



Obesity is a multifactorial disease with genetic, societal, socioeconomic, and environmental influences. As a multisystem disease, obesity’s implications span from insulin resistance to cardiovascular disease and eventually risk premature mortality.
The correlation between obesity and ocular health could not be anymore stark. For starters, obesity-related insulin resistance increases the risk of subsequent retinopathy. Additionally, the presence of excessive abdominal weight may result in increased intracranial pressure with negative visual sequelae.1
Furthermore, chronic obesity fosters a pro-inflammatory state carrying an elevated risk of autoimmune disease and macular degeneration.2,3 With all of these at play, it is crucial that eyecare professionals are educated on the risks so they can pass on this information to their patients.
Overweight and obesity: An epidemic
Understanding the importance of maintaining a “healthy weight” begins with a synopsis of the overweight and obesity epidemic. Overweight and obesity, in tandem, constitute two significant challenges in medicine today.
According to the World Health Organization, being overweight is “a condition of excessive fat deposits,” whereas obesity is “a chronic complex disease defined by excessive fat deposits that can impair health.”4
The organization estimates that nearly 2.5 billion people over the age of 18 are categorized as overweight. Of which, 890 million are diagnosed as obese.5 In the United States, roughly 42.4% of adults are considered obese.6
Understanding body mass index (BMI)
From a clinical position, it’s common practice to reference body mass index (BMI) to evaluate overweight and obese populations. Tracking these values may assist the clinician in understanding the future level of risk for complications such as heart disease or diabetes. BMI is calculated using a patient’s weight (in kilograms) divided by their height (in meters).
Table 1: Further information for BMI ranges in adults over 20 years of age.6
| Body Mass Index | Classification |
|---|---|
| 18.5 to 24.9 | Normal, healthy weight |
| 25 to 29.9 | Overweight |
| 30 to 40 | Obese |
| 40 or more | Severe obesity |
Table 1: Courtesy of the National Institute of Diabetes and Digestive and Kidney Diseases.
Key considerations for BMI
Though many believe tracking BMI may provide a good estimation of future health, controversy exists regarding the validity of these measurements and their utility in weight management. As an example, BMI measurements commonly misrepresent athletes as overweight or obese due to an increased presence of muscle mass and overall weight.7
BMI may also inaccurately portray patients in minority communities. The indices and subsequent classifications are primarily reflective of white populations. Therefore, these classifications may not consider the differences in body composition that vary across demographics. For example, according to Harvard Health, BMI tends to be overestimated in Black patients and underestimated in patients of Asian descent.7
Shedding light on the link between obesity and ocular disease
Obesity is associated with an extensive array of ocular complications. A primary driver being subsequent metabolic syndrome and a chronic inflammatory state. Most of the conditions are managed therapeutically; however, each of these conditions would benefit greatly if conventional treatments were paired with weight management.
Diabetic retinopathy
As metabolic syndrome persists, there ensues an elevation of reactive oxidative species and a decrease in the capacity of antioxidants. Reactive oxidative species cause severe damage to multiple cellular components, thus resulting in chronic retinal inflammation.8
The forces of hyperglycemic oxidative stress and pro-inflammatory cytokines multiply, leading to vascular endothelial damage. This damage causes leukocyte oxidative burst and an increase in vascular permeability. Ultimately, the sequence reaches a climax with the pericyte and vascular endothelial cell death responsible for sight-threatening complications typically associated with diabetic retinopathy.9
More and more evidence suggests that weight control via exercise, glucagon-like peptide-1 (GLP-1) receptor agonists, and a healthy diet yields greater benefits than standalone, traditional ophthalmic therapies.10
Figure 1: Fundus image of proliferative diabetic retinopathy with vitreous hemorrhage, a temporal preretinal heme, intraretinal hemorrhages, and blot hemes.


Figure 1: Courtesy of Roya Attar, OD, MBA, DHA, FAAO.
