There is no question that optical coherence tomography (OCT) has revolutionized how optometrists and ophthalmologists examine the eye.
OCT has become indispensable for the medical eye care practitioner. Whether it is helping to localize a retinal lesion to a certain retinal layer, or finding retinal nerve fiber layer defects, OCT is as important to medical eyecare as the phoropter is to refraction. Though OCT cannot replace a dilated fundus exam and a keen eye and mind, it has significantly eased the clinician’s burden in differentiating ocular pathology.
Optical coherence tomography is a noninvasive technology for imaging various ocular tissues using light. Modern day OCT allows indirect visualization of the posterior vitreous, retina, retinal pigment epithelium (RPE), and choroid. Unlike fundus photography or funduscopy, OCT images are false views of the retinal anatomy, generating a map of changes in refractive indices. After significant research and clinical work, these optical maps have been correlated to known retinal anatomy.
Large changes in the index of refraction, such as between the vitreous and the retina, will lead to a very distinct demarcation on OCT. Optically homogeneous structures (which reflect little light) will be relatively dark (such as the vitreous) whereas optically heterogeneous structures (which reflect a lot of light) will be relatively bright (such as the retinal nerve fiber layer).1
When looking at OCT B-scan images with the false color scale, highly reflective structures are represented by warmer colors such as red and orange whereas less reflective structures will be illustrated as cooler colors like green and blue.
When looking at an OCT image of the macula, we often forget that we are not looking at a true image due to the near histologic resolution that modern day OCTs are able to achieve.
As we examine the following OCT images, keep in mind that we are not viewing retinal tissue as it truly is, but as the machine interprets it. It is always helpful to keep a copy of a normal OCT image when examining pathology or to explain pathology to patients.
For this article, all images will be presented in grayscale as I have found it easier to discern the various layers and to spot pathology in grayscale than it is with color images.
The Zeiss Cirrus HD-OCT and the Zeiss Cirrus Photo are both straightforward to use but produce high quality and reproducible images. For these reasons, we chose to use images rendered with a Cirrus 5000 and Cirrus Photo in this article.
The
Zeiss Cirrus is a full capability OCT which can image the cornea, iridocorneal angle, retina and optic nerve. Images of the retina can be performed with different types of scans varying in orientation and resolution.
The 512 x 128 Macular Cube Scan is the workhorse of retinal imaging. It allows for a broad scan of the whole macula. Numerous post-scan analyses such as Macular Thickness Map, Guided Progression Analysis, and RPE Segmentation Map can be performed to aid in the diagnosis and management of retinal disease. The numerous HD and Raster scans provide higher resolution scans which can pick up minute changes in retinal architecture.
The
Zeiss Cirrus Photo combines all these imaging modalities with a high-quality fundus camera. The correlated images allow for quick and easy distinction of retinal lesions. All the following images except for the Normal Retinal OCT were completed with the Zeiss Cirrus HD-OCT during routine clinic evaluation using the 512 x 128 Macular Cube Scan; the Normal Retinal OCT image was captured with a 5 Line Raster Scan.
Want more content dedicated to ocular disease? Check out our medical optometry resource page for tons of clinical cases and images and information on using OCT and ultra-widefield imaging.
Table of Contents
- Normal Retinal Optical Coherence Tomography
- Vitreomacular Traction on Optical Coherence Tomography
- Macular Hole on Optical Coherence Tomography
- Epiretinal Membrane on Optical Coherence Tomography
- Macular Edema on Optical Coherence Tomography
- Central Serous Chorioretinopathy on Optical Coherence Tomography
- Hard Exudate on Optical Coherence Tomography
- Cotton Wool Spot on Optical Coherence Tomography
- Drusen on Optical Coherence Tomography
- Congenital Hypertrophy of the Retinal Pigment Epithelium on Optical Coherence Tomography
- Choroidal Nevus on Optical Coherence Tomography
- Conclusion
Normal Retinal Optical Coherence Tomography
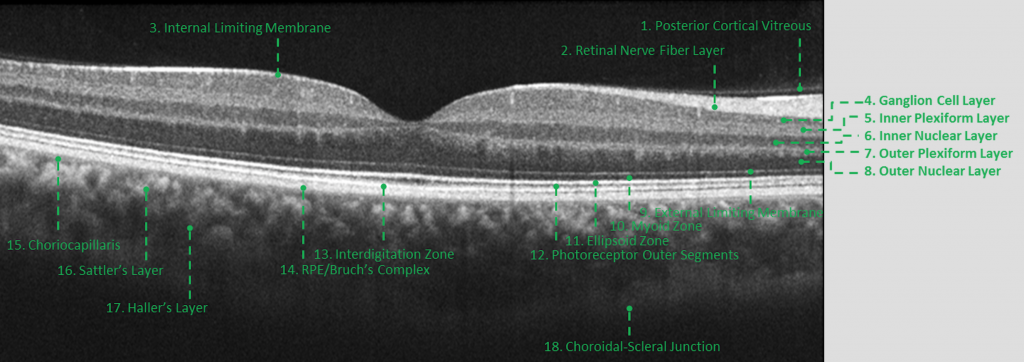
This OCT image is the right eye of a healthy 27-year-old male’s right eye.
