


Macular degeneration (AMD) is one of the main causes of central vision loss in the developed world and affects approximately 25% of people above age 75. This debilitating ocular disease appears clinically in one of two presentations, either dry or wet forms. Wet AMD, also known as “exudative” or “neovascular” AMD, is significantly more sight-threatening than the dry, non-exudative form.
Advanced AMD affects approximately 2 million Americans. Advanced AMD occurs when dry AMD progresses to geographic atrophy (GA) or when wet AMD leaves a disciform scar after the presence of prolonged choroidal neovascular membrane (CNVM).
The easiest way for patients to understand the disease process of macular degeneration is by explaining the compromised exchange of nutrients and waste products within the eye. Numerous mechanisms are proposed in the clinical manifestation of AMD. In general, AMD occurs when the retina/retinal pigment epithelium’s (RPE) ability to metabolize waste products is compromised. It can also occur when the choriocapillaris is unable to adequately deliver nutrients to (or adequately remove waste products from) the retina.
The progression of AMD can be variable, depending on the patient’s age, systemic/lifestyle risk factors, and family ocular history. Age is the greatest risk factor for developing AMD, followed by Caucasian race and history of past/present smoking. A positive family history also increases patients’ risk for developing AMD.
Several emerging therapies are making headway in addressing the unmet need of more durable suppression of this sight-threatening disease. Over the past decade, anti-vasoendothelial growth factor agents (anti-VEGF) have dramatically transformed the treatment approach to macular degeneration, particularly wet AMD.
I thought it would be interesting to write an update on what we have to look forward to in the management of Wet AMD. I love to tell my patients about these upcoming advancements on the horizon, keeping them excited for the future and letting them know they are not destined to see me every four-to-six weeks for the rest of their lives!
Pathogenesis of macular degeneration
The etiology and pathogenesis of macular degeneration is multifaceted and thought to occur via several mechanisms. Regardless of AMD presentation, the retinal pigment epithelium (RPE) and choriocapillaris are greatly compromised. Through various age-related retinal changes, the RPE’s ability to maintain photoreceptor cells is slowly diminished.