Dry eye disease
Obesity risks exacerbating dry eye disease through the presence of a chronic, pro-inflammatory environment.11 Another theory considers the abundance of estrogen as compared to testosterone in obese patients, and posits these low androgen levels may contribute to a reduction of trophic support to meibomian glands.
The common association between meibomian gland dysfunction (MGD) and hormonal imbalance often assumes too little estrogen—as exhibited in menopausal patients.
However, further research has determined that an abundance of estrogen may also interfere with appropriate levels of meibomian gland secretion.11 In either case, obesity—with its effects on hormonal balance—may be an elusive culprit in the progression of meibomian gland dysfunction.
Figure 2: Closeup of inflamed meibomian glands, likely caused by MGD.

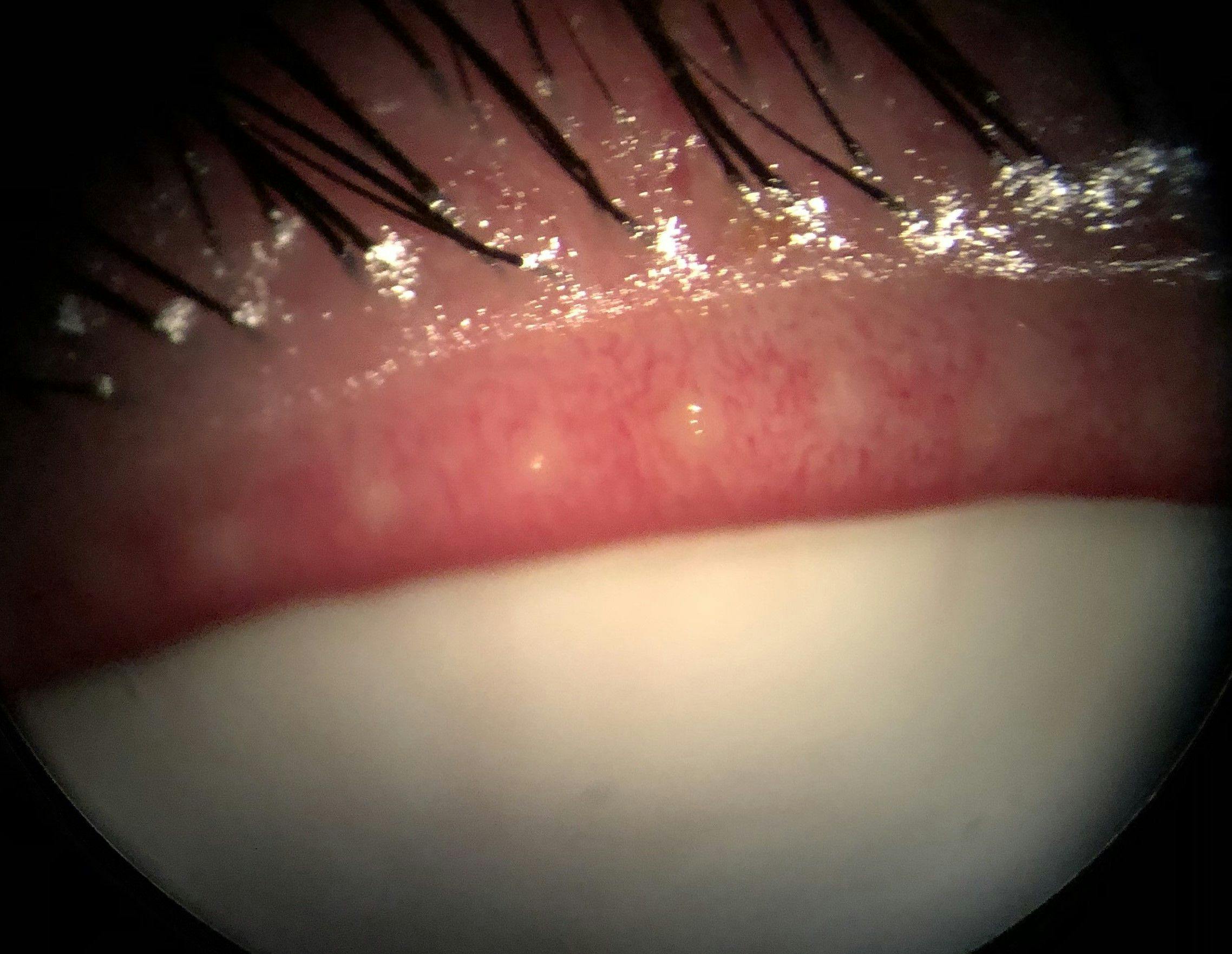
Figure 2: Courtesy of Cory Lapin, OD, MS, FAAO.
