


Optical coherence tomography (OCT) is a non-contact imaging technology that produces high-resolution cross-sectional images of ocular tissues.1,2 First introduced in 1994 and commercially available in 2001, anterior segment OCT (AS-OCT) enables precise visualization of the anterior segment structures and can therefore be utilized in various corneal, anterior segment, and ocular surface diseases.1-6
It is important to note that the cross-sectional imaging capability of AS-OCT is similar to ultrasound biomicroscopy (UBM); however, AS-OCT is non-contact and minimizes patient discomfort and image distortion.1-8 OCT also offers the benefit of higher resolution than UBM, for a more detailed analysis of anatomic structures.1-8
There are two OCT platforms available: Time-Domain (TD-OCT) and Spectral-Domain (SD-OCT).1,2
TD-OCT produces cross-sectional images by varying the position of a reference mirror; it allows for deep penetration through the sclera and limbus with 15-20µm resolution.1,2 It also offers a broader range of image capture. Two platforms that utilize TD-OCT are Visante (Carl Zeiss Meditec, Jena, Germany) and Heidelberg (Heidelberg Engineering, GmBH, Smithfield RI).1,2
SD-OCT (also known as Fourier-domain OCT ) uses a spectrometer to detect an image signal by varying the wavelength of light source with time; the interference between the reference reflection and sample is detected as a spectrum. SD-OCT has a more rapid image acquisition but a shorter horizontal scan width compared to TD-OCT.1,2 Examples of platforms that use SD-OCT are Spectralis (Heidelberg Engineering, GmBH, Smithfield RI), RTVue (Optovue, Inc, Fremont CA), and Cirrus (Carl Zeiss Meditec, Jena, Germany).1,2
Additionally, there is ultrahigh-resolution OCT available, which can have an axial resolution of 1-4µm.1,2 This may be more useful in differentiating between various corneal and ocular surface pathologies (e.g., ocular surface neoplasia vs. pterygium vs. ocular surface lymphoma).1-7
Anterior Segment OCT Diagnostics
Diagnosis of corneal and anterior segment disease
AS-OCT can provide cross-sectional imaging of the cornea, conjunctiva, and anterior chamber angle. This proves useful in diagnosing and delineating details in specific ocular surface and anterior segment conditions.
Conjunctivochalasis: AS-OCT can measure a cross-sectional area of the conjunctiva prolapsing into the tear meniscus.1-7 It can also evaluate the ocular surface post-treatment.1-7
Figure 1 demonstrate clinical images of conjunctivochalasis before (left) and after (right) repair.

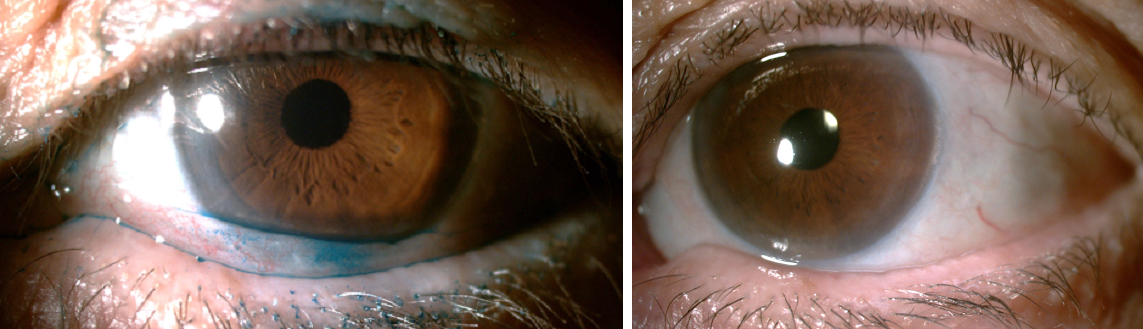
Figure 1
Pterygium/Pingueculum: While pterygium and pinguecula are usually easily identified on clinical examination, SD-OCT can highlight subepithelial hyper-reflective wedge-shaped areas within the overlying epithelium.1-7 Ultra-high resolution OCT will also show a dense hyper-reflective subepithelial lesion; this may be more useful in identifying an early recurrence of pterygium post-surgery.1-7
Conjunctival lymphoma: Conjunctival lymphoma constitutes 1.5% of conjunctival tumors.8,9 It is a tumor of the ocular surface that usually presents as a painless, salmon-pink, fleshy area.8 It may appear to have a smooth or nodular surface and is often associated with minimal symptoms, leading to a delay in diagnosis.9 Use of AS-OCT here, which identifies a hyporeflective subepithelial lesion with a thin, slightly hyperreflective layer, may add to the diagnosis.1-9 It is vital to prevent delayed diagnosis (as well as subsequent biopsy and treatment), as systemic workup may be necessary.1-7,9 Treatment may consist of radiation, localized chemotherapy, in conjunction with excisional biopsy.9
Ocular surface squamous neoplasia (OSSN): Here, AS-OCT displays hyperreflective, thickened epithelium with an abrupt transition from normal to abnormal.1-7 Ultra-high resolution OCT can also be used to monitor treatment response and normalization of epithelial appearance.1-7 While most cases of OSSN can be differentiated from benign growths like pterygium, AS-OCT does confirm abnormal anatomy.
