


Patients with cortical blindness present with devastating vision loss without any remarkable anterior or posterior segment abnormalities. The presence of fully intact pupillary reflexes further compounds the problem, making the diagnostic process of cortical blindness (CB) complex and challenging.
This article will provide essential information so optometrists can understand cortical blindness, leading to timely treatment, management, and improved visual outcomes.
Cortical blindness terminology
The terms cortical blindness, cerebral blindness, and cortical visual impairment are sometimes used interchangeably, but they each have their own distinct meanings.
- Cortical blindness: Defined as vision loss due to damage to the primary visual striate cortex, V1, in the occipital lobe of the brain.1
- Cerebral blindness: Structurally, cerebral blindness refers to damage at V1 and the surrounding subcortical visual pathway. As CB refers to dysfunction at V1, CB can be thought of as a subtype of cerebral blindness.1
- Cerebral/cortical visual impairment (CVI): The preferred terminology used by pediatric specialties because it describes a more variable condition associated with neuroplasticity.2
Prevalence of cortical blindness
The prevalence of CB in the general population has not been adequately investigated, but CB is thought to be fairly uncommon.1,3 In 2003, Flanagan et al. reported a prevalence rate of 161 per 100,000 for the incidence of newly certified visually impaired children under 16 years of age.4
Review of ocular and brain anatomy
A brief overview of the ocular and brain anatomy can assist with the appreciation of the terminology and pathophysiology of CB.
Visual pathway
Visual information from the retina travels from the optic nerve to the optic chiasm, where the inner retinal fibers cross over and rejoin in the optic tract before reaching the lateral geniculate nucleus (LGN) in the thalamus.
From the LGN, optic radiations carry the data to the primary visual striate cortex in the occipital lobe, known as V1. The surrounding subcortical areas V2 to V5 link to other parts of the brain.1
Figure 1 illustrates the primary visual striate cortex and subcortical areas of the occipital lobe. The diagram shows the (a) frontal lobe at the anterior region of the brain with the (b) occipital lobe at the posterior end. The (c) subcortical areas surround the (d) primary visual striate cortex, V1.

