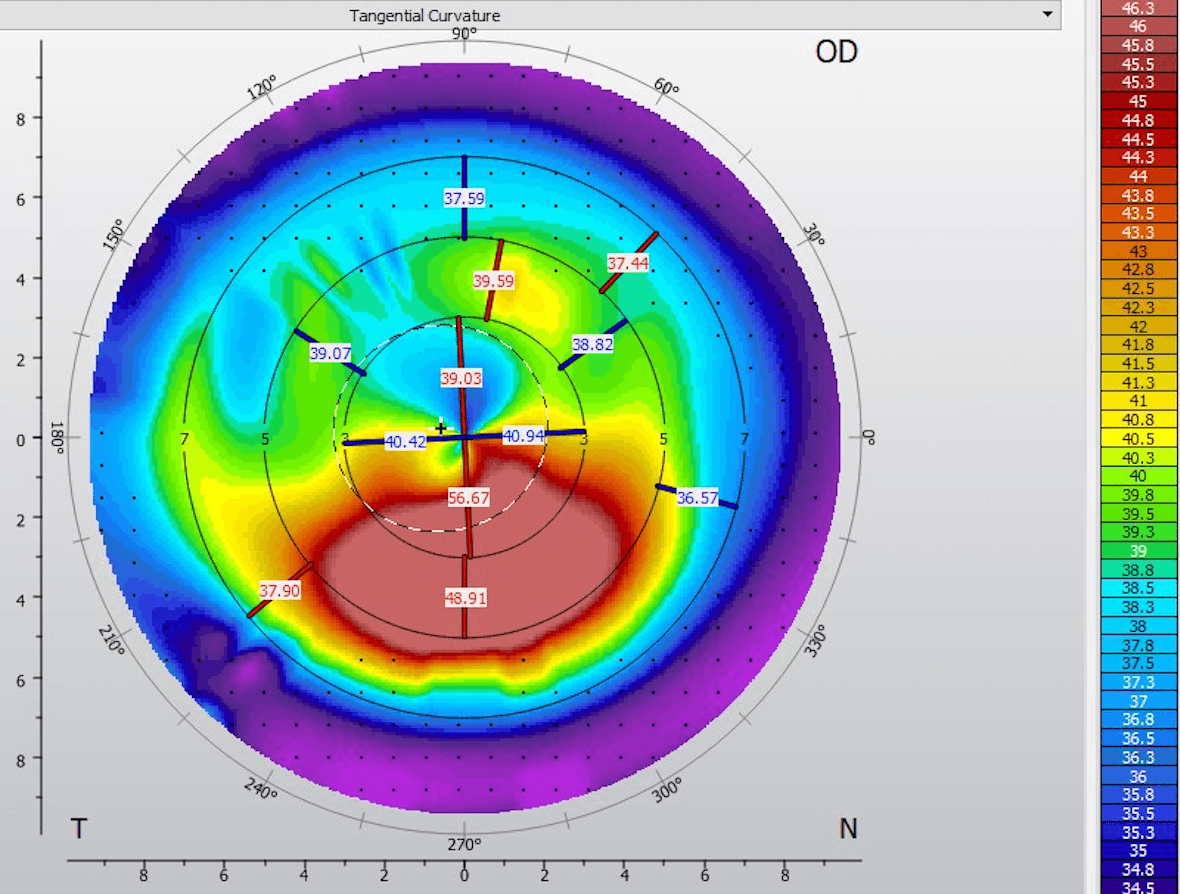
Figure 5: Courtesy of Susan J. Gromacki, OD, MS, FAAO, FSLS.
The patient has a mild case of keratoconus and was eligible for either corneal or scleral GP contact lenses. Since he is a soccer player, we decided to fit him with a scleral contact lens OD to ensure optimal comfort and lens retention.
With this lens, he achieved 20/20 vision and remarked that his vision was sharper than when wearing glasses. I referred him to a corneal specialist for CXL, which the surgeon performed on both eyes (OU).
The previous doctors were not entirely wrong, as he had a reduced tear breakup time OD. But this was because the tears were breaking up over the cone, not because the young man wasn’t making enough tears.
The take-home message is twofold:
- A patient with a best-corrected vision of 20/20 can still have keratoconus. If low contrast VA had been measured, it certainly would have been less than 20/20.
- Any time a young adult sees less than 20/20 and/or complains about their vision, consider keratoconus.
Don't forget to check out the Corneal Crime Scene Report!
