



A 71-year-old female presented to the clinic to re-establish ocular care for systemic lupus erythematosus (SLE).
She had been lost to follow up for 3 years, but had been followed in my clinic for 10 years. Her rheumatologist had diagnosed her with SLE 16 years prior, due to a mild facial rash, and immediately started hydroxychloroquine 200mg BID, with which the patient was compliant.
Since the initiation of hydroxychloroquine therapy, her rash resolved and she never developed any other SLE symptoms nor did she complain of any visual changes. Her medical history was otherwise unremarkable though she was frail appearing, weighing 100 lbs (45kg) with a height of 5’5 (1.5m).
Her clinical exam with me was mostly unremarkable. Best corrected entering acuities were 20/20 OD and OS with a mild myopic prescription. She had trace nuclear sclerotic cataracts in both eyes and non-macular drusen most prominent in the superior-temporal arcades of both eyes. Due to her long-term use of hydroxychloroquine, a 10-2 visual field and macular OCT imaging was ordered.
My preferred hydroxychloroquine screening OCT protocol is to perform a macular cube scan and a HD 5-line raster scan. The macular cube scan provides volumetric quantifiable data while the HD 5-line raster scan provides high resolution imaging of the retinal anatomy.

Figure 1: Fundus photo
The macular cube report revealed central and paracentral thinning of both eyes. Review of the HD 5-line raster in the right eye did not reveal any significant changes in retinal architecture. In contrast, very early paracentral attenuation of the ellipsoid zone was noted in the left eye. The OCT changes in the left eye were extremely mild and I do not think that I would have appreciated them if it wasn’t for the quantified thinning on the macular cube report.
The 10-2 visual field testing confirmed the presence of hydroxychloroquine retinopathy with bilateral paracentral and central defects. The defects were more prominent in the left eye which correlated with the greater structural defects on OCT.
Figure 2 represents correlated OCT and visual fields.


Figure 2
Though the patient’s recent adherence to follow up was poor, the patient did have 7 years of unremarkable ocular exams, visual field testing, and OCT imaging prior to being lost to follow up. I reviewed her previous OCT scans and visual fields which were all unremarkable. Due to the poor correlation between the latest OCT and visual field, I ran an OCT progression analysis to determine if the OCT changes in the left eye were truly new and degenerative.
As seen in Figure 3, the progression analysis showed definitive symmetric degeneration of the central and paracentral macula which solidified the diagnosis of hydroxychloroquine retinopathy.