Idiopathic intracranial hypertension (IIH)
Idiopathic intracranial hypertension (IIH) is the modern medical terminology for the condition formerly referred to as pseudotumor cerebri (PTC). The condition is most common among young women, ages 20 to 50,12 with a BMI of 30 or more.13
The pathophysiology of IIH is not fully understood, though there are possible explanations, including:14
- Venous stenosis
- Certain medications, such as steroid, tetracyclines, and vitamin A
- Hormones; females are nine times more at risk (although, the role of hormones is not fully understood)
However, what is known for certain, is that the condition is strongly correlated with obesity.13 The obesity hypothesis ascertains that excess abdominal weight may influence intra-abdominal pressure. The heightened abdominal pressure interacts with venous pressure, thereby increasing intracranial pressure and resulting in bilateral disc edema.
These patients will often experience neurological complaints, such as recurrent or progressing headaches, pulsatile tinnitus, and dizziness. Ocular complaints may present as more subtle in earlier stages, with some patients presenting as asymptomatic.
However, without adequate management, patients may present with diplopia, visual field defects, reduced best-corrected visual acuity, and amaurosis fugax.
Figure 4: Initial clinical presentation of a 36-year-old patient with IIH who had a history of obesity, hypertension, and oral contraceptive use (Estarylla).


Figure 4: Courtesy of Kevin Cornwell, OD.
Diagnosing patients with IIH
Understanding visual field defects in these patients is crucial to proper management. According to a small study in the UK, 1 to 2% of newly diagnosed cases are likely to exhibit blindness within 1 year of the disease diagnosis.15 Other patients may exhibit peripheral field defects or blind spot enlargement.
Diagnosis requires neuro-imaging to rule out the presence of intracranial lesions and lumbar puncture to identify the risk of pathogenic species as well as opening pressure. It’s best practice to order the MRI/MRV prior to the lumbar puncture to rule out intracranial tumors. The presence of an intracranial tumor may result in brainstem herniation subsequent to CSF removal following a lumbar puncture.16
Other considerations would include ruling out known causes of bilateral disc edema. A non-exhaustive list of these might include vitamin A derivatives, tetracyclines, and birth control.17
It is crucial to understand that IIH is a diagnosis of exclusion. The provider must be certain to eliminate other possible etiologies prior to diagnosis. Treatment may be divided into three basic categories: weight loss, medication, surgery.
On average, a 15% weight reduction is correlated to reduced intracranial pressure and improvements in visual function.18 Weight loss may also be paired with medicated therapies such as furosemide or acetazolamide.
In advanced cases, neurology may advise the placement of a ventriculoperitoneal or lumboperitoneal shunt; proper body weight is critical in securing both the longevity and function of the shunt.16
Age-related macular degeneration (AMD)
The link between AMD and obesity is complicated. A meta-analysis summarizing the risk of AMD development among overweight and obese individuals determined an associated risk of early and significantly increased risk of developing late AMD.2
Two pro-inflammatory chemical messengers, MCP-1 and TNF-α, were identified as probable causes for this increased risk. It’s hypothesized that the activity of MCP-1 and TNF-α within the retina causes monocyte infiltration within the RPE and subsequently disrupts normal function.2
Perhaps even more intriguing is the secondary hypothesis. It’s presumed that increased adiposity attracts fat-soluble carotenoids away from the macula and into adipose tissue.