Corneal collagen cross-linking
Continuing with the theme of early detection, early intervention to halt ectatic progression should be our immediate next thought, and is also endorsed by the Cornea Society and American Academy of Ophthalmology (AAO) Preferred Practice Patterns.20,21
When keratoconus is progressive, cross-linking should be scheduled promptly to avoid additional loss of best-corrected vision.18 US Food and Drug Administration (FDA)-approved CXL fits in this arena. There is only one FDA-approved option for CXL today, which is epithelium-off (epi-off CXL) using iLink (Glaukos). Under investigation with the FDA is a less invasive, epithelium-on cross-linking, Epioxa (Glaukos).
Giving the conclusion early, the ultimate goal with cross-linking is to arrest corneal ectasia disease progression, freezing the cone in place. It should make sense that performing cross-linking when the uncorrected visual acuity (UCVA) is 20/40 and the best-corrected spectacle acuity (BCSA) is 20/20 provides a more favorable vision outcome for patients than a procedure with 20/400 UCVA and 20/50 BCSA.
Understanding CXL and setting patient expectations
As introduced, CXL is the only keratoconus treatment specifically performed for and labeled for halting ectatic disease progression. iLink with Photrexa and Photrexa Viscous (Glaukos) for epithelium-off cross-linking was approved by the FDA. iLink is also the only insurance-reimbursed form of cross-linking, and in my opinion, to date, has the most efficacious data.
Procedurally, the first step is to create a central 7 to 9mm epithelial defect. Then, 0.1% riboflavin ophthalmic solution (Photrexa, Glaukos) or 0.1% riboflavin ophthalmic solution / 20% dextran (Photrexa Viscous, Glaukos) is applied to the cornea for 30 minutes.
Next is UVA light (370nm) exposure to activate the riboflavin. This lasts an additional 30 minutes while the riboflavin/dextran drops are continuously instilled. Finally, a bandage contact lens is applied to the cornea to aid in epithelialization.
Similarly in importance to early intervention with cross-linking, setting post-operative expectations and delivering high-level post-op care will lead to patient success.
Before the cross-linking procedure, I want patients to understand three key expectations:
- With epi-off CXL, there will be moderate discomfort (photophobia, burning, foreign body sensation, etc) that will improve over time.
- After cross-linking, vision is going to be worse for 1 to 4 weeks before it gets back to baseline, and potentially marginally exceeds pre-operative acuity over time.
- Patients can typically get back into their pre-operative scleral lenses and or soft lenses within 1 week. Commonly, a new fit for contact lenses is 1 to 3 months.
- Unfortunately, cross-linking is not a refractive surgery aimed at helping patients see better, but rather a tool to stabilize the cornea. Once the cone is stabilized, the refractive toolbox widens for options to improve vision acuity and quality.
Case report: Mitch Ibach, OD, FAAO
A 40-year-old female nurse practitioner was referred for keratoconus OD. She has a family history of keratoconus. Her father had corneal transplants in his 30s.
Referring auto-K’s:
- OD: 40.0 @ 026/43.2 @ 116
- OS: 41.6 @ 178/43.1 @ 088
Figures 6 and 7: Corneal topography maps OD and OS, respectively.



Figures 6 and 7: Courtesy of Mitch Ibach, OD, FAAO.
- OD: -0.75-2.25x070 (20/25); improves with RGP; moderate bump in cyl (>1D) in last year
- OS: -2.25-1.50x005 (20/20); no large change to refractive error
The patient denies daytime rubbing. She sleeps on her left side but wonders if she rubs OD at night. She is a previous contact lens wearer but discontinued and switched to glasses due to intolerance. She’s motivated to return to soft contacts and/or consider refractive surgery.
Diagnosis: Progressive keratoconus OD and OS
- OD: >1D increase in refractive astigmatism
- OS: Shows >1D increase in Kmax from auto-K’s to Pentacam
We scheduled an epi-off CXL procedure for both eyes, 4 to 6 weeks apart. The condition's progression was confirmed by an increase in Kmax, as reported by the referring doctor’s manual keratometry. After the surgery, tomography is repeated every 6 months.
If the condition remained stable after 12 to 18 months, topography-guided photorefractive keratectomy (PRK) based upon epithelial mapping could be considered. Our goal is to reduce dependence on specialty contact lenses, and any improvement in uncorrected visual acuity would be an added benefit.
Conclusions
Optometry plays a critical role in keratoconus management because so many of these patients start in our offices, and most will return to optometry after surgery for continued visual improvement and care.
After CXL, diligent monitoring of crosslinked corneas using topography or tomography to verify stability, combined with visual rehabilitation, is required to help our patients manage their sight and ocular health in the long term.8