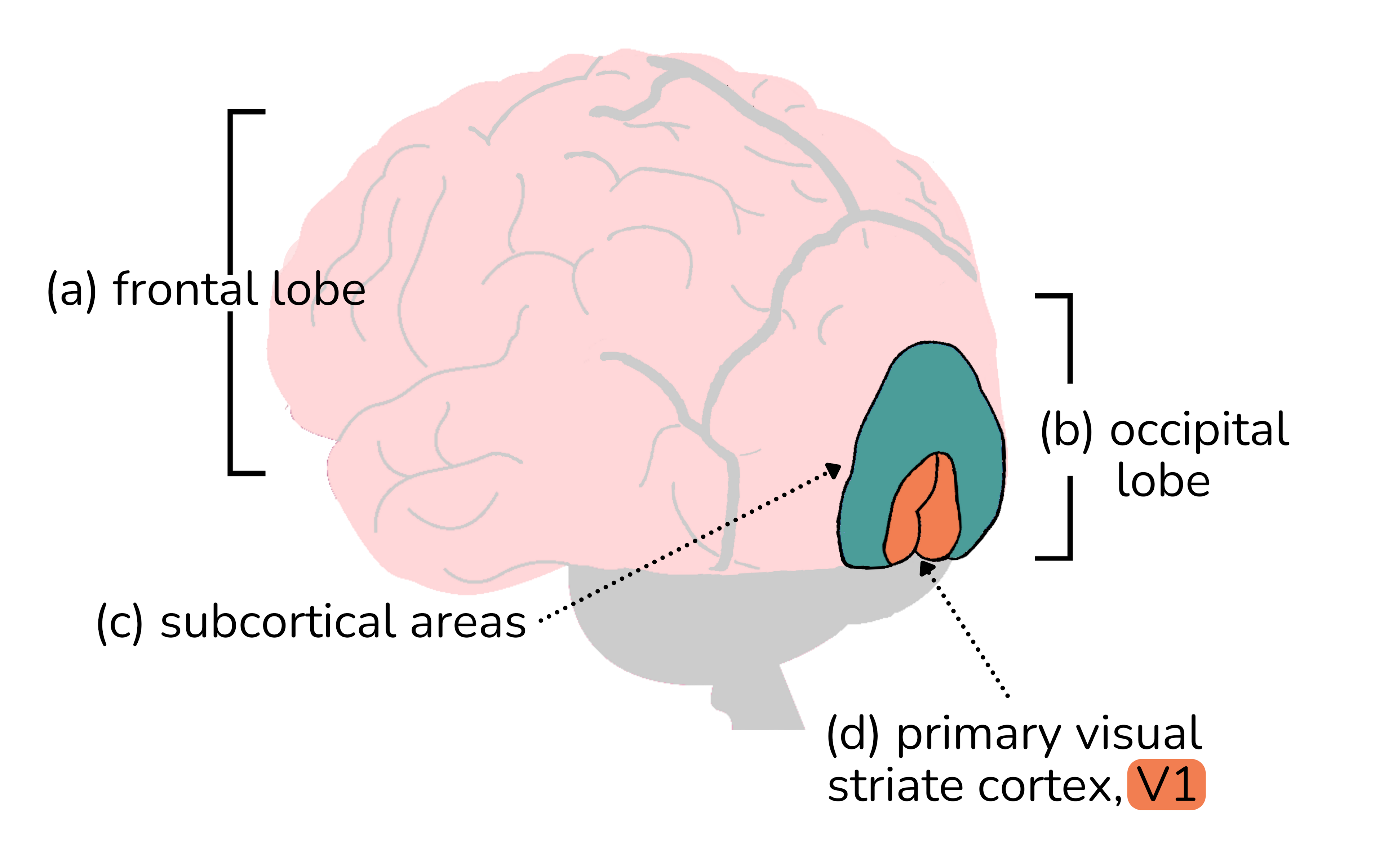
Figure 1: Courtesy of Tyler Mathenia, MD.
Blood supply
The optic tract is supplied by the posterior cerebral artery (PCA), while the optic radiation receives its blood supply from the middle cerebral artery (MCA). The occipital lobe is primarily nourished by the PCA, with a smaller contribution from the MCA.1
Causes and pathophysiology of CVI
Hypoxia, or oxygen deprivation, causes damage to the visual cortex, resulting in CVI. The most common cause of CVI in the pediatric population (22%) is perinatal hypoxia (i.e., impaired blood flow to the placenta, a birth complication).3
Additional causes of CVI include central nervous system (CNS) structure abnormalities, infection, metabolic disorders, chromosomal aberrations, epileptic encephalopathy, traumatic events, and other mixed etiologies.4
- Epilepsy: Notably, epilepsy and epileptic drugs seem to produce specific vision loss; specifically infantile spasms that appear between 3 and 8 months of age, can result in central visual impairment. The exact pathogenesis of visual impairment in patients with infantile spasms is uncertain.2
- Vigabatrin, an antiepileptic drug used in infantile spasms, may cause permanent, concentric peripheral visual field loss due to drug-induced injury to both the retinal photoreceptors and the retinal ganglion cells and their axons.5
- Hydrocephalus: Hydrocephalus leads to chronic distention of the posterior cortex, contributing to cerebral visual impairment. Additionally, secondary elevation of intracranial pressure can exacerbate CVI.
- Hypoxic-ischemic encephalopathy (HIE): CVI resulting from HIE involves damage to the visual processing areas of the brain due to inadequate oxygen supply. Perinatal and postnatal HIE represent the most prevalent cause of CVI.
- Infections: Infections from bacteria, viruses, or parasites are implicated in CVI. Various mechanisms by which infection might harm the brain include thrombophlebitis, arterial occlusion, hypoxic-ischemic damage, venous sinus thrombosis, and hydrocephalus. Examples include TORCH (toxoplasmosis; other [syphilis, rubella, cytomegalovirus, and herpesvirus]) infections.