Normal eye
Eighteen anatomic landmarks can be visualized here. These landmarks have recently been standardized by the International Nomenclature for Optical Coherence Tomography Panel which is staffed by several of the world’s leading OCT experts.2
There is a stark change in the index of refraction between the optically empty vitreous and the highly
reflective internal limiting membrane (ILM). The retinal nerve fiber layer (RNFL) is thin on the temporal side of the fovea and thick on the nasal side, corresponding to the papillomacular bundle.
Often the posterior cortical vitreous can be seen just barely attached to the macula or floating above it in the case of a complete posterior vitreous detachment.
The ganglion cell layer is significantly less reflective than the RNFL and appears as the darker layer below it. The inner and outer plexiform layers are made up of cell layer connections which are optically irregular leading to higher reflectivity and lighter layers in the image. The inner and outer nuclear layers are composed of densely organized nuclei which are minimally reflective and thus show up as relatively dark layers. The external limiting membrane (ELM) shows up as the first of several thin bands in the outer retina.
The ellipsoid zone (EZ), which has had a contentious naming history and has previously been called the connecting cilia, inner segment-outer segment junction, photoreceptor integrity line, and inner ellipsoid zone, is significantly reflective and separates the myoid zone and the photoreceptor outer segments.3
The integrity of the EZ often correlates to potential retinal acuity. What was once referred to as the RPE or RPE/Bruch’s Complex has now been renamed the interdigitation zone and the RPE/Bruch’s Complex. Under high-resolution conditions, these two layers will show up as two distinct highly reflective bands but under lower resolution conditions can meld into one thicker highly reflective band.
Going forward, I will refer to the interdigitation zone and RPE/Bruch’s Complex simply as the RPE (as there is little clinical value for basic clinical interpretation).
The choroid is visualized posteriorly as three layers, the choriocapillaris, Sattler’s Layer, and Haller’s Layer. These layers may be hard to distinguish with a poorer resolution OCT image. The choroidal-scleral junction is the outer limit of the decipherable OCT layers. The sclera is imaged as the large, homogeneous, outermost structure where little detail is noted.
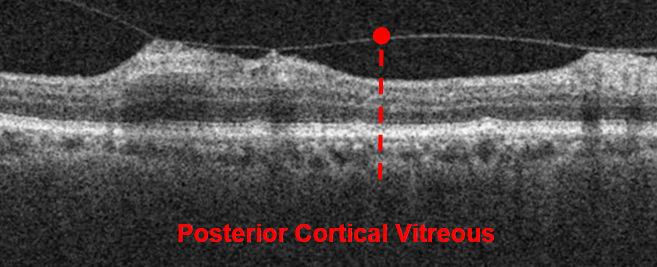
Vitreomacular Traction on Optical Coherence Tomography
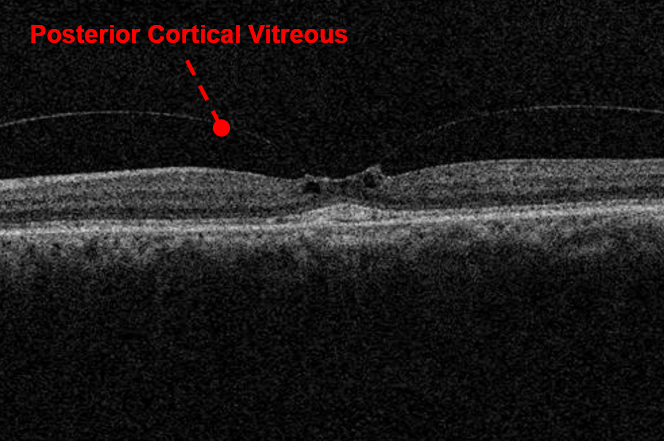
Vitreomacular traction (VMT) is a relatively common vitreoretinal disorder that is often the product of normal vitreal liquefaction and vitreous cortex separation.4
In the majority of cases, this normal age-related process will culminate in subjective floaters and the presence of a Weiss ring upon dilated fundus exam.
Vitreomacular Traction
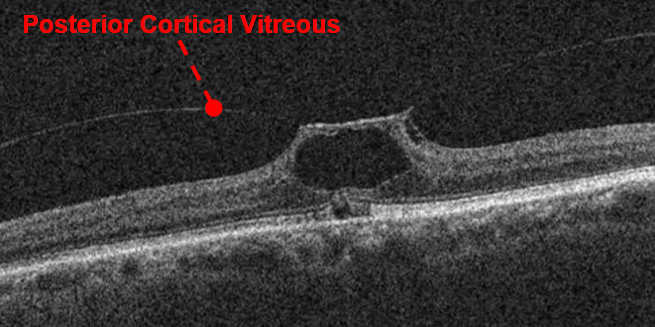
In a minority of cases, the separation of the posterior cortical vitreous from the internal limiting membrane will be incomplete leading to VMT. Ophthalmoscopically, VMT might be difficult to discern but can seen as loss or distortion of the foveal reflex.