A clinical example of ocular surface squamous neoplasia (OSSN) is shown in Figure 2.

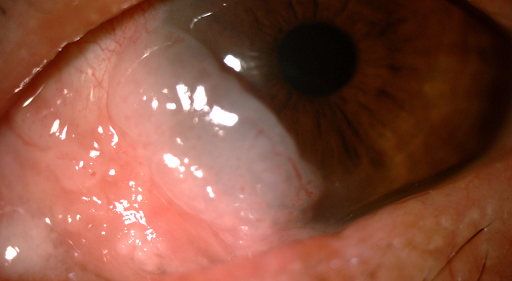
Figure 2
Melanoma/Nevi: Here, SD-OCT displays epithelial hyperreflectivity, most intense within the basal layer and less so throughout the epithelium.1-7 Ultra-high resolution OCT shows normal-to-slightly thickened overlying epithelium with variable hyperreflectivity.1-7 Intralesional cystic spaces may be present in conjunctival nevi, whereas melanoma often demonstrates intense shadowing of sub-lesional tissue on OCT.1-7
Salzmann nodular degeneration: AS-OCT may help in the diagnosis of Salzmann nodular degeneration, as well as differentiation from other ocular diagnoses.1-7 OCT here may show a dense, hyperreflective subepithelial lesion overlying Bowman’s layer with normal surrounding epithelium.1-7
Iris/Ciliary body tumors: It is important to note that UBM may be superior in comparison to AS-OCT in identifying the extent of anterior segment intraocular tumors.1-7 However, SD-OCT may be a more reliable alternative for small/less-densely pigmented anterior iris tumors, especially when cyst-like in nature.1-7
Treatment planning: OCT may provide pachymetry measurements and a physical picture of corneal thickness/irregularities that can help plan for procedures such as phototherapeutic keratectomy (PTK).1-7 This is especially helpful when PTK is being used as a modality to treat corneal haze, scarring, and superficial corneal dystrophies.1-7
Microbial keratitis: In cases of severe keratitis/corneal ulceration, OCT may serve as an adjunct modality to help determine response to treatment and the possible need for more urgent surgical intervention (e.g., severe corneal thinning, impending perforation).1-7 Here, AS-OCT may show keratitis as a hyperreflective area in the stroma.1-7
Keratoconus/ectasia: While topography and tomography are considered the standard for diagnosis in keratoconus and ectasia, AS-OCT can provide helpful information regarding the state of the epithelium (usually thickened over the cone), as well as an anterior hyper-reflective area at Bowman’s layer, which can be associated with increased risk of hydrops.1-6,10 AS-OCT can also help focally measure pachymetry in the presence of corneal scarring.1-6,10
Anterior segment trauma: In the case of anterior segment injury needing surgery, AS-OCT is an optimal imaging method as it is non-contact and high resolution in nature, allowing for evaluating injury depth and extent.1-7 AS-OCT can also be used to follow clinical progress post-treatment and look for signs of scarring, epithelial downgrowth, and retained foreign matter in the anterior segment, which may be missed on slit-lamp examination.1-7
Angle configuration: AS-OCT can be used to determine the anterior chamber angle configuration, which is especially useful before and after performing laser peripheral iridotomy. 1-7
Figure 3 is an example of AS-OCT showing a moderately open anterior chamber angle.