- Trauma: Direct damage to the visual cortex is another cause of CVI. Trauma can be non-accidental, such as in shaken baby syndrome.
- Other causes of CVI: Brain tumors, cerebrovascular accidents, congenital brain malformations, hemodialysis, hypoglycemia, and metabolic and neurodegenerative disease are other causes of CVI.
Etiology and pathophysiology of CB
Spontaneous ischemic stroke (32%) and cardiac arrest or surgery (20%) are the primary causes of cortical blindness in adults. They represent vascular and perfusion-related issues that impede blood flow, compromising oxygen and nutrients to the visual cortex, and manifesting as cortical blindness.8
The other numerous and diverse causes of CB in adults are summarized below.
Vascular conditions linked with CB
Inadequate vascular supply of blood and nutrients to the occipital lobe is the most common cause of cortical blindness (CB).
Vascular conditions include:
- Bilateral occipital infarction
- Dural venous sinus thrombosis
- Hypoperfusion or hypoxia related to cardiac arrest
- Carbon monoxide poisoning
- Spinal surgery
- Posterior reversible encephalopathy syndrome
- Preeclampsia, eclampsia
- Angiographic contrast agents
Infectious diseases associated with CB
CB resulting from infection is typically due to direct microbial invasion, inflammation, or secondary vascular compromise.
Infectious disorders are:
- Meningitis
- Subacute sclerosing panencephalitis (SSPE)
- Creutzfeldt-Jakob disease (Heidenhain variant)
- COVID-19
- Progressive multifocaI leukoencephalopathy
Metabolic disturbances and cortical blindness
Metabolic imbalances in glucose, electrolytes, or oxygen compromise neuronal function, culminating in CB.
Several metabolic conditions include:
- Hypoglycemia
- Nonketotic hyperglycemia
- Hepatic encephalopathy
- Ornithine transcarbamylase (OTC) deficiency-related hyperammonemic encephalopathy
Mitochondrial conditions linked with CB
In mitochondrial disease, the mitochondria impairs energy production necessary for normal neuronal activity, particularly in the occipital cortex.
Mitochondrial conditions in adults are:
- Mitochondrial encephalopathy (i.e., mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes [MELAS] syndrome)
- Leigh disease
Neurodegenerative diseases associated with CB
In neurodegenerative diseases, the progressive degeneration of brain structures, including the occipital cortex, contributes to cortical blindness through the cumulative impact on visual processing pathways.
Neurodegenerative diseases associated with CB:
- Leukodystrophy
- Alzheimer’s disease (posterior cortical atrophy)
Other factors connected with CB
The other conditions, causes, and pathophysiologies of CB are diverse and numerous and include:
- Seizures and postictal state
- Radiation necrosis or stroke-like migraine attack after radiation therapy (SMART)
- Demyelinating disease (Schilder variant)
- Periventricular leukomalacia
- Electrocution
- Electroconvulsive therapy
- Ozone-induced encephalopathy
Presentation of cortical blindness
The classic presentation of CB is characterized by (1) severe bilateral and symmetric vision loss, (2) little to no anterior and posterior segment findings, (3) fully intact pupillary light reflexes with no relative afferent pupil defect (RAPD), and (4) presence of homonymous hemianopsia visual field defect, which may be partial or complete.1,4,7
The severity of vision loss can range from no light perception to near-normal visual acuity in children and adults.9 Near-normal visual acuity can occur as a result of macular sparing.1
Signs and symptoms of CVI
In pediatric patients with CVI, ocular signs and symptoms may deviate from the classic presentation with the addition of associated neurological conditions.
Ocular findings in CVI include:9
- Exotropia (41%)
- Mild optic atrophy (25%)
- Nystagmus (21%)
- High refractive error (20%, [e.g., hyperopia >+3D and myopia >-2D])
- Esotropia (19%)
CVI is often associated with other neurologic deficits, including epilepsy, cerebral palsy, hemiparesis, microcephaly, and hearing loss.9
Diagnostic testing for cortical blindness
Electrophysiology
Clinical electrophysiological testing incorporates noninvasive procedures that provide an objective indication of function at various locations within the visual system.10 In situations involving unexplained or suspected functional visual loss, normal electrophysiology can effectively exclude organic causes.10
Valuable visual electrophysiology tests employed in diagnosing CB and CVI include electroretinography (ERG) and visually evoked potential (VEP). ERG assesses the functional integrity of the retina to brief flashes of light,10 while VEP measures optic nerve and post-retinal pathway function.