Vitreomacular Traction
The classification of VMT, as visualized by OCT, is broken down by size into focal (≤1500µm) or broad (≥1500µm) and whether it is isolated or if concurrent macular pathology is present.4 VMT causes disruption of the macular architecture in the form of foveal distortion, elevation, schisis, edema, or pseudocyst formation.4
Vitreomacular Traction
In contrast, vitreomacular adhesion which is a nonpathological entity represents the normal adherence of the vitreous to the retina and not associated with retinal disruption. VMT often spontaneously resolves but may progress into a lamellar or full thickness macular hole.4
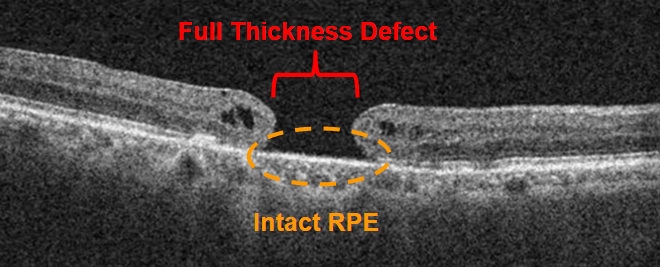
Macular Hole on Optical Coherence Tomography
Common etiologies of lamellar and full thickness macular holes include tractional vitreal forces, epiretinal membrane traction, and trauma.4-7
Macular Hole
All macular holes (full thickness, lamellar, pseudo) are ophthalmoscopically similar, appearing as ovoid or round reddish lesions in fundus photography.
Macular Hole
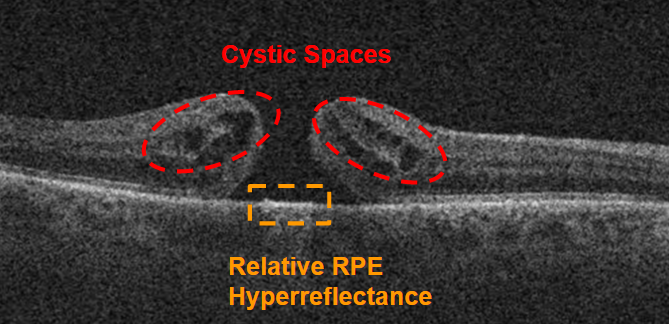
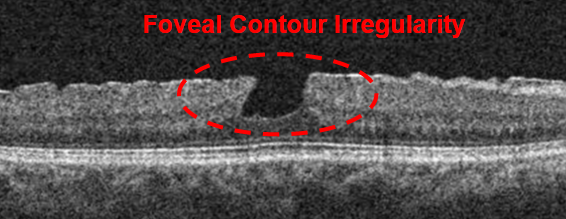
A full thickness macular hole is by definition “an anatomical defect in the fovea featuring interruption of all neural retinal layers from the ILM to the RPE.”4
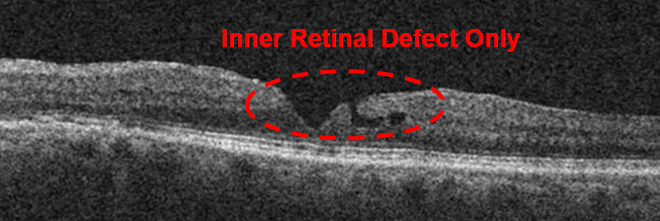
The edges of the hole are typically rounded and pulled anteriorly, often containing intraretinal cavitations. Within the defect, there is often relative hyperreflectance (increased brightness) of the RPE due to the increased incidence of light. In contrast to the full thickness defect, a lamellar hole is often visualized as an irregular foveal contour without outer retina layer disruption.4
Lamellar Hole
Although a macular psuedohole is funduscopically similar to a full thickness and lamellar macular hole, a macular pseudohole has no retinal tissue loss.4 often there is mild to moderate retinal thickening corresponding to epiretinal membrane contracture.
Pseudohole
A macular pseudohole will always be associated with a perifoveal epiretinal membrane.7 Either a Macular Cube Scan, or Raster scan is critical in differentiating these three lesions and any comorbid vitreomacular interactions.
Epiretinal Membrane on Optical Coherence Tomography
An epiretinal membrane is another common vitreoretinal disorder that is easily identified with OCT.
