



Rhegmatogenous retinal detachment (RRD) refers to the separation of the retina from the underlying retinal pigment epithelium (RPE) due to a retinal tear and subsequent subretinal fluid accumulation. Despite being one of the more common conditions retina specialists encounter, retinal detachments are relatively rare, with an incidence of approximately one per 10,000 patients, or about 28,000 cases/year in the US. When retinal detachment occurs, patients are at significant risk for permanent vision loss and legal blindness.
Patients who are suspected to have a RRD should be evaluated urgently by a vitreoretinal specialist. Patients at higher risk for RRD (e.g., high myopes, prior retinal detachment, family history) are advised to have a dilated examination on an annual basis. This allows the clinician to rule out and treat any sight-threatening retinal pathology, including lattice degeneration, atrophic holes, retinal tears, and subclinical retinal detachment.
There is no definitive timeline over which a retinal detachment can occur and some RRD cases may be initially asymptomatic. Patients may go days or weeks with a retinal break before presenting to their eye care practitioner with symptoms. Other patients may be more sensitive to subtle changes in their vision and present the same day for evaluation.
In cases of macula-involving RRDs, permanent functional damage occurs to the macular retinal tissue, making post-op visual prognosis variable. While the anatomical success rate for retinal reattachment surgery exceeds 90%, patients may develop persistent vision issues. Over half of these patients are initially left with persistent symptoms of distorted vision, metamorphopsia, or even monocular diplopia in the surgical eye. Some studies have shown even higher rates of post-op metamorphopsia, occurring in nearly 70% of all macula-off RRD cases, and may be persistent. Addressing this common visual outcome is crucial in the management of your retinal detachment patients.
The purpose of this article is to review the pathophysiology of retinal detachment, as well as the potential for metamorphopsia following repair.
Pathophysiology of retinal detachment (and metamorphopsia)
The retina is thin translucent tissue lining the back wall of the eye similar to delicate wallpaper on the inside of a sphere. The retina is held in place by a light adhesion and negative pressure between the neurosensory retina and RPE. The vitreous is a transparent gel composed of water, collagen, and hyaluronic acid that fills the middle of the eye and is adherent to the retina. Over time the vitreous liquifies and will eventually separate from the retina. Infrequently, during this process of separation, the vitreous may tear the retina. A retinal break may then allow liquid vitreous into the subretinal space, leading to a retinal detachment. As the outer retina relies on oxygenation from the choroid and maintenance functions from the RPE, photoreceptors undergo gradual apoptosis and retinal function becomes compromised. Furthermore, ischemia-induced inflammatory cytokines (e.g., IL-8 and TGFbeta) exacerbate outer retinal damage. The peripheral retina is minimally affected by this, whereas macular detachment may lead to permanent dysfunction. In macula-off RRD cases, duration is an important predictor of final visual outcome, with less than one week being most optimal.
Symptoms of retinal detachment
Rhegmatogenous retinal detachments are due to a retinal tear followed by the accumulation of subretinal fluid. Acute symptoms of a retinal tear often include spontaneous crescent-like peripheral photopsia (i.e., lightning strikes) and prominent new floaters, and a detachment will cause a curtain-like vision loss (in the opposite visual field of the pathology). Surprisingly, some patients assume the symptoms are benign and may present days to weeks later.
Despite high surgical success rates, RRD repair remains a gross process. If the center of the retina is involved in the detachment, patients will have a variable degree of permanent vision loss, again related to the duration of detachment. In addition to reduced visual acuity or blurring, patients with macular involvement also have a risk for metamorphopsia (i.e., distorted central vision) even following successful repair. Affected patients complain of distortion, doubling, or “slanting” of central vision in the affected eye. This will be more prominent when the other eye is occluded, and may be more prominent with near visual tasks. Metamorphopsia can be difficult to evaluate and quantify as affected eyes may have excellent visual acuity. Amsler grid monitoring can help to document the severity, and imaging can document anatomic changes that may contribute.
