


Retinal dystrophies (RDs) and inherited retinal diseases (IRDs) refer to a genetically and clinically heterogeneous collection of disorders pertaining to progressive retinal degeneration.
These disorders predominantly involve the photoreceptors (rods and cones) and / or the retinal pigment epithelium (RPE), and result in various extents of visual disability or total blindness.1
Though historically deemed incurable, the last decade has witnessed great strides in molecular diagnosis, genetic therapy, and interdisciplinary management strategies that hold promise for these patients.
Etiology and genetics of inherited retinal diseases
IRDs are monogenic conditions typically resulting from mutations in genes essential for the survival of the photoreceptors, the process of phototransduction, and retinal cell metabolism. To date, over 270 genes have been implicated, including some major contributors of the proteins responsible for visual function such as RHO, ABCA4, RPGR, USH2A, CHM, and RPE65.1,2
Genetic mutations may be inherited in autosomal dominant, autosomal recessive, X-linked, or mitochondrial fashion. Significantly, even among family members with the same defect, phenotypic variability is prevalent, making diagnosis and management challenging.
Whereas monogenic IRDs usually begin to occur early in life, advanced retinal disorders such as age-related macular degeneration (AMD) appear later as a result of interaction between genetic susceptibility and environmental factors.3
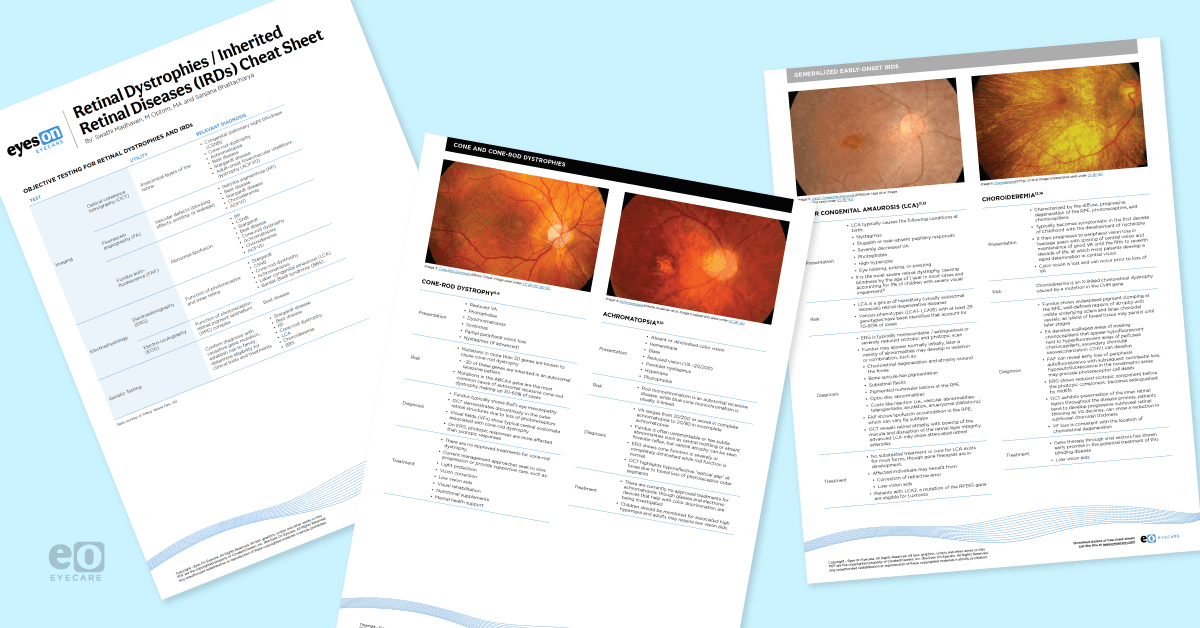
Download the Retinal Dystrophies / Inherited Retinal Diseases (IRDs) Cheat Sheet here!
With 10 fundus photos of retinal dystrophies

Retinal Dystrophies / IRDs Cheat Sheet
This cheat sheet on retinal dystrophies and IRDs features a table of clinical findings on imaging, 10 fundus photographs, and emerging therapies in the pipeline!

Classification of retinal dystrophies
Distinct RDs are usually classified by the most affected photoreceptor (rods vs. cones), rate of progression (stationary vs. progressive), and by the presence of systemic symptoms (syndromic vs. non-syndromic).