An ERM is caused by fibrous proliferation along the ILM made up of many cell types including glial cells, RPE cells, and inflammatory cells.5
Epiretinal Membrane
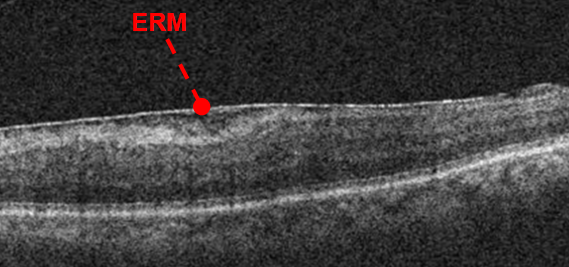
An ERM is seen in fundus photography as a white to yellow irregular reflective tissue overlying the retina. It is theorized that a common etiology of ERM formation is the proliferation of vitreal remnants on the retinal surface.4,5
Epiretinal Membrane
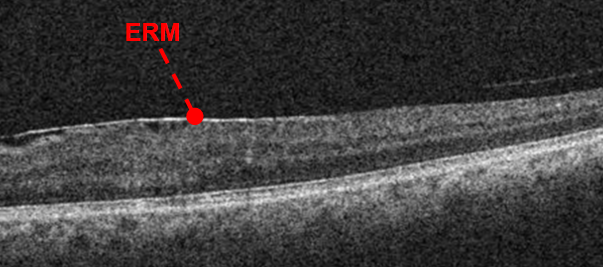
Clinically, it is very common to note the presence of a Weiss ring with an ERM and autopsy studies have found that 50% of eyes examined had remaining vitreal tissue along the retinal surface after a complete PVD.4 Simple ERMs, which are often relatively stationary, without significant contraction will lead to minimal retinal distortion and only mild subjective symptoms.
Epiretinal Membrane
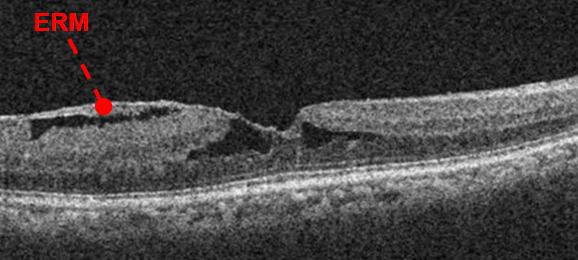
Complex ERMs that have significant contracture can lead to macular pseudohole formation, vascular distortion, edema, and retinal detachment resulting in significant visual disturbances.5 With OCT, an ERM is visualized as a thin diffuse hyperreflective irregularity on the retinal surface. OCT findings will vary considerably with the size of the ERM and amount of traction. As the ERM grows and contracts, more retinal distortion is noted which can lead to cystic formation. OCT is essential in the management of ERMs to assess early changes which can result in significant vision loss if left untreated.
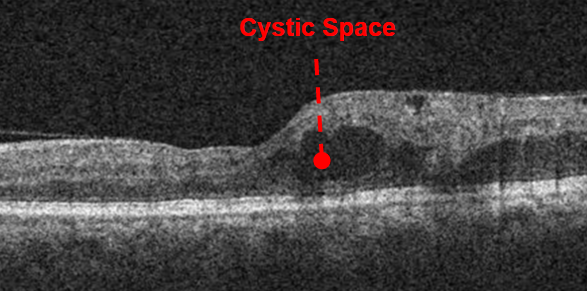
Macular Edema on Optical Coherence Tomography
Macular edema is a nonspecific serous cavitation present in several ocular diseases such as diabetic retinopathy, retinal vein occlusions, Irvine-Gass Syndrome, uveitis, retinitis pigmentosa, and ERM.
Macular Edema
Fluid accumulation is most common within the outer plexiform layer but as more fluid accumulates extension into the inner retina is noted.8 Depending on the associated condition, macular edema is precipitated by vascular damage, ischemia, and/or inflammation leading to blood-retinal barrier breakdown and impaired fluid filtration and removal.8 Due to this complex interplay, macular edema treatment varies greatly and includes Anti-VEGF therapy, steroidal therapy, carbonic anhydrase inhibitors, and laser photocoagulation.
Macular Edema
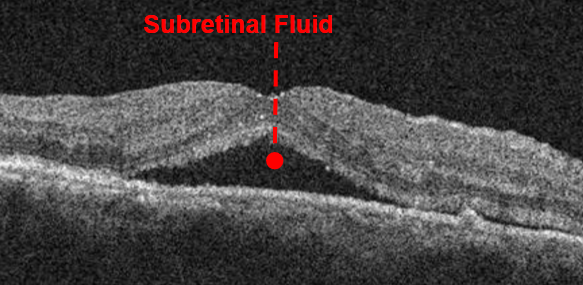
Funduscopically, macular edema is visualized as retinal thickening with or without the presence of hemorrhaging and/or hard exudates. In mild macular edema, retinal thickening may be difficult to appreciate, and instead alteration of the foveal reflex might be noted first. An OCT will easily visualize any edema as areas of retinal thickening and/or cystic spaces. In cases of subretinal fluid, there might be significant retinal thickening without discernible disorganization of retinal layers. Cystic spaces are visualized as discrete hyporeflective pockets within the retina. To aid in management, quantification of regions of macular edema based on ETDRS subregions is possible and readily completed.