Figure 3
In contrast, Figure 4, demonstrates a very narrow angle.1-7 The other benefit that it offers is that the image obtained by AS-OCT vs. gonioscopy is objective—even the best glaucoma specialists may sometimes disagree on subjective angle configuration! It can also show the progression of cases of phacomorphic glaucoma and guide when cataract surgery may be indicated earlier rather than later.1-7


Figure 4:
Cataract surgery planning: AS-OCT can be used for intraocular lens (IOL) calculation, evaluation of lens thickness, anterior chamber depth, and angle structures which are critical aspects in assessing a patient for cataract surgery.1-7,10-12
Intraoperative Anterior Segment OCT
Cataract: Intraoperative AS-OCT can help evaluate wound architecture (especially in complex cases—think, post-corneal transplant, post-LASIK, post-trauma eyes).1-7,11,12 AS-OCT can be used in femtosecond laser-assisted cataract surgery (FLACS) to map corneal astigmatic incisions, sites of wound creation (paracentesis and primary wound), capsulotomy, and lens fragmentation.1-7,11-13 AS-OCT can also be employed to measure lens thickness intraoperatively (in the case of a posterior polar cataract), IOL position (perhaps if there is tilt due to weak zonules), and wound gape at the end of the case.1-7,11-13
Cornea: AS-OCT is especially valuable in lamellar corneal transplantation.1-6,10,14-16 For deep anterior lamellar keratoplasty (DALK), AS-OCT can help surgeons in the challenging steps of the surgery to achieve optimal Descemet’s membrane dissection.1-6,10,14-16 For endothelial keratoplasty (DSAEK, DMEK), AS-OCT can ensure the anterior chamber is not overly crowded and decrease risk of pupillary block (more for DSAEK versus DMEK).1-6,10,14-16 AS-OCT can also help detect cases of partial graft attachment vs. full attachment, as well as fluid in the graft-host interface.1-6,10,14-16
Identifying these issues intraoperatively can be beneficial, especially since the patient is still under anesthesia, rather than performing a re-bubbling procedure postoperatively in the office.1-6,10,14-16
In patients who undergo keratoprosthesis placement (KPRO), it is well known that there is no standardized method for evaluation of the implanted KPRO and adjacent tissues.1-6,10,14-16 Due to limited visualization, it may be difficult to identify serious complications such as a retroprosthetic membrane, wound gape, and angle-closure.1-6,10,14-16 Fortunately, AS-OCT can detect the presence of a retrokeratoprosthetic membrane, gape in the wound interface (should not be missed!).1-6,10,14-16
AS-OCT is used for refractive (e.g., LASIK) surgery. It enables precise measurement of LASIK flap thickness and residual stromal bed thickness evaluation before planned enhancement surgeries.1-6,10,14-16 It is also utilized to evaluate precise corneal depth before placement of intracorneal ring segments (e.g., INTACS) to avoid complications, including epithelial-stromal breakdown or corneal perforation.1-6,10,14-16
Postoperative use of anterior segment OCT
Cataract: AS-OCT is not commonly used for postoperative cataract patients; however, it may help identify anterior segment pathology in cases of persistent corneal edema when not evident on slit-lamp exam.1-8,11-13 For example, a small but persistent Descemet’s membrane detachment may lead to chronic corneal edema that may be difficult to see on examination. If AS-OCT can delineate the extent of Descemet’s detachment, it can help the surgeon form a treatment or referral plan to a corneal specialist.
Cornea: AS-OCT can help identify fluid in the LASIK flap interface and the presence and extent of epithelial ingrowth.1-6,8,10,14-16 It can also be used in keratoconus patients (post-crosslinking) to determine the demarcation line that indicates the transition zone between the treated and untreated stromal tissue to measure the depth of the line.1-6,8,10,14-16
AS-OCT is also valuable in cases of lamellar keratoplasty in the postoperative period. It may help identify early issues of endothelial graft dislocation or detachment.1-6,8,10,14-16 This can help guide early treatment and increase the success rate for visual recovery post-transplant.