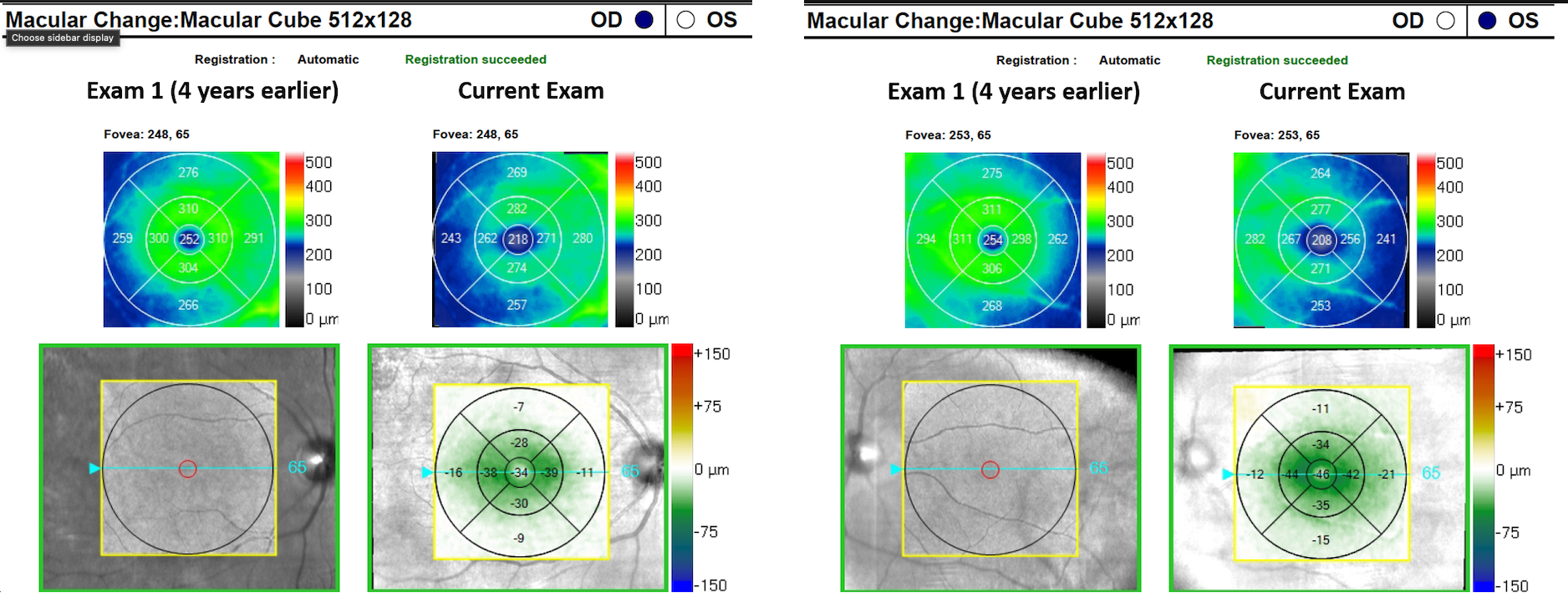
Figure 3: Progression analysis
I apprised the patient of all the findings and explained that a change in her medication was likely necessary. Though the patient had conclusive signs of hydroxychloroquine retinopathy, another day of treatment would not cause severe ocular harm whereas discontinuation could lead to a SLE flare up.
I contacted the patient’s rheumatologist and explained my findings, at which time we both decided that stopping the hydroxychloroquine would be the best course of action. I repeated visual field and OCT testing two more time over the next year to ensure that the patient did not have continued progression and eventually discharged the patient to yearly dilated exams.
Hydroxychloroquine retinopathy
Hydroxychloroquine (and chloroquine) retinopathy is characterized by bilateral and symmetric paracentral (≤10 degrees of the fovea) macular damage starting in the photoreceptors and eventually affecting the RPE. This degeneration progresses until parafoveal RPE depigmentation leads to the clinical sign of bull’s eye maculopathy. Though hydroxychloroquine retinopathy is classically thought to be a macular condition, pericentral disease closer to the vascular arcades has been noted and is particularly common in Asian populations.
The early-moderate stages of hydroxychloroquine are subclinical and can only be detected with auxiliary testing such as SD-OCT, visual field testing, fundus autofluorescence, or electrodiagnostic testing. OCT macular imaging will reveal outer retinal and RPE degeneration in an annular pattern centered on the fovea, either in the paramacular or pericentral regions. A ring scotoma or partial ring scotoma on visual field testing will correlate to the structural OCT damage.
Once funduscopic signs of hydroxychloroquine are noted, disease severity is usually moderate-severe and visual acuity is likely to be affected. If the retinopathy is allowed to progress, diffuse retinal and RPE atrophy will lead to significant loss of central, peripheral, and night vision.
Management of the hydroxychloroquine patient
Though no preventative or restorative treatment is available for hydroxychloroquine retinopathy, strict screening protocols are extremely effective at preventing vision loss. The American Academy of Ophthalmology’s hydroxychloroquine screening protocols have gone through several editions with the latest update published in 2016.1 The most recent screening recommendations are to perform a comprehensive ocular exam within a year of initiation of long term hydroxychloroquine therapy.
The purpose of the examination is to detect high risk characteristics (summarized in figure 4) and preexisting ophthalmic conditions that may increase the risk of hydroxychloroquine retinopathy or preclude proper screening for hydroxychloroquine retinopathy. The authors state that “although baseline visual fields and SD OCT are always useful, it is not critical to obtain them at baseline unless abnormalities are present.”1
The authors go on to state that annual screening with 10-2 visual field (24-2/24-2c/30-2 in Asian patients) and OCT imaging are not necessary until patients have had 5 years of hydroxychloroquine therapy or have high risk characteristics.1
Hydroxychloroquine retinopathy high risk factors1
Major risk factors:
- Daily dosage >5mg/kg real weight
- Duration of use >5 years (assuming no other risk factors)
- Presence of renal disease/subnormal glomerular filtrate rate
- Concomitant tamoxifen use
- Pre-existing retinal disease that may preclude proper screening or increase risk of retinopathy (myopic maculopathy, cone dystrophy, macular scarring, etc)
Despite the latest published hydroxychloroquine guidelines, I and many eye care practitioners take a more conservative approach to screening, ordering yearly visual field and OCT testing even in patients without high risk factors. Though I understand the risk of developing hydroxychloroquine retinopathy is quite low in the early years of treatment in patients without high risk characteristics, screening visual and OCT testing is easy, quick, and noninvasive so I still choose to complete it annually.
Speaking with rheumatologists, many of them also prefer to complete screening annually since that is how they were trained. Another reason that I like to complete screening tests yearly is due to the visual field learning curve that many patients have to overcome. Without good baseline data it may be difficult to detect early retinal toxicity.
Back to the patient
One of the hallmarks of the latest hydroxychloroquine retinopathy screening protocol is the stratification of patients into high risk and low risk categories. My patient was quite thin, weighing 100lbs (45kg) at a height of 5’5 (1.5m). She was taking 200mg BID of hydroxychloroquine daily for 16 years. The daily dose for her is 8.9 mg/kg which is significantly higher than the <5mg/kg cut off for high risk patients. Both her daily dose and her duration of treatment put her in a high risk category for the development of hydroxychloroquine retinopathy.
Luckily, the retinal toxicity was detected with OCT and visual field testing before the patient developed any symptoms or vision loss. After a discussion with her rheumatologist, the hydroxychloroquine was discontinued and the patient monitored for further retinal degeneration. No further deterioration was noted and the patient was discharged to annual comprehensive examination without OCT and visual field screening.
Hydroxychloroquine retinopathy is a rare condition that can lead to irreversible vision loss. Screening is focused on evaluation for high-risk characteristics, outer retinal and RPE OCT degeneration, and paramacular or perimacular visual field scotomas.
As the prevalence of autoimmune conditions continues to increase, the long-term use of hydroxychloroquine will likely increase as well. The screening of these patients offers a great avenue for co-management between eyecare providers and rheumatologists, ensuring that patients get proper systemic treatment without sacrificing their vision.
In January 2022, the FDA approved Vabysmo, a first-of-its-kind bispecific antibody for AMD and DME. Get an overview of this exciting medication along with insights from two top ophthalmologists. Click here to view the resource.