Flash VEPs, which use diffuse flash stimulation, are less sensitive but suit young children, patients with poor fixation, and non-compliant patients.10
Neuroimaging
Neuroimaging is crucial for assessing the location and amount of damage, differentiating optic nerve and cortical involvement, and aiding in the prognosis of visual recovery.7
Computed tomography (CT) offers initial accessibility but may overlook early or small strokes.7 Magnetic resonance imaging (MRI) is superior for diagnosing cerebral infarction, meningitis, encephalitis, and neurodegenerative disorders, with diffusion-weighted MRI pinpointing acute infarction areas.7
Optokinetic nystagmus testing
Optokinetic nystagmus (OKN) is an involuntary eye movement in response to moving visual stimuli, like stripes on an optokinetic drum. The OKN response estimates visual and neurological functions and can be abnormal or missing in patients with CB/CVI.11,12
It has been shown that OKN can be generated in patients with CB and CVI due to subcortical mechanisms or extrastriate pathways.11,12 The unreliability of OKN testing makes it best suited as a quick and adjunctive tool when neuroimaging equipment is not available.
Visual acuity testing
As mentioned earlier, patients often present with bilateral symmetric vision loss that can range from almost normal visual acuity in cases of macular sparing, and extend to finger counting, hand motion, or no light perception.1,9
Visual field testing
Visual field testing should be performed whenever possible. Visual field defects can be correlated with findings regarding location, damage, and amount of vision loss. Lesions in different areas of V1 correspond to different types of visual field defects.12
For example, anterior cortex lesions, typically from PCA stroke, cause contralateral congruous homonymous hemianopia with macular sparing. This occurs because blood to the occipital cortex tip is supplied by the unaffected MCA in PCA stroke.1
Figure 2 presents a cross-sectional diagram of the V1 area, whereas Figure 3 represents the corresponding visual field defects.12,13

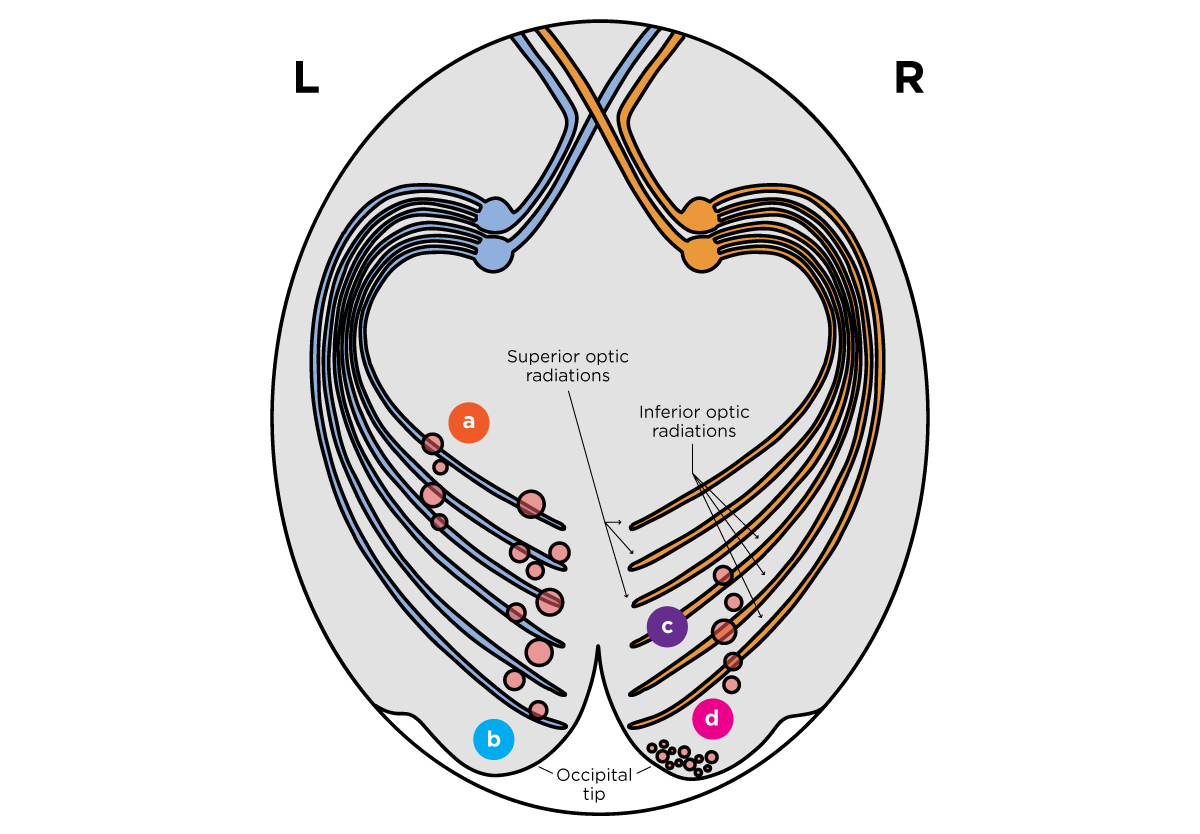
Figure 2: Courtesy of Cindy Hui, OD.

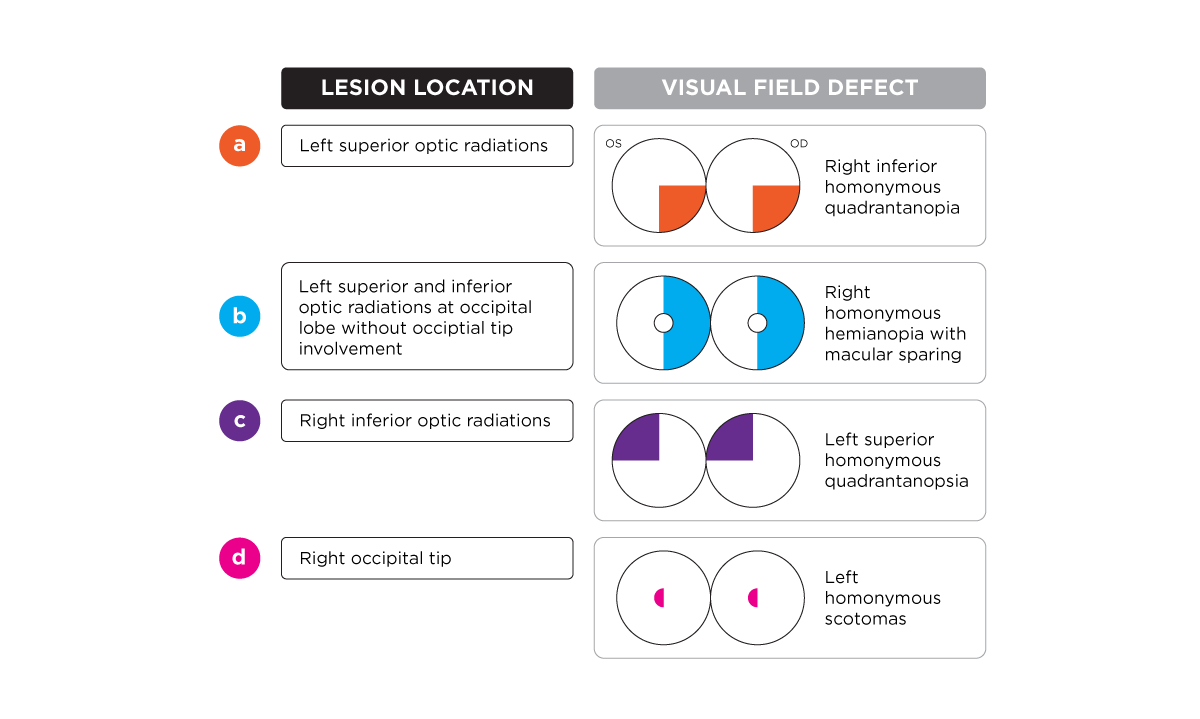
Figure 3: Courtesy of Cindy Hui, OD.