Effectively, fat-soluble macular carotenoids, such as lutein and zeaxanthin (antioxidants abundant in the AREDS2 formula), are suggestively measured at lower quantities in macular tissue due to their attraction to adipocytes.2 This would increase, to a degree, as an individual adds further adipose tissue.
The study concludes that the information regarding the impact of obesity and AMD is limited. For this reason, even as more evidence indicates a link between these conditions, considering weight loss as a part of a healthy lifestyle is advised. However, the actual risk correlation between obesity and AMD requires further research before definitive conclusions can be drawn.
Figure 5: Fundus photograph of a patient with intermediate AMD, demonstrating large drusen >125 microns and AMD pigmentary abnormalities.

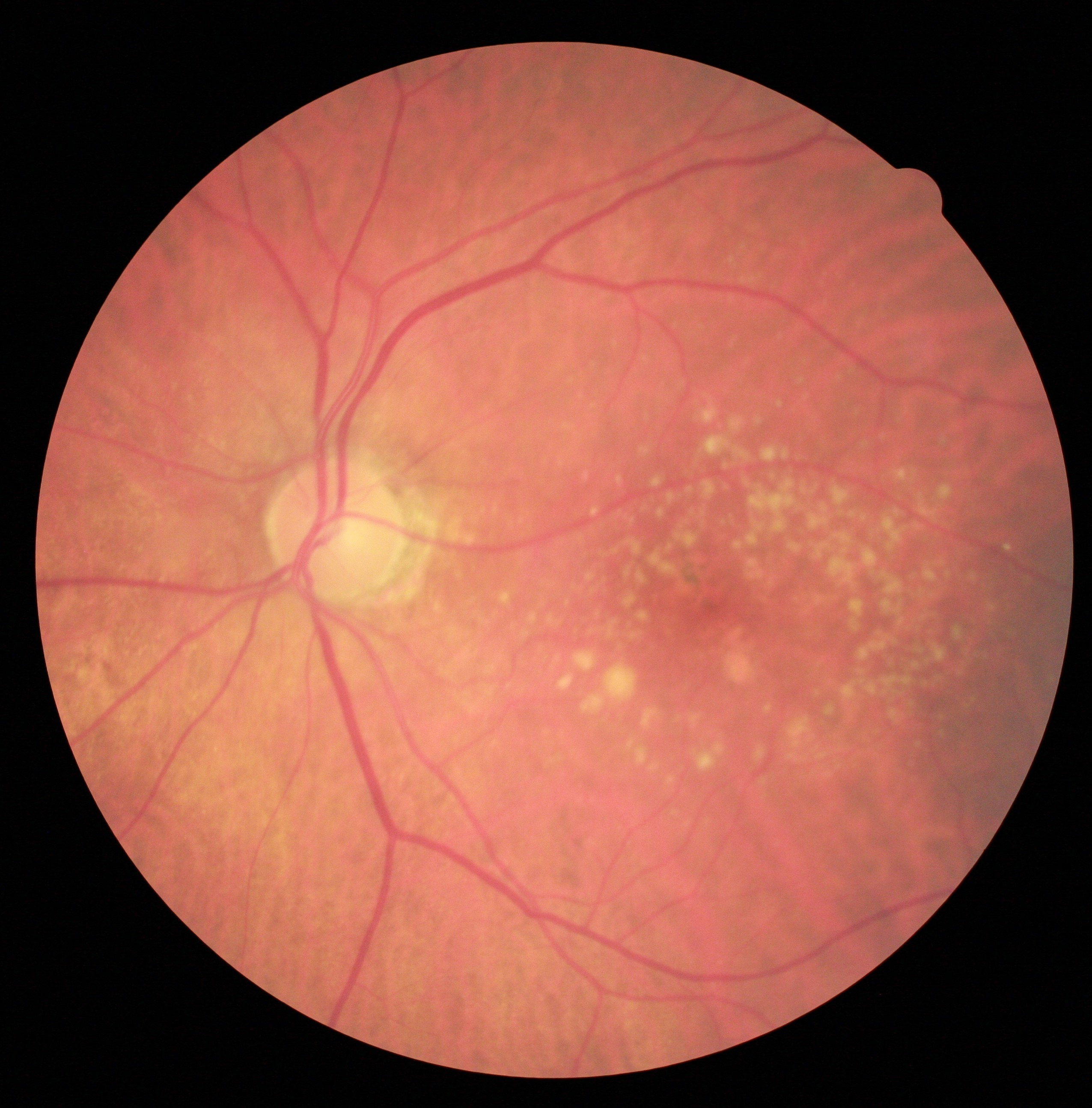
Figure 5: Courtesy of Julie Rodman, OD, MSc, FAAO.
