



In the early 1970s, initial efforts to reduce intraocular pressure (IOP) using a laser, such as goniopuncture with the Q-switched ruby laser, produced only temporary, if any, outcomes.
A more promising development was that of the argon laser trabeculoplasty (ALT), which involved high-energy photocoagulation of the trabecular meshwork.
This, unfortunately, was associated with the side effect of acute post-laser IOP spikes, the development of peripheral anterior synechiae (PAS), and more encapsulated blebs in drainage surgery.1,2
Development of selective laser trabeculoplasty
Despite these challenges, these early attempts laid the groundwork for the development of selective laser trabeculoplasty (SLT), which was introduced by Latina et al. in 1995.3
This technique utilizes a 532nm Q-switched, frequency-doubled neodymium-doped yttrium aluminum garnet (Nd:YAG) laser with a shorter pulse duration than ALT (3.0ns vs. 0.1s).3
SLT has proven effective in lowering IOP, and from a histopathological perspective, it appears to be less destructive.3 Therefore, its repeatability has been underscored as a potential advantage since it can be performed without significant risk.
SLT mechanism of action
The goal of SLT is to reduce intraocular pressure; this is achieved by using laser energy of wavelength 532nm to target melanin-containing cells of the trabecular meshwork (TM). The selective nature of the laser helps to target pigmented cells while sparing non-pigmented cells.
The temperature of these melanin-containing cells rises as they absorb the laser energy. This leads to heat generation (photothermal) and mechanical disruption (photomechanical) of the targeted cellular structures, ultimately leading to an increase in trabecular outflow structure.4
Furthermore, the photomechanical and photothermal effects of the SLT trigger biological responses within the pigmented cells. This leads to the induction of matrix metalloproteinase, cytokine secretion, gene expression, and TM remodeling—which, in effect, facilitates aqueous drainage via the TM.5 This reduced resistance at the level of the TM improves outflow, leading to a decrease in IOP.6
Indications for selective laser trabeculoplasty
SLT is useful in lowering IOP in patients with ocular hypertension (OHT) with open angles and primary open-angle glaucoma (POAG). It has also been found to be effective in patients with secondary open-angle glaucoma, such as pseudoexfoliative glaucoma, pigmentary glaucoma, and steroid response glaucoma.7,8
SLT is an incredible option for patients who have difficulty with medication compliance due to memory issues, mobility limitations such as Parkinson’s, and intolerable side effects of topical medications. It can also be used in eyes that have had prior incisional glaucoma surgery or repeated in patients who have had a successful response to initial treatment that has worn off.9,10
SLT patient selection
As noted prior, SLT can be used in patients with open-angle glaucomas. It is important to perform gonioscopy to ensure that patients are candidates for SLT based on their angle anatomy. Patients with narrow angles without iridotrabecular contact or PAS (as these are technically open angles) may also benefit from SLT.
The key point is that the pigmented trabecular meshwork needs to be easily visualized in order to perform this procedure safely and reduce the risk of complications.
Figure 1 illustrates important angle anatomical structures visualized via gonioscopy.
Figure 1 illustrates important angle anatomical structures visualized via gonioscopy.

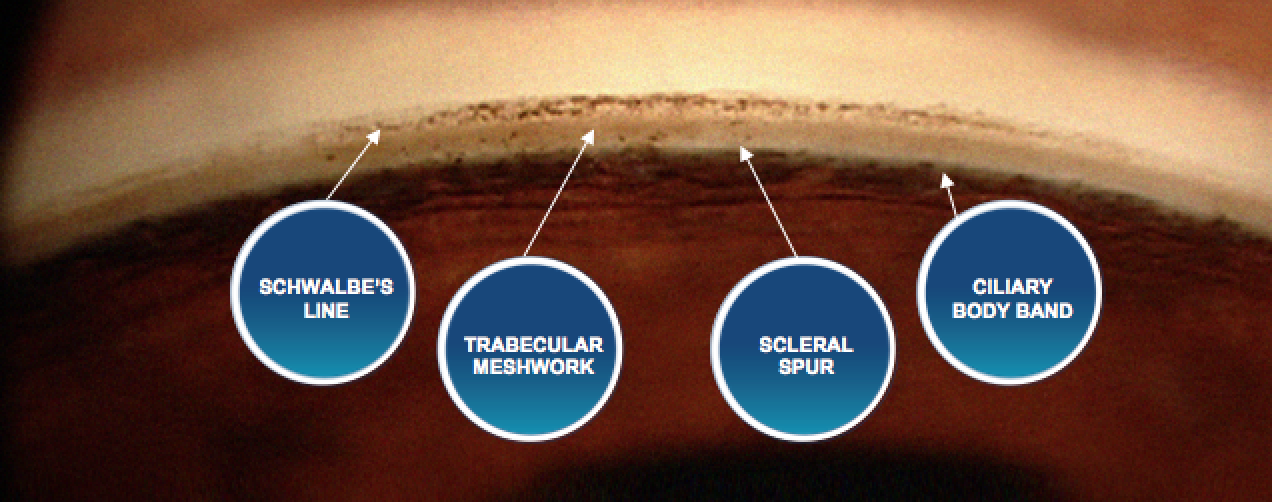
Figure 1: Courtesy of Constance Okeke, MD, MSCE.
Contraindications for SLT
SLT is contraindicated in patients with inflammatory glaucoma, iridocorneal endothelial (ICE) syndrome, congenital glaucoma, and neovascular glaucoma. It is not contraindicated in angle recession glaucoma but has not been shown to be effective, likely due to TM scarring and angle distortion.