The Zeiss Cirrus software allows for reproducible measurements of retinal thickening with a progression analysis which will automatically align images and compare region to region.
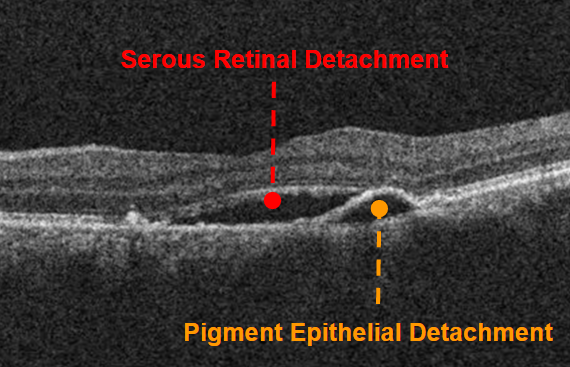
Central Serous Chorioretinopathy on Optical Coherence Tomography
Central serous chorioretinopathy (CSCR) [also known as central serous retinopathy] is a relatively common and often self-limiting chorioretinopathy characterized by fluid accumulation underneath the retina or RPE.10 Though the pathogenesis is still unclear, steroid use and prolonged emotional stress have been implicated.11 More recent multimodal imaging studies have revealed a thickened and hyperpermeable choroid as common findings.12
Central Serous Chorioretinopathy (CSCR)
Recently it has been suggested that CSCR is part of a category of retinochoroidopathies dubbed Pachychoroid Spectrum Disorders.12 CSCR is noted as a retinal detachment with or without the presence of a pigment epithelial detachment (PED). PEDs often have an orange hue which can make them difficult to distinguish from RPE changes and lipofuscin deposits. Resolved CSCR often results in lingering pigmentary disturbances and visual distortion. A serous retinal detachment is often visualized with an OCT as a smooth diffuse elevation of the neurosensory retina which is wider than it is taller. The RPE will be noted underneath the pocket of optically blank fluid. In contrast, a PED is almost always smaller with similar height and width.
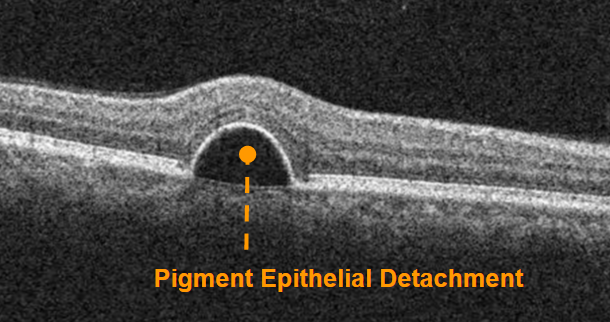
Pigment Epithelial Detachment
An OCT image might reveal areas of RPE atrophy and PED outside the funduscopically noted area of disease which is more consistent with a multifocal or chronic CSCR. In some cases, a PED without a neurosensory detachment might be noted. These PEDs sometimes resolve but can be stationary over years. Solitary PEDs might be thought of as an aborted CSCR but in my opinion are likely a finding somewhere on the pachychoroid disorder spectrum. OCT is vital in determining whether a patient can be monitored by me for a relatively benign case of CSCR or needs to be referred to a retinal specialist to rule out a malicious entity that needs immediate treatment.
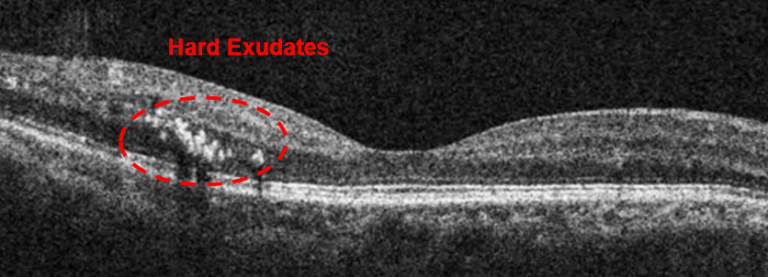
Hard Exudate on Optical Coherence Tomography
Funduscopically, white spots and dots are often difficult to localize to a certain retinal layer confounding the diagnosis. Hard exudates, cotton wool spots, and drusen vary in size, shape, and color which can impede proper diagnosis.