Conclusions
Imaging diagnostics continue to evolve in ophthalmology. AS-OCT has proven extraordinarily valuable in a myriad of pre-peri-and-post-operative circumstances surrounding anterior segment surgery. It is also essential for residents and fellows in training to be aware of the strengths of this imaging modality, as it can help learn more about nuances in surgical technique and subsequent results, in addition to extensive anatomic evaluation.
References
- Han SB, Liu Y, Noriega KM, Mehta JS. Applications of Anterior Segment Optical Coherence Tomography in Cornea and Ocular Surface Diseases. J Ophthalmol. 2016;2016: 4971572
- Ramos J.L.B., Li Y, Huang D. Clinical and research applications of anterior segment optical coherence tomography—a review. Clinical and Experimental Ophthalmology. 2009;37(1): 81-89
- Doors M, Berendschot T.T.J.M., de Brabander J, Webers C.A.B., Nuijts R.M.M.A. Value of optical coherence tomography for anterior segment surgery. Journal of Cataract and Refractive Surgery. 2010; 36(7): 1213-1229
- Shousha M.A., Karp C.L., Canto A.P., et al. Diagnosis of ocular surface lesions using ultra-high-resolution optical coherence tomography. Ophthalmology. 2013;120(5):883-891
- Nanji A.A., Sayyad F.E., Galor A., Dubovy S. Karp C. L. High-resolution optical coherence tomography as an adjunctive tool in the diagnosis of corneal and conjunctival pathology. Ocular Surface. 2015; 13(3): 226-235
- Fuentes E, Sandali O, El Sanharawi M, et al. Anatomyic predictive factors of acute corneal hydrops in keratoconus: an optical coherence tomography study. Ophthalmology. 2015;122(8): 1653-1659
- Ryan D.S., Sia R.K. Coyler M., et al. Anterior segment imaging in combat ocular trauma. Journal of Ophthalmology. 2013;2013:8
- Kent C. Anterior Segment OCT: Still Evolving. Review of Ophthalmology. December 2020
- Han SB, Liu Y, Noriega KM, Mehta J. Applications of Anterior Segment Optical Coherence Tomography in Cornea and Ocular Surface Diseases. Journal of Ophhtalmology. 2016. https://doi.org/10.1155/2016/4971572
- Rocha K.M., Perez-Staziota C.E., Stulting R.D., Randleman J.B. Epithelial and stromal remodeling after corneal collagen cross-linking evaluated by spectral-domain OCT. Journal of Refractive Surgery. 2014; 30(2): 122-127.
- Nguyen P, Chopra V. Applications of optical coherence tomography in cataract surgery. Current Opinion in Ophthalmology. 2013; 24(1): 47-52
- Das S, Kummelil M.K., Kharbanda V, et al. Microscope integrated intraoperative spectral domain optical coherence tomography for cataract surgery: uses and applications. Current Eye Research. 2016; 41(5): 643-652
- Zhang Q, Jin W, Wang Q. Repeatability, reproducibility, and agreement of central anterior chamber depth measurements in pseudophakic and phakic eyes: optical coherence tomography versus ultrasound biomicroscopy. Journal of Cataract and Refractive Surgery. 2010; 36(6): 941-946
- Scorcia V, Busin M, Lucisano A, Beltz J, Carta A, Scorca G. Anterior segment optical coherence tomography-guided big-bubble technique. Ophthalmology. 2013; 120(3) 471-476
- Yeh R-Y, Quilendrino R, Musa F.U.,Liarakos V.S., Dapena I, Melles G.R.J. Predictive value of optical coherence tomography in graft attachment after descemet’s membrane endothelial keratoplasty. Ophthalmology. 2013; 120(2): 240-245
- Garcia J.P.S. Jr., De La Cruz J, Rosen R.B., Buxton D. F. Imaging implanted keratoprostheses with anterior-segment optical coherence tomography and ultrasound biomicroscopy. Cornea. 2008; 27(2): 180-188