The “sick RPE” theory proposes that the RPE layer is unable to fully metabolize photoreceptor waste products. This occurs by the altered permeability and degeneration of RPE/Bruch’s complex, leading to the formation of subretinal drusen deposits, pigment epithelial detachments, CNVM, and eventual geographic/outer retinal atrophy.

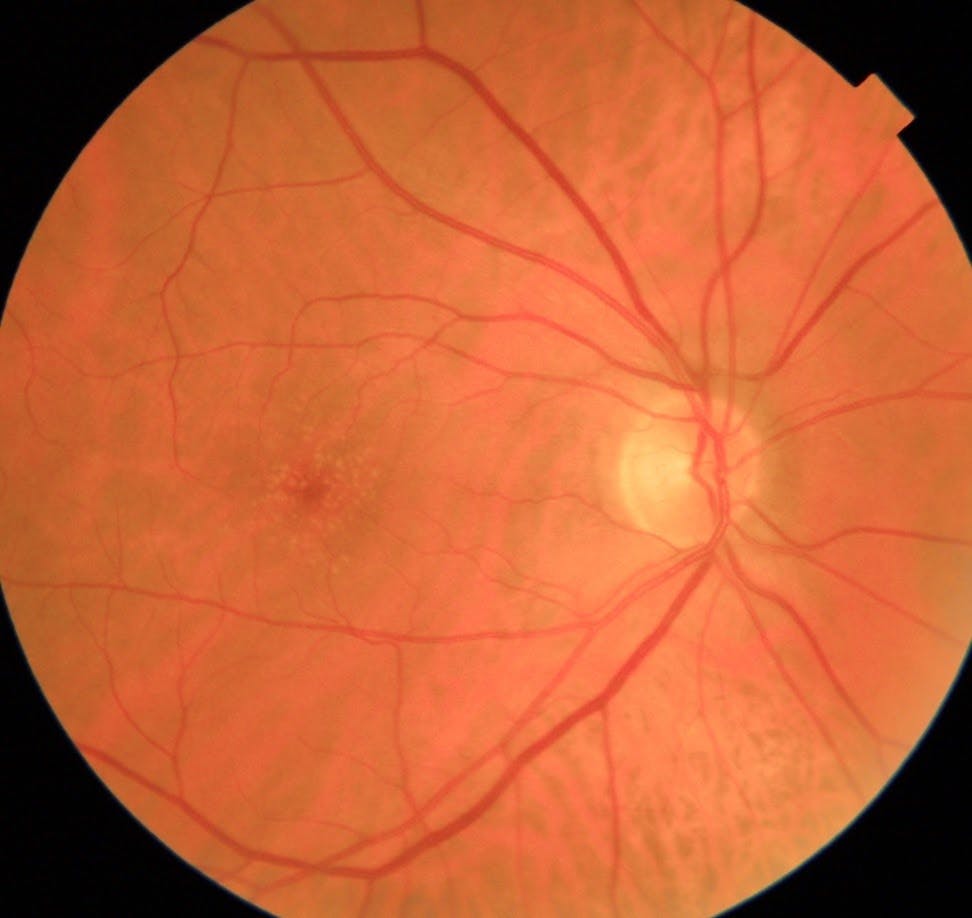
Figure 1: Fundus photo showing small/medium sized drusen deposits in intermediate dry AMD. Large drusen are defined as > 125 micrometers in size (diameter of central retinal vein) Photo courtesy of Kevin Cornwell, OD

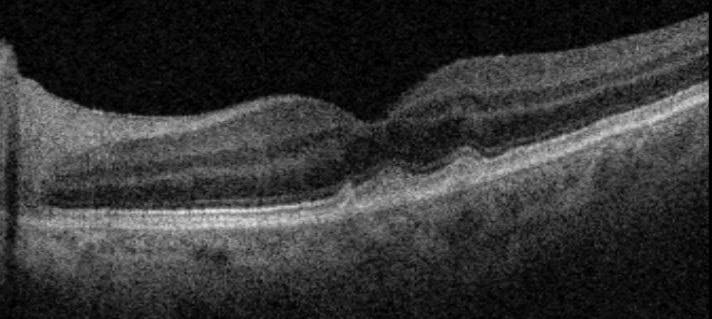
Figure 2: OCT scan showing subretinal soft drusen deposits in dry AMD. Photo courtesy of Kevin Cornwell, OD
The “vascular ischemic” theory proposes insufficient nutrient delivery and poor RPE waste removal via an atrophic/atherosclerotic choriocapillaris. It has been shown that patients with AMD have a thinner, more atrophied choriocapillaris layer.
Inflammation and oxidative stress have also been shown to be involved in the pathogenesis of AMD. Various components of the complement cascade have been found within drusen deposits. This may partly explain why smokers, who are prone to more inflammation, develop AMD at higher rates. Some genetically susceptible patients have also been shown to have increased choroidal C-reactive protein levels, which may link genetics and inflammatory etiology in AMD.
The compromised RPE can eventually lead to the upregulation of VEGF. This pro-angiogenic state occurs within the retina and new blood vessels break through an already compromised RPE/Bruch’s complex to form a CNVM. Similar to weeds growing up through cracks in a driveway, the formation of CNVM is the hallmark of wet AMD. The end result of uncontrolled CNVM is usually a disciform scar that results in irreversible loss of central acuity for the patient.

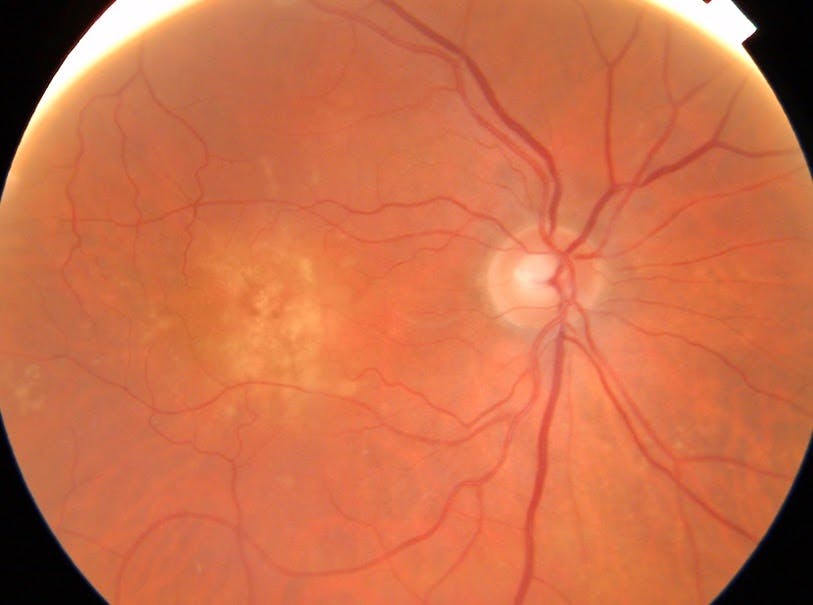
Figure 3: Fundus photo showing early CNVM in wet AMD. Formation of CNVM will initially appear grayish/green, and progresses to appear more red in color during later stages. Photo courtesy of Kevin Cornwell, OD
Dry vs. wet macular degeneration
Regardless of what form of AMD a patient has, they are at a significantly higher risk for irreversible vision loss, and require close monitoring. Patients presenting with dry AMD will initially have mild RPE disruption within their macula, often classified as “pigment mottling” or “pigment granulation.” The RPE will typically have areas of coalesced hyper and/or hypopigmentary changes. Dry AMD typically progresses to form small “hard” drusen deposits, or larger “soft” drusen deposits, all of which consist of photoreceptor waste material.