Hard Exudates
Hard exudates are lipid products originating from the retinal vasculature and often found in conjunction with macular edema. With fundus examination, hard exudates are seen as reflective white to yellow lesions with distinct borders. When imaged with OCT, hard exudates are seen as highly reflective lesions within or near the outer plexiform layer.13
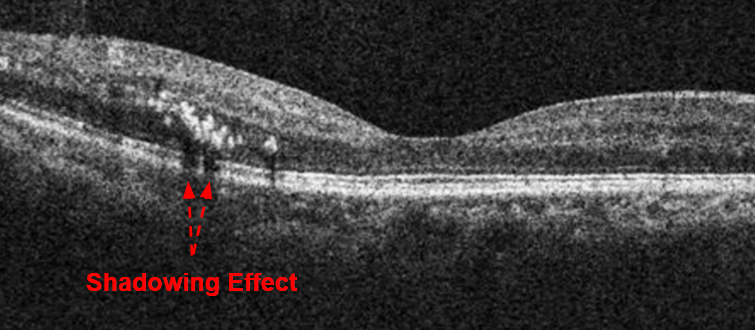
Hard Exudates
Localization to the middle of the retina makes the distinction of this lesion significantly easier with OCT. Depending on the density of the lipid deposition, a shadowing effect might be noted leading to relative hyporeflectivity of the retinal tissue below the exudate mimicking disruption of the outer retina.
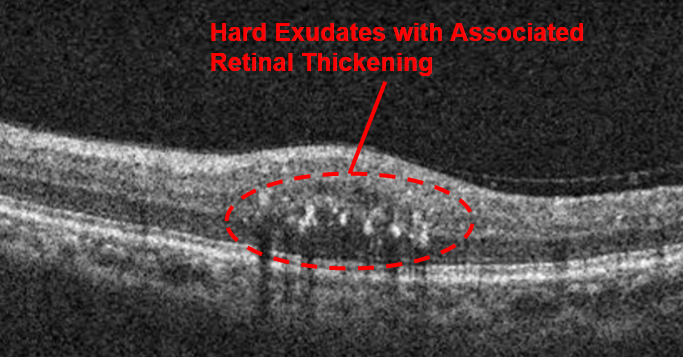
Hard Exudates
With correlation of fundus photos and OCT images with the Zeiss Cirrus Photo, differentiation of retinal white spots and dots is straightforward.
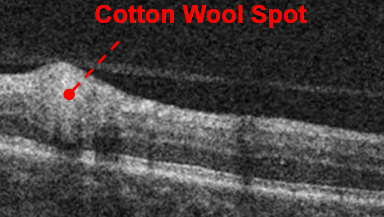
Cotton Wool Spot on Optical Coherence Tomography
Classically, cotton wool spot (CWS) have been thought of as microinfarctions of the RNFL. In the past decade, researchers have combined both clinical and histological evidence and have challenged that notion.
Cotton Wool Spot
New evidence suggests that CWSs are “localized accumulations of axoplasmic debris within adjacent bundles of unmyelinated ganglion cell axons.”14,15
Cotton Wool Spot
As the pathophysiological debate regarding CWSs continues, clinicians still need to differentiate CWSs from other lesions. A CWS is seen as a white indistinct retinal lesion. OCT reveals a localized RNFL thickening in the most anterior part of the image. Though sometimes ophthalmoscopically similar to drusen or exudates, a CWS is much more superficial to either of those lesions and thus easily distinguished with OCT. If CWSs are outside the Macular Cube Scan, Zeiss Cirrus allows for the easy change of retinal scan location by dragging the “scan box” to the zone of interest.
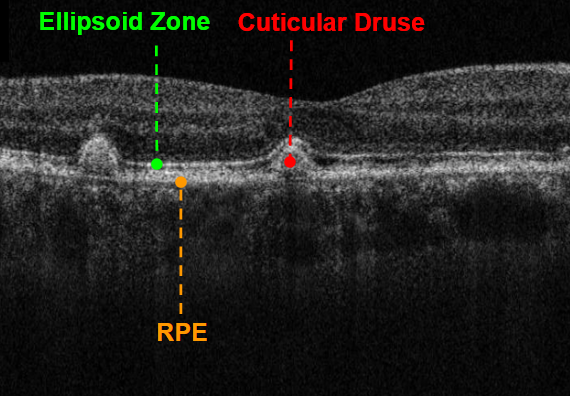
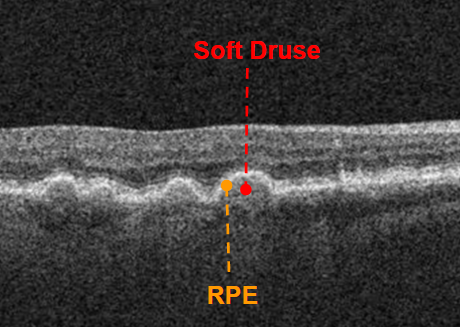
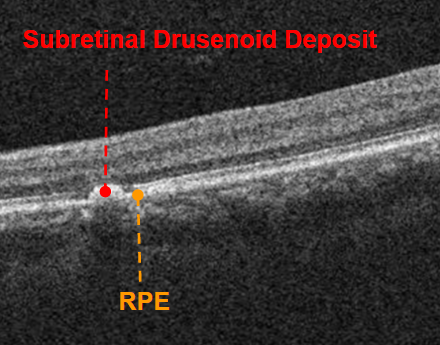
Drusen on Optical Coherence Tomography
“Drusen are focal deposits of extracellular debris located between the basal lamina of the RPE and the inner collagenous layers of Bruch’s membrane.”16 A more recently recognized entity, subretinal drusenoid deposits, are funduscopically and biochemically similar to drusen but have different anatomical locations.16
Drusen
Drusen range in size from pinpoint to greater than 1000 µm. Soft drusen are large accumulations of extracellular debris that look similar to PEDs on OCT. Soft drusen are located beneath the RPE, creating a dome-like hyporeflective elevation. Unlike PEDs which are optically empty, soft drusen will show some reflectivity within the lesion. Cuticular drusen are smaller and will be visualized as rounded triangular lesions below the RPE.