Less commonly, some patients will have abnormal post-operative vision due to differences between the pre- and post-operative retinal position. This is termed “retinal shift,” and is analogous to replacing wallpaper that has fallen off a wall. You can place the wallpaper back on the wall, but it may not have the same exact location as before. This scenario is more common in cases with giant retinal tears, or in the presence of substantial residual subretinal fluid (SRF). Retinal shift is also more prevalent in cases where the patient was unable to strictly follow the postoperative positioning requirements. Postoperative SRF and/or a disruption to the external limiting membrane (ELM) are independent predictors of metamorphopsia, and are associated with poorer visual outcomes at 12 months post-op.
Affected patients often have visible retinal “microfolds” near the low water mark, with small outer retinal folds visible on OCT and autofluorescence. Microfolds are visible as thin hypopigmented lines on exam, and as small hyper-reflective dots in the outer retina on OCT. These often resolve spontaneously over several months. In some cases, retinal shift is only visible with fundus autofluorescence, revealing hyper-autofluorescent lines that indicate where blood vessels were previously.
Retinal shift, while not fully unavoidable, can be minimized with surgical technique. Pneumatic retinopexy has a lower incidence of metamorphopsia following RD repair, likely due to the slow, “natural,” rate of SRF resorption. Positioning is critical. As there is commonly a small amount of residual SRF following surgical repair, patients should be advised to temporarily position themselves with the tear in the most gravity-dependent position. This is counter-intuitive as we typically require the patient to position in the exact opposite way, but this can allow a few hours for residual fluid to egress in the appropriate direction. Face-down positioning is also a way to use the bubble to tamponade the macula and push fluid elsewhere. During surgery, the use of the heavy liquid perfluorocarbon can also be used to push subretinal fluid back out through the retinal break and minimize residual SRF.
Treatment for microfolds is commonly observation, with slow, spontaneous resolution over many months. Larger folds may require surgical intervention with repeat vitrectomy, injection of subretinal fluid in the area of the fold, and gas-fluid exchange with strict post-operative positioning. An alternative is to treat post-operative diplopia with prism glasses and/or strabismus surgery.

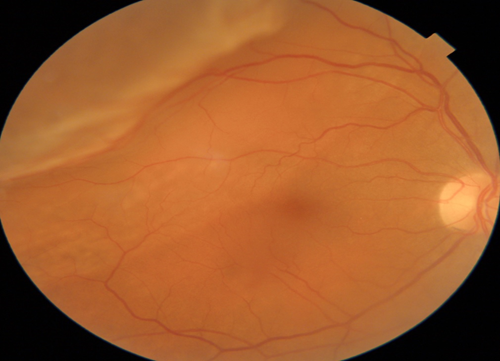
Figure 1: Macula-splitting rhegmatogenous retinal detachment OD shown in 62 y/o female. This patient had visual symptoms of flashing lights and shadows for almost eight weeks before presenting for evaluation. Patients with pre-operative macula-off status are over three times as likely to experience postoperative symptoms of metamorphopsia. Photo courtesy of Kevin Cornwell, OD
Expectations after surgery
Despite our best efforts, some patients still suffer from post-operative symptoms like metamorphopsia or monocular diplopia. For these patients, I will reassure them that the retina looks very healthy overall and that over half of cases will significantly improve over the next several months. This can be a difficult sell in some instances. I remind my patients not to give up hope, and sometimes even to expect residual mild symptoms for up to 24 months. I have wonderful memories of affected patients coming in a year or two later with big smiles on their faces as their vision had now returned to normal.
Extensive patient education and monitoring through serial OCT imaging is a good starting point in the management of metamorphopsia cases. If you are co-managing with another surgeon, you may need to refer back to their team for evaluation in cases with unresolved, symptomatic postoperative metamorphopsia. Remember, these visual symptoms can persist for months after surgery, typically improving within one year.
Since postoperative refractive outcomes can be variable, a thorough refraction may help to alleviate visual symptoms of metamorphopsia. In cases of high anisometropia, contact lenses can be a viable option to avoid spectacle magnification/aniseikonia and can provide satisfactory binocular vision.
As highly trained eye care practitioners with surgical subspecialties, it is important to remember that our patient is more than just a retina, optic nerve, or cornea. The whole process of retinal detachment and subsequent repair can leave patients feeling anxious and uncertain about their future visual function. Conveying realistic expectations on postoperative visual symptoms will help instill confidence in patients, while also building rapport with you and your team. Understanding metamorphopsia and spending an extra few moments explaining it to your patient can make all the difference in their experience with you.