Numerous AMD grading scales exist to help clinicians determine disease severity and necessary treatment protocols. The American Academy of Ophthalmology has adopted the AREDS grading scale in the clinical classification of AMD severity.
The presence of numerous small/medium hard drusen (<125 micrometers in size) typically indicates early AMD classification (AREDS category 2). Multiple soft drusen, typically greater in size (>125 micrometers), are generally indicative of intermediate dry AMD stages (AREDS category 3). The presence of CNVM and/or any fovea-involving geographic atrophy places the patient at advanced/late stage disease (AREDS category 4).
Of the patients with dry AMD, up to 20% will convert to the wet form. Dry AMD is typically treated with patient education (eg. smoking cessation counseling and use of home amsler grid) and nutritional supplementation (e.g., AREDS/Preservision vitamins, increased dietary intake of lutein/zeaxanthin and omega 3 fatty acids).
The wet form of AMD is more sight-threatening. Approximately 10% of all AMD cases occur in the wet form and require aggressive management with anti-VEGF therapy. Unfortunately, patients with wet AMD can still progress and lose central vision, despite standard-of-care treatment and close monitoring. This occurs when the CNVM partially “resolves”, leaving a disciform macular scar in its place.

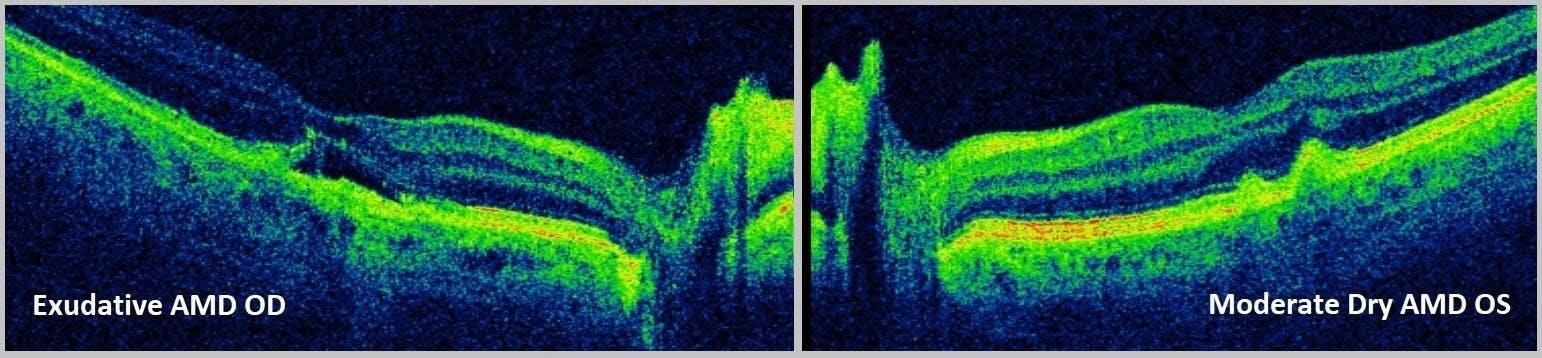
Figure 4: OCT scan showing exudative (wet) vs. dry AMD. Photo courtesy of Kevin Cornwell, OD
Making a diagnosis
Depending on the extent of progression, diagnosis of wet AMD may be highly suspected on clinical exam alone. The implementation of other diagnostic tools, however, is crucial in the diagnosis and management of AMD, both wet and dry forms. The gold standard for diagnosis of suspected CNVM in wet AMD is fluorescein angiography (FA). The CNVM pattern (classic vs. occult), lesion borders, and location can be fully assessed with FA. Treatment protocols are also determined and/or modified based on FA results.
Other imaging modalities in AMD management include spectral domain optical coherence tomography (SD-OCT), indocyanine green angiography (ICGA), and fundus autofluorescence (FAF).
One of the latest, non-dye based, diagnostic technologies in wet AMD management is OCT angiography (OCT-A). While OCT-A will not replace FA at present, it is a non-invasive, less time consuming adjunct to FA testing. Images taken via OCT-A have also been shown to have high diagnostic accuracy when compared to former imaging modalities in the management of exudative AMD (eg. fluorescein angiography).