Drusen
When these lesions are larger, they will be hyporeflective on the inside but smaller cuticular drusen may be optically full and therefore hyperreflective. At the apex of cuticular drusen, the overlying RPE may be attenuated leading to increased light penetration into the choroid. Subretinal drusenoid deposits are visualized as hyperreflective lesions superficial to a mostly intact RPE. Depending on their size and color, drusen might mimic hard exudates or CWS but are easily differentiated with OCT due to their deep location within the retina.
Drusen
Longitudinal analysis of drusen can be achieved by looking at individual OCT images or by using the RPE Segmentation Map which gives an overall view of RPE morphology.
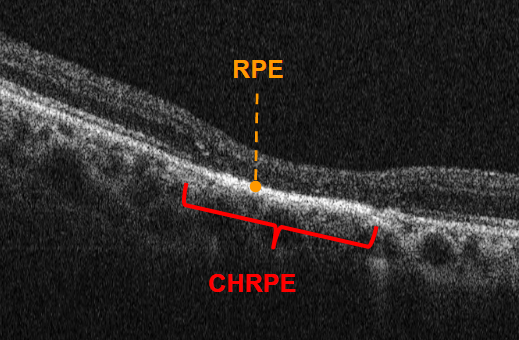
Congenital Hypertrophy of the Retinal Pigment Epithelium on Optical Coherence Tomography
“Congenital hypertrophy of the retinal pigment epithelium (CHRPE) is a benign, pigmented lesion located at the level of the RPE.”17 CHRPE lesions can present with areas of hypopigmentation known as lacunae which can grow in size with age.17,18,19
CHRPE : Photo Credits Dr. Jerome Sherman
Though sometimes ophthalmoscopically similar to choroidal nevi, an OCT image will allow easy differentiation of one lesion from the other. OCT images a CHRPE as a flat and irregular RPE lesion. The overlying retina, especially outer retinal layers, will be thinned.20 If the inner retina is relatively intact, there will often be a collapse of the inner retina leading to local concavity. Lacunae will present as RPE loss within the CHRPE; these areas will allow increased signal penetration and therefore improved visualization of deeper layers. The choroid is unremarkable in these lesions. As CHRPE are often extra-macular, the fixation of the Macular Cube Scan can be changed to image these lesions.
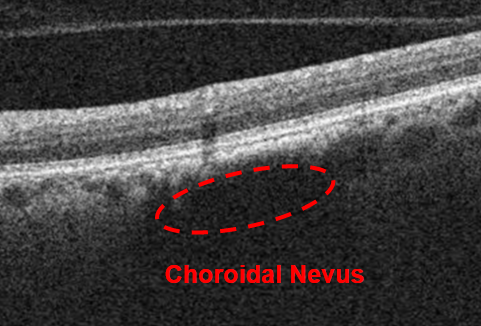
Choroidal Nevus on Optical Coherence Tomography
A choroidal nevus is a melanocytic lesion of the choroid which varies in size and pigmentation. Most often appearing as a regularly pigmented flat dark lesion, choroidal nevi may mimic other pigmented retinal lesions, especially if a stereoscopic view is difficult to achieve.
Nevus
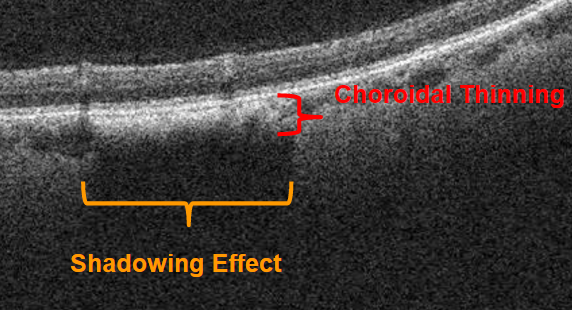
With OCT, choroidal nevi are visualized as smooth convex choroidal lesions with overlying choroidal thinning and significant deep choroidal shadowing.18,19,21
Nevus
A nevus shows up as a hyporeflective area within the choroid with the degree of hyperreflectivity varying with the degree of nevus pigmentation; a darker nevus will be more hyporeflective than a lighter pigmented nevus. There might be associated drusen, subretinal fluid, and/or outer retinal disruption.21
Conclusion
The combination of fundus photography and OCT imaging in a Zeiss Cirrus Photo makes differentiation and monitoring of choroidal nevi straightforward. One can look for changes in size on the fundus photo while looking for changes in retinal architecture with the OCT scan.