Differential diagnoses for cortical blindness
Ocular conditions that produce symmetrically reduced vision in both eyes, normal pupillary reflexes, and unremarkable anterior and posterior segment findings should be considered in the differential diagnosis of cortical blindness.3
Ocular disorders
Bilateral retrobulbar optic neuritis
Bilateral retrobulbar optic neuritis, can present with central and peripheral vision loss with a normal fundus appearance.3 Distinguishing features include sluggish pupils, color vision impairment, and eye pain with movement.15
Genetically-determined retinal photoreceptor degeneration
Genetically-determined retinal photoreceptor degeneration, like foveal cone dystrophy, is characterized by central vision loss with color vision abnormalities. Abnormal ERG findings occur due to impairment of the foveal cone cells.16
Glaucoma and retinitis pigmentosa
Glaucoma and retinitis pigmentosa (RP) exhibit peripheral visual field loss, with possible macular sparing. Unlike cortical blindness from bilateral PCA infarctions, they lack bilateral homonymous hemianopias.3
Leber congenital amaurosis
Infants with retinal degenerations, such as Leber congenital amaurosis (LCA), present with nystagmus, sluggish or absent pupillary responses, severely decreased visual acuity, photophobia, and high hyperopia. Diagnosis of LCA relies on severely subnormal or non-detectable ERGs, optical coherence tomography (OCT), and genetic testing.17
Leber hereditary optic neuropathy (LHON)
Leber hereditary optic neuropathy (LHON) presents with vision and color loss, featuring a cecocentral scotoma. A pupillary defect may only appear in the acute stage.18
Ocular migraines
Migraines, including ocular migraines, may simulate cortical blindness by causing restricted visual fields or tunnel vision during an episode.19 With ocular migraines, visual field changes are temporary and variable, lasting for up to 30 minutes.
Oculomotor apraxia
Young children with oculomotor apraxia (OMA) often get misdiagnosed as blind due to an inability to orient their eyes to visual targets. Symptoms include difficulty fixating, head thrusting, and abnormal OKN.20
Paraneoplastic retinopathies
Paraneoplastic retinopathies, such as cancer-associated retinopathy (CAR), may cause mild pupillary light reflex reduction, severe vision loss, ring scotoma, and other visual field defects with minimal fundus abnormalities. Retinal and optic nerve autoantibody testing and ERG are starting points in the diagnosis of CAR.21
Non-organic disorders with similar presentations to CB
Non-organic disorders that produce symmetrically reduced vision in both eyes, normal pupillary reflexes, and unremarkable anterior and posterior segment findings should be considered in the differential diagnosis of cortical blindness.
Non-organic disorders that can mimic cortical blindness include hemineglect, malingering, prosopagnosia, and simultagnosia.1
- Hemineglect: Hemineglect and CB share similarities in impaired awareness, both resulting from brain damage, affecting perception or attention. Hemineglect is associated with damage to the parietal lobe, not at V1.
- Malingering: Malingering is a conscious and intentional exaggeration or feigning of physical or psychological symptoms. Objective testing for OKN and VEP can be helpful. Visual field testing can generate unusual outcomes.
- Prosopagnosia: Prosopagnosia is a neurological condition characterized by the inability to recognize faces. It often results from damage to the fusiform gyrus, a region in the temporal lobe of the brain associated with face recognition.
- Simultagnosia: Simultagnosia is a neurological condition characterized by the inability to perceive a visual scene as a whole, only able to process one object at a time. Patients will often have homonymous or juxtaposed homonymous visual field deficits due to bilateral parieto-occipital damage.