OCT-A uses cross sectional B-scans to detect erythrocyte motion and create detailed images of the retinal microvasculature and choroidal vessels. It may also provide superior imaging of the foveal avascular zone (FAZ) as compared to conventional FA.
OCT-A can be a useful alternative for patients at risk for potential systemic side effects or contraindications to fluorescein dye. Several disadvantages to OCT-A imaging include restricted fields of view and the higher likelihood of image artifacts, when compared to FA. By nature, OCT-A produces a static image, whereas FA reveals a more dynamic story. From a medical billing perspective, there also currently lacks additional CPT codes beyond standard OCT imaging for reimbursement purposes.
Wet AMD treatment: past, present, and future
The primary goal of wet AMD treatment is to target and stop CNVM formation. The intravitreal injection of anti-VEGF agents has undoubtedly transformed the treatment approach to wet macular degeneration. Since the early 2000’s, anti-VEGF therapy has slowly developed to become today’s first-line treatment for wet AMD. Ranibizumab (Lucentis), bevacizumab (Avastin), and aflibercept (Eylea) are the most commonly used agents today. Eylea is one of our current kings in wet AMD care.
Other treatment modalities, including intravitreal steroids, photodynamic therapy (PDT) and laser photocoagulation, have also been used in the past in cases with poor treatment responses.
Typically, wet AMD patients are started on a monthly/bimonthly treatment protocol using intravitreal anti-VEGF agents. Once the disease process shows stability and comes to a halt, it is common for the patient to be switched to a “treat and extend” protocol. This progressively extends the periods between each follow up visit and reduces the logistical burden of treatment on the patient. This approach is more cost-effective and has been shown to have similar outcomes on final visual acuity for the patient with wet AMD.
New research in wet AMD treatment
Despite current treatment options, there remains an unmet need for more durable, prolonged suppression of this sight-threatening disease. While none of our current wet AMD treatment options will cure the disease or reverse its destructive course, there are myriad new, more robust treatments on the horizon.
The following list introduces several new, promising treatment modalities that may significantly alter the standard-of-care in wet AMD treatment while also greatly improving visual outcomes.
Brolucizumab
Brolucizumab is a tiny humanized single-chain antibody fragment and a potent VEGF inhibitor. The small size allows higher dosing per volume, which may result in a longer-lasting effect. Two large phase 3 trials, HAWK and HARRIER, investigated the efficacy and safety of brolucizumab and demonstrated noninferiority of brolucizumab to aflibercept. Moreover, over 50% of patients were maintained on a quarterly dosing schedule, promising fewer injections for our patients.
Port Delivery System
Genentech is developing a surgically implanted drug delivery system, the Port Delivery System (PDS) for use with ranibizumab (Lucentis, Genentech). This surgically-implanted reservoir promises to slowly release the drug over time, and in the phase 2 LADDER trial 80% of patients who received the highest dose did not require refills for at least 6 months. At the end of the 9-month study period, patients treated with the PDS showed similar anatomic and visual outcomes equivalent to those treated with monthly anti-VEGF injections. Treatment innovations such as the implantable PDS may significantly reduce the financial and logistical burden of wet AMD treatment on the healthcare system and patient respectively.
Faricimab
Simultaneous with developing the PDS, Genentech is also developing a novel drug, faricimab. This is a highly-engineered bispecific antibody that suppresses both VEGF similar to all current drugs as well as angiopoietin 2 (Ang-2), which is also important in vascular development and stabilization. It is thought that a dual blockade of VEGF and Ang-2 may bring synergistic effects in the treatment of wet AMD. The phase 3 study of this drug, TENAYA, is currently underway and enrolling patients.
Gene Therapy
In the more distant future, there may be even greater promise for patients with wet AMD through one or more of the gene therapies that are now being explored in phase 1 and 2 clinical trials.
One of the most intriguing therapies being developed is RGX-314 (RegenxBio). This is a recombinant adeno-associated virus gene therapy vector which carries a coding sequence for a soluble monoclonal antibody fragment. This vector then binds to and neutralizes VEGF within the eye. Essentially, treatment with RGX-314 engineers a patient’s retina to produce Lucentis on its own. The early results are promising, and next-phase clinical trials will be coming soon.
Conclusion
Many new developments are on the way which may soon make monthly anti VEGF injections a thing of the past. There has never been a more exciting time for new treatment breakthroughs in wet AMD research. Through the various mechanisms involved in AMD pathogenesis, there exists multiple targets for new therapeutic interventions. We are slowly but surely discovering more ways to improve visual outcomes in this sight-threatening disease. I am very encouraged by early results with these treatment options, and am excited to share these advancements with our patients.