Whether it is staging ERMs and VMT, differentiating the types of macular holes, elucidating the reason for macular thickening, distinguishing white spots and dots, or discriminating between pigmented chorioretinal lesions, OCT is invaluable in the differential diagnosis of vitreal interface, retinal, and choroidal disease.
The
Zeiss Cirrus HD OCT and Zeiss Cirrus Photo both have the necessary imaging resolution, scan versatility, and ease of use to integrate into day to day clinical practice. As clinical data continues to be correlated with histopathological evidence, OCT will only become more useful within the eyecare practitioner’s armamentarium.
The statements of the healthcare professional whose opinion is contained in this material reflect only their personal opinions and experiences and do not necessarily reflect the opinions of any institution with whom they are affiliated. The healthcare professionals whose opinion is contained in this material does not have a contractual relationship with Carl Zeiss Meditec and not received financial compensation. Not all products, services or offers referenced in this article are approved or offered in every market and approved labeling and instructions may vary from one country to another. CIR.8291
Sources:
- Schuman, Joel S., et al., eds. Optical coherence tomography of ocular diseases. Thorofare, NJ: Slack, 2004.
- Staurenghi, Giovanni, et al. “Proposed lexicon for anatomic landmarks in normal posterior segment spectral-domain optical coherence tomography: the IN• OCT consensus.” Ophthalmology 121.8 (2014): 1572-1578.
- Spaide, Richard F., and Christine A. Curcio. “Anatomical correlates to the bands seen in the outer retina by optical coherence tomography: literature review and model.” Retina (Philadelphia, Pa.) 31.8 (2011): 1609.
- Duker, Jay S., et al. “The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole.”Ophthalmology 120.12 (2013): 2611-2619.
- Steel, D. H. W., and A. J. Lotery. “Idiopathic vitreomacular traction and macular hole: a comprehensive review of pathophysiology, diagnosis, and treatment.” Eye 27 (2013): S1-S21.
- Johnson, Mark W. “Posterior vitreous detachment: evolution and complications of its early stages.” American journal of ophthalmology 149.3 (2010): 371-382.
- Haouchine, Belkacem, et al. “Diagnosis of macular pseudoholes and lamellar macular holes by optical coherence tomography.” American journal of ophthalmology 138.5 (2004): 732-739.
- Scholl, Stefan, et al. “General pathophysiology of macular edema.” European journal of ophthalmology 21 (2010): S10-9.
- Bhagat, Neelakshi, et al. “Diabetic macular edema: pathogenesis and treatment.” Survey of ophthalmology 54.1 (2009): 1-32.
- Liegl, Raffael, and Michael W. Ulbig. “Central serous chorioretinopathy.”Ophthalmologica 232.2 (2014): 65-76.
- Yannuzzi, Lawrence A. “Type A behavior and central serous chorioretinopathy.” Transactions of the American Ophthalmological Society84 (1986): 799.
- Dansingani, Kunal K., et al. “En face imaging of pachychoroid spectrum disorders with swept-source optical coherence tomography.” Retina 36.3 (2016): 499-516.
- Ota, Masafumi, et al. “Optical coherence tomographic evaluation of foveal hard exudates in patients with diabetic maculopathy accompanying macular detachment.” Ophthalmology 117.10 (2010): 1996-2002.
- McLeod, D. “Why cotton wool spots should not be regarded as retinal nerve fibre layer infarcts.” British journal of ophthalmology 89.2 (2005): 229-237.
- Schmidt, Dieter. “The mystery of cotton-wool spots-a review of recent and historical descriptions.” European journal of medical research 13.6 (2008): 231.
- Spaide, Richard F., and Christine A. Curcio. “Drusen characterization with multimodal imaging.” Retina (Philadelphia, Pa.) 30.9 (2010): 1441.
- Fung, Adrian T., Marco Pellegrini, and Carol L. Shields. “Congenital hypertrophy of the retinal pigment epithelium: enhanced-depth imaging optical coherence tomography in 18 cases.” Ophthalmology 121.1 (2014): 251-256.
- Say, Emil Anthony T., et al. “Optical coherence tomography of retinal and choroidal tumors.” Journal of ophthalmology 2011 (2011).
- Shields, Carol L., et al. “Enhanced depth imaging optical coherence tomography of intraocular tumors: from placid to seasick to rock and rolling topography—the 2013 Francesco Orzalesi Lecture.” Retina 34.8 (2014): 1495-1512.
- Shields, Carol L., et al. “Photoreceptor loss overlying congenital hypertrophy of the retinal pigment epithelium by optical coherence tomography.”Ophthalmology 113.4 (2006): 661-665.
- Shah, Sanket U., et al. “Enhanced depth imaging optical coherence tomography of choroidal nevus in 104 cases.” Ophthalmology 119.5 (2012): 1066-1072.