Glaucoma
It’s possible that open-angle glaucoma is related to decreased levels of adiponectin with increased insulin resistance.20 Normal-tension glaucoma may be attributed to vasculopathic diseases commonly associated with hypertension and diabetes,1 both of which occur at a higher incidence within obese populations.
Interestingly, a Chinese study examining the incidence of glaucoma within obese populations found that men were at a higher risk than women. This was attributed to estrogen acting in a protective capacity for retinal ganglion cells.19
Additionally, the study demonstrated that glaucoma diagnosis in obese patients may simply occur at a higher rate due to a greater frequency of ophthalmology visits, oftentimes for other retinal pathologies.
Figure 6: OCT RNFL analysis of a patient with NTG, note the temporal RNFL thinning and paracentral/ganglion cell complex defects.


Figure 6: Courtesy of Justin Schweitzer, OD, FAAO.
Cataracts
Regarding cataracts, obesity appears to increase the risk for posterior subcapsular and cortical cataracts, albeit not nuclear sclerosis.20 It’s hypothesized that the mechanism is related to oxidative stress. In a rat model, it was proven that higher levels of oxidative stress are related to oxidative damage in lenticular tissues.1
However, other studies contradict this precept. A study from Asia, published in the American Journal of Epidemiology, argues that this association is not definitive. According to the article, study results suggest no demonstrable, causal correlation between obesity and posterior subcapsular or cortical cataracts.21
Other ocular diseases and considerations
Aside from the conditions listed above, obesity should be considered as a risk factor for a host of other potentially blinding conditions.
Obesity is directly related to metabolic syndrome, vasculopathic diseases, and many other undesirable sequelae—consider the risk for retinal pathology, such as central / branch retinal arterial occlusion, central/ branch retinal vein occlusion, and ocular ischemic syndrome.1
A comprehensive analysis of obesity and autoimmune disease determined an association between obesity and a long list of diseases linked with ocular complications, including:3
- Thyroid dysfunction
- Grave’s disease
- Rheumatoid arthritis
- Crohn’s disease
- Ulcerative colitis
- Multiple sclerosis
- Myasthenia gravis
- And others
The underlying theme is the release of pro-inflammatory mediators from adipose tissue. According to a two-sample Mendelian randomization (MR) study titled, The Causal Effect of Obesity on the Risk of 15 Autoimmune Diseases, “excessive body weight results in overactivation of intracellular nutrient pathways and energy-sensing pathways, resulting in metabolic overload or peripheral tissues involved in immune response.”3
In addition to the aforementioned, the secretion of the pro-inflammatory cytokines from adipose tissue magnifies overall dysfunction.
Figure 7: Close-up of a thyroid eye disease (TED) suspect patient with a medical history of hyperthyroidism.


Figure 7: Courtesy of Audrey Ko, MD.
Conclusion
For clinicians practicing in a primary eyecare setting, counseling patients on the importance of proper BMI maintenance will reduce disease risk and enhance quality of life.
Although the science of obesity and disease is not fully understood, common themes regarding immune dysfunction and chronic inflammation may explain higher rates of risk within this population.
Remember, what happens in the body will reflect in the eyes; healthy eyes are simply a reflection of a healthy body. Don’t be afraid to address BMI and co-manage with primary care providers and dietitians. Doing so may save both vision and a life.