Rod and rod-cone dystrophies
- Retinitis pigmentosa (RP) is the most common inherited retinal disease, with the onset of night blindness and peripheral field defects at an early stage. Fundoscopy can reveal bone-spicule pigmentation, attenuation of the vessels, and waxy pallor of the disc.
- While vision deficits initially present peripherally, central vision gradually fails as well. Different variants of RP create a wide variety of presentations and visual function.
- Congenital stationary night blindness (CSNB) occurs as a non-progressive condition in infancy, presenting with nyctalopia along with a normal fundus. Electroretinography (ERG) usually shows a typical "electronegative" pattern.
Cone and cone-rod dystrophies
- Photophobia, diminished central visual acuity, and color vision disturbances mark the onset of cone-rod dystrophy (CRD). As the condition progresses, the patients may develop night blindness and peripheral field defects due to secondary rod involvement in CRD. The rate of progression of the rod-related symptoms can vary based on the underlying genetic mutation.4
- Achromatopsia and cone monochromatism become apparent in the early months of life. It is followed by presentation of day blindness, nystagmus and diminished visual acuity. While there is a chance the impaired colour vision may be from birth, it is only recognised at the later years due to the feasibility of proper testing.
Generalized early-onset IRDs
- Leber congenital amaurosis (LCA) is a profound dystrophy with manifestations in the first year of life involving significant vision reduction, nystagmus, and undetectable ERG recordings.5
- Progressive atrophy of the choroid, RPE, and the photoreceptors occurs with choroideremia, resulting in nyctalopia and peripheral field narrowing. Inheritance is X-linked, generally occurring in males.6
Macular dystrophies
- Stargardt disease is caused by mutations of the ABCA4 gene. It typically begins during adolescence or early adulthood with a gradual loss of central vision. On fundus examination, yellow-white pisciform (fish-tail shaped) flecks appear at the level of the RPE, especially in the posterior pole.
- As the condition progresses, macular atrophy may develop, often with a distinctive “beaten bronze” appearance. Night vision is usually preserved in the early stages.
- Best vitelliform macular dystrophy is an autosomal dominant condition linked to mutations in the BEST1 gene; it often arises in childhood or adolescence with blurred central vision and metamorphopsia. Early fundus findings include the classic “egg-yolk” vitelliform lesion in the macula due to lipofuscin buildup.
- Over time, this lesion may fragment—sometimes described as progressing to a “scrambled egg” stage—leading to central atrophy and vision decline. Peripheral vision generally remains unaffected.
- Adult-onset vitelliform macular dystrophy resembles Best disease but appears later in life, typically between the fifth and sixth decades. It’s associated with mutations in BEST1 or PRPH2. Lesions are often smaller and less well defined, and symptoms—such as subtle central vision changes—may be more modest initially.
- While often milder than Best disease, it can still progress to macular atrophy over time.
Syndromic inherited retinal dystrophies
- Usher syndrome is defined by the combination of RP and bilateral sensorineural hearing loss. It may also involve vestibular dysfunction in certain subtypes. Fundus findings are consistent with RP, including bone-spicule pigmentation, vessel narrowing, and optic disc pallor.
- Bardet-Biedl syndrome: a multisystem genetic disorder characterized by RP along with features such as obesity, polydactyly, kidney abnormalities, and cognitive impairment. Early symptoms may include night blindness (nyctalopia) and progressive peripheral vision loss. Fundus findings align with classic RP.7
Figures 1, 2, and 3: Fundus images of Bardet-Biedl syndrome, choroideremia, and Leber congenital amaurosis, respectively.




- Figure 1:Bardet-Biedl Syndrome© Christian Hamel. Image used under CC BY 2.0.
- Figure 2: Choroideremia©Ying Lin et al. Image cropped and used under CC BY 4.0.
- Figure 3: Leber Congenital Amaurosis©Natsuki Higa et al. Image cropped and used under CC BY 4.0.
To see more fundus images of retinal dystrophies, download the cheat sheet!
Diagnosis of retinal dystrophies
The clinical presentation of IRDs varies from a color vision deficiency to a severe visual disability.