If there is no response to SLT in one eye, providers will oftentimes not perform SLT in the contralateral eye.11 Although the procedure is typically painless, some patients may have high levels of anxiety and not be able to tolerate the contact lens or laser procedure in the office.
Studies on SLT treatment outcomes
SLT success rates
Experts estimate that SLT used as a first-line treatment can reduce IOP by 25 to 30% on average, with about 85 to 90% of patients responding well to first-line SLT.8 This response can be even greater in patients with pigmentary glaucoma or pseudoexfoliation glaucoma but can also be associated with an initial IOP spike.
In a large retrospective observational study performed in the United Kingdom, 831 eyes treated with SLT were analyzed.12 The study defined failure of SLT as IOP above 21mmHg, IOP reduction of less than 20% from baseline, or an increase in glaucoma medications from baseline.
Survival analysis showed that 70% of patients demonstrated treatment success at 6 months, 45% at 12 months, and 27% at 24 months.12 Other studies demonstrate a similar waning effect of the IOP-lowering effect over time.
Results from the LiGHT Trial
In 2022, Gazzard et al. published findings from the LiGHT (Laser in Glaucoma and Ocular Hypertension) trial, which shifted the practice patterns of many ophthalmologists.13 This was a prospective, multicenter, randomized controlled trial of 692 treatment-naive patients with open-angle glaucoma or ocular hypertension who were randomized to either initial SLT or eye drops.
In 69.8% of eyes, the SLT arm remained at or less than the target IOP without the need for medical or surgical treatment. Conversely, 26% of the eyes in the drops arm exhibited disease progression compared to 19.6% of eyes in the SLT arm.
Of note, 32 eyes in the drops arm and 13 eyes in the SLT arm required trabeculectomy. There were no serious adverse events secondary to laser treatment. Overall, this study showed SLT to be clinically and cost-effective in patients with POAG and OHT over 6 years.13
Predictive factors for SLT success
In 2020, Kuley et al. published a large retrospective case series of patients undergoing SLT and found that higher IOP and more angle pigment before SLT correlated positively with success.
Age, total SLT power, severity of glaucoma, and prior treatments were not associated with SLT success or failure.14 Elahi et al. found that SLT outcome was strongly correlated to the outcome of the fellow eye (odds ratio=17.33).15
SLT repeatability
Real-world data and survey studies have indicated that SLT can be an effective repeatable procedure. In one such study, Polat et al. demonstrated this in their retrospective review of 38 patients who underwent two successive SLTs in whom the first SLT was successful for at least 6 months.
Their data showed a significant reduction in IOP (~3.25mmHg) after the second treatment that was comparable to the initial reduction (~4.35mmHg) and a longer median survival time for repeat SLT compared with initial SLT.10 Although there is no current data on the rates of retreatment, many providers are repeating SLT, given the evidence that it works.
5 clinical pearls for SLT
1. Manage patient expectations.
I like to explain to the patient exactly what to expect before undergoing the laser treatment. I discuss post-operative drops beforehand (I usually use prednisolone acetate 1% QID for 4 days to make it easy for the patient to remember).
I also like to stress that not everyone will respond to the laser and that the IOP could transiently increase, so they are not concerned if an IOP spike does occur.
2. Administer a pre-operative IOP-lowering therapy.
I typically will give the patient either a drop of apraclonidine or brimonidine if there are no contraindications.16
3. Get comfortable before starting the procedure.
Typically this procedure takes less than 5 minutes, but this can be drawn out if you are not seated comfortably and have to continue to adjust yourself or the patient during the treatment.
Set the patient to a height that is comfortable for you and use a rest for your elbow to avoid fatigue.
4. Realize the view is everything.
There are a variety of lenses with one or more mirrors that all work very well for this procedure. A viscous jelly such as Goniovisc, lidocaine gel, or lubricant gel works as a great coupling agent to improve the view (so long as there are no bubbles!).
Establishing a clear view of the angle is critical to performing this procedure quickly and safely.
5. Know how to do dynamic gonioscopy.
A baseline knowledge of the normal anatomy of the angle is very important. However, sometimes the angle can be confusing! A Sampaolesi’s line can masquerade as pigmented TM to the unsuspecting ophthalmologist.
By doing dynamic gonioscopy (pushing on the eye with the lens), you can reveal more posterior structures and confirm the identity of the structures you are looking at. The ciliary body band is a very clear landmark that can help you to orient yourself.
Sometimes there may only be a Sampaolesi’s line inferiorly, so I look for symmetry of the pigmented TM in those tricky quadrants to the pigmented TM in the more obvious quadrants.
Conclusion
As drop compliance remains an issue ophthalmologists have battled for decades, SLT offers a unique opportunity to provide effective IOP lowering without depending on patients to use medications properly and consistently.
Significant data confirms this procedure's efficacy, and many practitioners are transitioning to using SLT as a first-line treatment for glaucoma. The repeatability and ability for use in a variety of patients with and without a history of incisional glaucoma surgery offers flexibility in options for IOP lowering.
With a very low side effect profile (possibility of IOP spike, inflammation, and no response), selective laser trabeculoplasty is an excellent treatment option for patients who are having difficulty using eye drops regularly or who have intolerable side effects.
While there is still more work to be done in areas, such as the best amount of energy to use while performing SLT, the data already present is promising and expands our glaucoma treatment toolbox.