Treatment and management of CB
Pediatric treatment of CVI
A significant proportion of children with CVI experience improvement in visual function with therapy. A review by Matsuba et al. evaluated the long-term outcome of children with congenital CVI and found that 46% of the children had at least one level of visual improvement, compared to 8% of children who experienced visual decline.26
Treatment of concomitant ocular/visual disorders
Any concomitant visual disorders should be corrected, including underlying refractive error, strabismus, and amblyopia. Likewise, ocular disorders such as congenital cataract or retinal disease should be treated.5
Vision therapy for pediatric patients with CVI
Vision therapy for children with CVI consists of exercises and training to improve (1) visual awareness and attention, (2) visual perception, (3) scanning and tracking, and (4) hand-eye coordination.27
Adult treatment of cortical blindness
Substitution therapy
Substitutive interventions feature adapted lighting, environmental modification, and prism therapy to support activities of daily living (ADLs). Adapted lighting entails optimizing the position and brightness to maximize residual vision. Environmental modification improves contrast by minimizing patterns, such as removing heavily patterned rugs.
Visual substitution therapy with prisms shifts images from damaged portions of the retina projecting to the intact visual cortex, enabling patients to capture visual information that would otherwise be missed.28
Compensation therapy
Compensation therapy, similar to visual substitution therapy without prisms, trains patients in deliberate head and eye movements to (1) increase saccades toward the impaired visual field, (2) vary saccade amplitude for increased sampling efficiency, and (3) develop organized scanning patterns in areas of their visual field defect.28
Restitution
The purpose of visual restitutive interventions is to restore vision and reduce visual field defect size by training impaired functions or repeatedly stimulating areas of the visual field.
Visual restoration approaches usually employ computer-based vision training that provides repeated exposure to target stimuli to activate the brain and restore vision.28
Brain stimulation
Visual training could potentially be enhanced with noninvasive electric brain stimulation, with various strategies currently under investigation as potential adjuvants to training. These include transcranial random noise stimulation (tRNS), transcranial direct current stimulation (tDCS), and repeated transorbital alternating current stimulation (rtACS).28
Pharmacotherapy
The use of pharmacology in vision recovery post-stroke is under research, with several studies suggesting that serotonin reuptake inhibitors could enhance plasticity in the adult visual system. The mechanism works by reopening a critical period to facilitate recovery and prolonging the transient phase of increased plasticity post-stroke.28
Co-management of CB and CVI
Educating patients
Educating patients and their families about their condition, government programs, low vision services, and special education services available to them is imperative for ongoing care. Coordinating with social services empowers patients and families to take full advantage of available opportunities and support.27
Many low vision clinics offer a full spectrum of rehabilitation services as well. These include training on orientation and mobility, independent living skills, assistive technology, and reading/writing with braille.
Preventing perinatal hypoxic-ischemic encephalopathy and preterm delivery is the optimum technique for limiting vision loss from CVI.2 Patient education and promoting compliance with specialists in the patient’s medical team can circumvent adverse effects.
Collaborative care to treat CB and CVI
Children with CVI commonly have co-morbidities like cerebral palsy, developmental delay, and autism spectrum disorder (ASD). Partnering with pediatricians and/or child psychologists to treat these conditions is significant as systemic improvements may also influence and benefit a patient’s visual outcome.5
Part of managing patients requires integrating care with the patient’s neurovascular medical team to treat the underlying condition of CB and prevent future ischemic events, such as in cases of cerebral infarction.3
Additionally, sleep disturbances are common in patients with severe CB, likely resulting from a loss of the circadian rhythm controlled by light. These sleep disturbances can manifest as restlessness, wandering, mood swings, agitation, and akathisia (the inability to sit still).
Co-management with neurologists or psychiatrists can help restore sleep cycles and manage other psychological concerns in patients with CB.29
Conclusion
While this article simplifies the topic of CB, the true challenge lies in managing CB patients with severe vision loss.
This emphasizes the importance of eyecare providers engaging in collaborative care with neurologists, psychologists, and rehabilitation specialists for optimal outcomes in dealing with cortical blindness and cortical visual impairment.