Key clinical indications of RDs include:
- Night blindness (nyctalopia): Indicates involvement of rods (e.g., RP, CSNB)
- Reduced visual acuity and photophobia: Both are found in cone dystrophies
- Family history: May aid in identifying inheritance patterns
- Changes in color vision: Described in cone-rod dystrophy and achromatopsia
Diagnostic tools
- ERG: Critical to the identification of rod- and cone-dominant disorders by employing the International Society for Clinical Electrophysiology of Vision (ISCEV) standards
- Optical coherence tomography (OCT): May reveal photoreceptor damage or sub-RPE deposits, and allows for anatomical visualization
- Fundus autofluorescence (FAF): Highlights areas of RPE atrophy or metabolic illness of RPE (e.g., lipofuscin deposition in Stargardt disease)
Genetic testing
- NGS panels: Target an increasing number of RD-associated genes
- MLPA and microarrays: Identify large deletions or duplications not detected by sequencing
- Genetic testing: Necessary not only for diagnosis, but for family counseling and access to gene therapy as well.2
Pathophysiology: Beyond the gene
Whereas genetic mutations trigger the disease, secondary mechanisms including oxidative stress, chronic inflammation, and cell death pathways play a large role in the degeneration of the retina.5
This can occur via a number of pathways, including:5
- Photoreceptors, particularly rods, are highly oxygen-demanding and susceptible to oxidative damage.
- Microglial activation following cell death results in the release of pro-inflammatory cytokines (e.g., TNF-α), causing further damage.
- The core pathways involved are NF-κB, JAK/STAT, and MAPK, which are common to numerous neurodegenerative diseases.
Management strategies for IRDs
A cure for most IRDs does not currently exist, but management strategies and available treatments target slowing the progression and maximizing remaining vision. The investigation of new therapies is ongoing.
Supportive care for IRDs
- Aids for low vision, orientation, and mobility.
- Psychological assistance to manage emotional and social effects.
Genetic counseling and therapy
- After diagnosis confirmation, patient education regarding inheritance patterns is a critical, and often overlooked, aspect of patient management for those conditions.
- Luxturna (voretigene neparvovec) is FDA-approved for RPE65-related RP and LCA. Luxturna is administered subretinally with promising outcomes for improved visual function.3
- Ongoing trials target the following genes: RPGR (X-linked RP), CHM (choroideremia), and ABCA4 (Stargardt).
Stem cell and optogenetic therapy
- Experimental therapies involve replacement of the photoreceptors through induced pluripotent stem cell (iPSC)-derived retinal cells and light-sensitive protein reprogramming.
Pharmacologic therapy
- Antioxidants (such as lutein, vitamin A) and neuroprotectants are directed at slowing the degeneration.
- RNA therapies and antisense oligonucleotides are being developed for splicing disorders.
Focus on future therapies for RDs and IRDs
The intersection of genomics, AI imaging technologies, and precision medicine is revolutionizing retinal dystrophy care. Real-time tracking of the course of the disease and targeted interventions might become the new norm in the near future. CRISPR/Cas9 and base editor technologies are being tested to directly modify mutations within the retinal cells.
These are highly targeted gene-editing tools that allow for DNA corrections. With these, inherited retinal conditions can be addressed at their genetic root, especially in cases where traditional gene replacement therapy is not feasible due to gene size or delivery challenges.
However, despite advancements, several challenges continue to limit the widespread impact of these emerging therapies for inherited retinal diseases. For low-resource settings and for patients without insurance coverage or access to specialized centers, the high cost and limited accessibility of gene therapies remain major barriers.
Secondly, phenotypic variability complicates diagnosis, prognosis, and treatment selection even among individuals with the same genetic mutation. This makes it difficult to predict clinical outcomes or tailor therapies precisely.
Finally, the lack of comprehensive, long-term patient registries hinders our ability to track treatment responses over time, identify suitable candidates for clinical trials, and refine disease classification based on natural history and therapeutic outcomes.
Conclusion
A diagnosis of retinal dystrophy no longer carries the inevitability of irreversible vision loss. With earlier detection, advances in genetic testing, and emerging treatments like the approval of Luxturna for RPE65-related disease, patients have access to targeted options that were once unimaginable.8
While current therapies benefit only a small subset of individuals, they signal a growing shift toward personalized care. As eyecare professionals, staying informed about these evolving possibilities allows us to offer accurate guidance, meaningful referrals, and a renewed sense of hope to those affected.
